
Abstract
Introduction
Educational materials are important tools in the prevention of altitude illness among individuals traveling to high altitude destinations. Travelers obtain information about altitude illness from many different educational resources. Our objective was to determine which educational resources for altitude illness prevention were used by trekkers on the Everest Base Camp trek and Annapurna Circuit. We also sought to compare which resources were used by individuals from different geographic areas.
Methods
A survey was administered to trekkers attending an altitude illness information lecture at the Himalayan Rescue Association clinic. Trekkers provided their basic demographic information and educational resources they used while preparing for the trek. Comparisons were made between trekkers based on the resources they used, as well as their age and country of origin.
Results
Of 1075 surveys administered, 906 were completed. Internet sources were most commonly used by trekkers (49%), followed by friends or family (22%), and healthcare providers (18%). The age of participants using Internet sources was 36 ± 12 y (mean ± SD), lower than those who did not use Internet sources (39 ± 14 y, P < 0.01). Participants came from 8 geographic areas; Europe (55%), North America (24%), and Oceania (11%) made up the vast majority. Compared to the overall cohort, participants from Oceania demonstrated more Internet reliance at 65% (χ2(1, n = 102)=9.7, P < 0.01).
Conclusions
In this group of trekkers in the Himalayas, the Internet was the most common source of information on altitude illness prevention and management. Trekkers using Internet sources were slightly younger than non-Internet users.
Introduction
Travel to high altitude environments has become increasingly popular in recent years. In 2016, more than 750,000 people visited Nepal, many of them taking part in mountaineering or trekking expeditions. Trekkers are at high risk of developing altitude illness. The reported incidence of acute mountain sickness (AMS) among foreign visitors to the Himalayas of Nepal has varied widely, between 22 and 68%, depending on the location, date, and ascent rate of study participants. 1 –3 Some also develop more life-threatening illness, with incidence of high altitude pulmonary edema and high altitude cerebral edema reported at 0.5 to 15% and 1.3 to 1.8%, respectively.1,3 With increased travel to the area, it has become important for trekkers to have access to reliable and accurate educational materials related to the recognition and prevention of altitude-related illness. 4 Although it is unclear if trekkers’ knowledge is actually increasing,2,5 improved understanding of altitude-related illness, adherence to appropriate ascent rates, and use of prophylactic medication have been shown to decrease the incidence of AMS.2,6 This suggests that there is great potential to improve illness prevention by increasing the availability of information to trekkers as they prepare to enter areas of high altitude.7,8 Fortunately, with the expansion of Internet services and improved understanding of AMS, there have never been more resources available to trekkers during their preparation.
The purpose of this study was to determine which educational resources were used by trekkers on the Everest Base Camp trek and Annapurna Circuit. We also sought to determine whether there were any significant differences in age or geographic distribution when comparing educational resources used.
Methods
Data used in this study were collected for internal process improvement at the Himalayan Rescue Association (HRA) and later used by the authors of this study for post hoc evaluation, with permission from the HRA. Data were anonymized without names or identifying personal information, and the subjects were not contacted to gather any additional information.
Informational sessions were held at HRA clinics during trekking seasons at Pheriche along the Everest Base Camp trek in fall of 2013 and at Manang along the Annapurna Circuit in spring of 2015. These sessions discussed altitude illness awareness, prevention, and treatment and were advertised and open to all trekkers. At the conclusion of these sessions, trekkers were asked to complete an anonymous survey about which sources they used to gain information about altitude illness prevention. Participants were asked to record basic demographic information, which included age, sex, and country of origin. All participants were sorted into geographic areas of origin: Europe, North America, Oceania, Asia, Middle East, Africa, South America, and other. They were also asked to specify in an open-ended question format which sources they used in preparation of their treks. Each of their survey responses was grouped into 1 of 12 categories of information sources. Participants who did not complete all of the demographic questions or specify at least 1 source of altitude illness information were excluded.
All collected data were entered into a Microsoft Excel spreadsheet with statistical comparisons made using a 2-sample t test and χ2 test. Data are presented as mean ± SD, and χ2 values are reported with number of responses and degrees of freedom.
Results
Of the 1075 surveys collected from trekkers, 906 (84%) were complete and used for data analysis. Of the included surveys, 712 were from the Pheriche clinic in 2013 and 194 were from the Manang clinic in 2015. Survey participants came from all 8 predetermined geographic areas: Europe (55%), North America (24%), Oceania (11%), Asia (6%), Middle East (2%), Africa (1%), South America (< 1%), and other (< 1%; Table 1).
Self-reported regions of origin of trekkers participating in the altitude information source survey and percentage of each region with respect to the total population
Internet sources were the information resources most commonly used by trekkers, with 48% of all participants reporting Internet use as a source of information prior to their treks. Friends and family were used as a resource by 22% of individuals, and a healthcare provider was used by 18% (Figure 1).
