
Abstract
Powassan virus is a rare flavivirus that may be transmitted by tick bite and is associated with encephalitis. Infections have been described in the northern United States, Canada, and Russia. We present the case of a 56-y-old man who presented to our hospital with symptoms of confusion, altered behavior, and headache. The patient developed fever and status epilepticus despite supportive care and required endotracheal intubation. Six days before presentation, the patient had returned from a hunting trip in the Adirondack region of New York State.
Introduction
Powassan virus (POWV) is a zoonotic flavivirus endemic to the Northeastern and Great Lakes regions of the United States, Canada, and Russia and is capable of causing lethal encephalitis in approximately 10% of cases. 1 POWV was first isolated by McLean and Donahue in 1958 on brain biopsy of a 5-y-old boy in the town of Powassan, Ontario. In this first verified case, the patient’s initial presentation of fever of 39.4°C and drowsiness quickly progressed to unresponsiveness with left-sided hemiplegia and finally respiratory arrest on Day 4 of hospitalization. 2 At the time histologically indistinguishable from other known viral encephalitides such as St. Louis encephalitis, Japanese B encephalitis, and Western Equine encephalitis, POWV was ultimately isolated using a series of antisera neutralization techniques. To date, 2 distinct genetic lineages of POWV have been identified, known as lineage I POWV (POW-L1) and lineage II POWV (POW-L2), also referred to as deer tick virus. 3
Epidemiological surveys have identified several different tick taxa acting as vectors for POWV, each with a unique geographic distribution, including Ixodes scapularis (Northeastern United States), Ixodes cookei (Midwest United States, Canada), and Haemaphysalis longicornis (Russia). To date, at least 3 unique enzootic cycles in which the virus is maintained in a nonhuman reservoir have been identified. POW-L1 is maintained between Ixodes cookei and groundhogs/skunks and between Ixodes marxi and red squirrels. POW-L2 is vectored between Ixodes scapularis and white-footed mice. 4 Reported cases of Powassan encephalitis (PE) have steadily increased over the last several decades, a fact that may be due in part to improved recognition and diagnostic techniques. From 1958 through the mid-2000s there were 40 to 45 verified cases of PE in North America, diagnosed primarily by neutralization titer testing. 4 The Centers for Disease Control reports that approximately 114 cases of PE have been reported in the United States between 2008 and 2017. The states with the highest number of cases include Minnesota (25), Wisconsin (20), New York (17), and Massachusetts (13), as reported by local health departments. 5 Today, the virus can be detected by isolating IgM antibody by capture immunoassay of cerebrospinal fluid (CSF), a fourfold rise in serum antibody titers against the virus, or isolation of viral antigen or genomic sequences from tissue, blood, or CSF. 6 In many cases, the virus itself cannot be isolated; however, increased neutralization titers indicate its presence.
Viral infections of the central nervous system can manifest on a spectrum ranging from mild aseptic meningitis to severe encephalitis, as seen in our patient. Although PE has only been recognized in fewer than 200 cases in its brief 60-y history, the rapid clinical deterioration seen in cases such as this one demand that clinicians practicing in endemic regions be comfortable recognizing this illness. 4
Case Report
Our case regards a previously well 56-y-old Caucasian male with a medical history only significant for mild asthma and diet-controlled hypertension. Six days before his initial hospital presentation in early November 2017 he had been on a 3-night hunting trip in the Adirondack Mountains of northeastern New York. After returning from his hunting trip, the patient began to experience a mild headache that gradually worsened. On the morning of his hospital admission, he was noted by his wife to have trouble dressing, to seem acutely confused, and to complain of new-onset blurred vision. In addition, he was observed to have 24 h of decreased appetite and a single episode of emesis.
The patient presented to an urgent care, from which he was referred to the emergency department of our hospital. He was found to be oriented only to his name, which he was able to recall with difficulty and obvious frustration. His speech was fluent, behavior was appropriate, and he denied pain, weakness, or shortness of breath. On initial evaluation he was found to have a temperature of 38.1°C with an otherwise unremarkable physical examination. A noncontrast computed tomography scan of the head was performed and revealed no acute abnormalities. Lumbar puncture revealed an elevated white blood cell count to 218 cells·mL-1 with 92% lymphocytic predominance (Table 1). Normal glucose and protein levels were noted. The presumed viral central nervous system infection was empirically managed with intravenous acyclovir, and the patient was admitted to the hospital in stable condition. The CSF and serum specimens were collected and sent for analysis. Magnetic resonance imaging (MRI) studies of the patient’s brain on Day 1 of admission revealed only signs of chronic microvascular ischemic changes.
CSF analysis from lumbar puncture on day of emergency department evaluation
CSF, cerebrospinal fluid; RBC, red blood cell; WBC, white blood cell.
Over the next 24 h, our patient’s mental status continued to decline to a lethargic, minimally interactive level, accompanied by worsening fever to 39.5°C and new-onset hypertension up to 190/109 mm Hg. Electroencephalography displayed a failure to develop a dominant posterior rhythm, brief periods of electrocerebral silence, and generalized background slowing consistent with diffuse severe encephalopathy. At this point, the patient was transferred to the medical intensive care unit for closer monitoring, where he was noted to display persistent seizure activity. Over the course of our patient’s third hospital day, both his fever and hypertension were refractory to medical intervention, and he developed status epilepticus requiring intravenous sedation and endotracheal intubation. Subsequently, he was transferred to a regional tertiary care center for admission to a dedicated neurological intensive care unit.
After facility transfer, the patient received supportive care in the neurological intensive care unit for a total of 3 d. New-onset right-sided weakness was also appreciated on examination. Repeat MRI was collected and showed new findings of increased fluid attenuated inversion recovery hyperintensity about the cerebral convexities and cerebellar folia (Figure 1), as well as leptomeningeal enhancement suggestive of meningitis or other inflammatory process. Acyclovir was discontinued after herpes simplex virus and varicella zoster virus were ruled out. After 3 d of intensive care unit support, our patient’s neurological examination began to stabilize and his strength became symmetric. After gradual recovery over 5 d on the medical floor, the patient was discharged to a subacute rehabilitation facility, where he remained for 8 d. He was subsequently discharged to home back at his baseline functional status. His only discharge medication was a several-week course of prophylactic levitiracetam, which was subsequently discontinued upon outpatient neurologic follow-up. After hospital discharge, his serum arbovirus serology was found to be reactive. Powassan IgM was noted on enzyme-linked immuno-assay (ELISA) and microsphere immunofluorescence assay (MIA). Interestingly, West Nile virus had positive cross-reactivity on MIA but was found to be nonreactive on ELISA (Table 2).
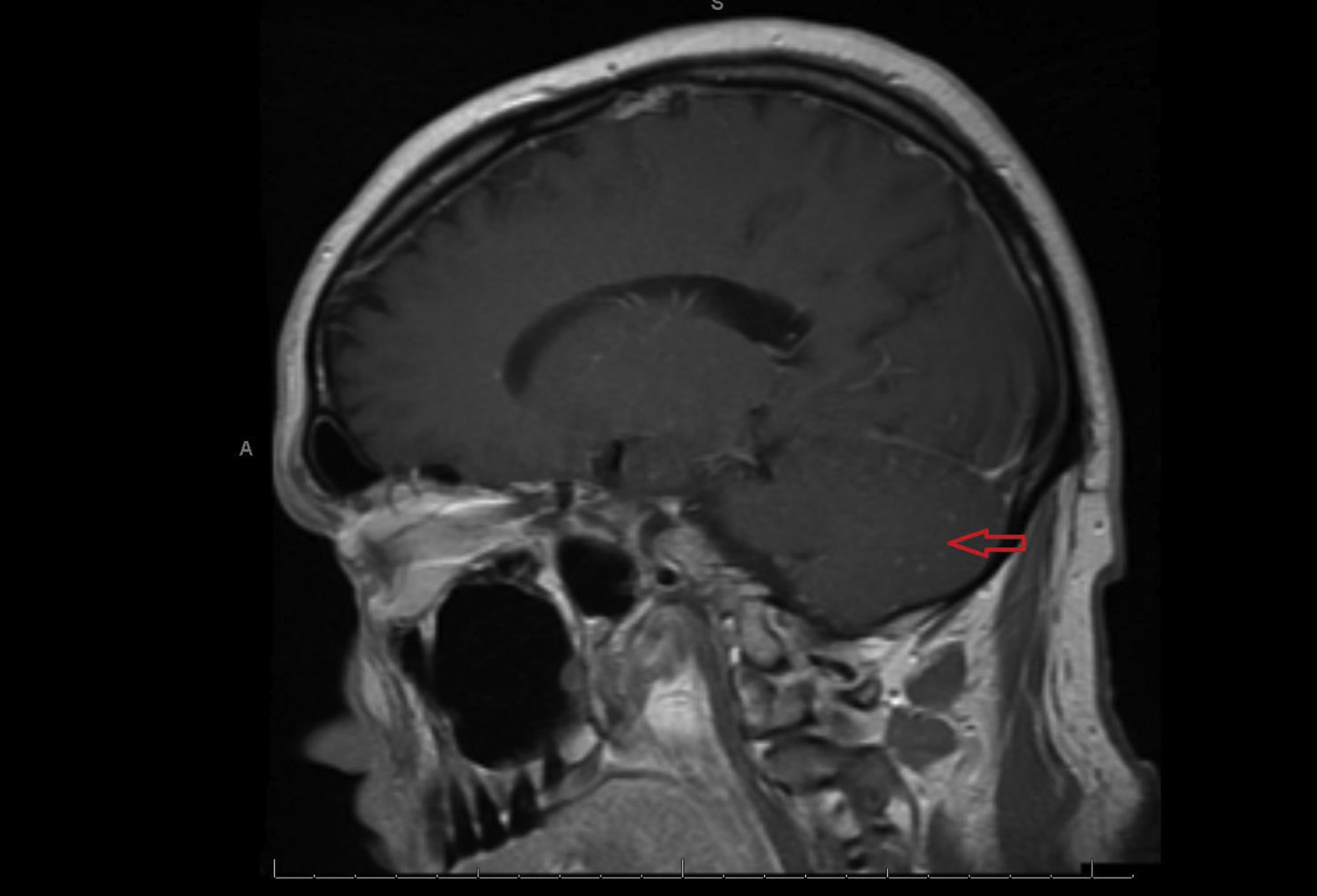
Diffuse fluid attenuated inversion recovery signal abnormality noted in the cerebellar fossa on sagittal T1 magnetic resonance imaging.
Results of serum and cerebrospinal fluid tests
CSF, cerebrospinal fluid; ELISA, enzyme-linked immuno-assay; HSV, herpes simplex virus; MIA, microsphere immunofluorescence assay; rt-PCR, real time polymerase chain reaction.
Discussion
In reviewing our patient’s disease course, his experience mirrors that of most other documented PE cases over the past 60 y. First, his acquisition of the virus presumably occurred in the mountains of Northeastern New York, a well-studied habitat of Ixodes scapularis. 7 As seen in other cases, the patient did not recall experiencing a tick bite, and unlike Lyme disease, POWV infection does not trigger any characteristic skin lesion. Second, the incubation period in this case was approximately 9 d: 3 d of exposure followed by 6 d at home before hospitalization. This aligns with the known 8 to 34 d typical incubation period of the virus. 1 Third, his viral prodrome of confusion, headache, fever, and emesis followed by rapid symptomatic progression and clinical deterioration to hemiparesis, seizure, and unresponsiveness mimic the typical presentation of PE. 8 In addition, the leptomeningeal enhancement and increased fluid attenuated inversion recovery findings from our patient's MRI have been reported in other cases of PE requiring intubation. 9
As is typical in viral encephalitis, confirmatory microbiologic diagnosis in this case was not made until the patient was through the most acute phase of his illness. In our case, the patient had serologic and CSF testing conducted via both hospital and third-party national laboratories. Ultimately the diagnosis was made by serologic IgM ELISA and MIA from the hospital laboratory. The only successful isolation of the virus on genetic polymerase chain reaction testing came from the national laboratory. Cross-reactivity with other members of the flaviviridae subgroup, in this case West Nile virus, has been well documented in previous cases of PE. 10
In the last 20 y, the spread of Ixodes scapularis into northwestern Minnesota, central Michigan, the Ohio river valley, and inland from the southeastern and gulf coasts has been well documented. 7 Although education and tick bite prevention are still the best defense against infection with POWV and other tick-borne illnesses, the potential for rapid clinical decline and need for urgent tertiary care support should keep these rare cases on the differential for all physicians practicing in the Eastern United States. Physicians venturing to the austere environment in endemic regions and those who care for patients returning from these regions should be aware of POWV and its characteristic presentation.
Footnotes
Acknowledgements
Author Contributions: Concept, design, manuscript, and patient care: DC and SP.
Financial/Material Support: None.
Disclosures: None.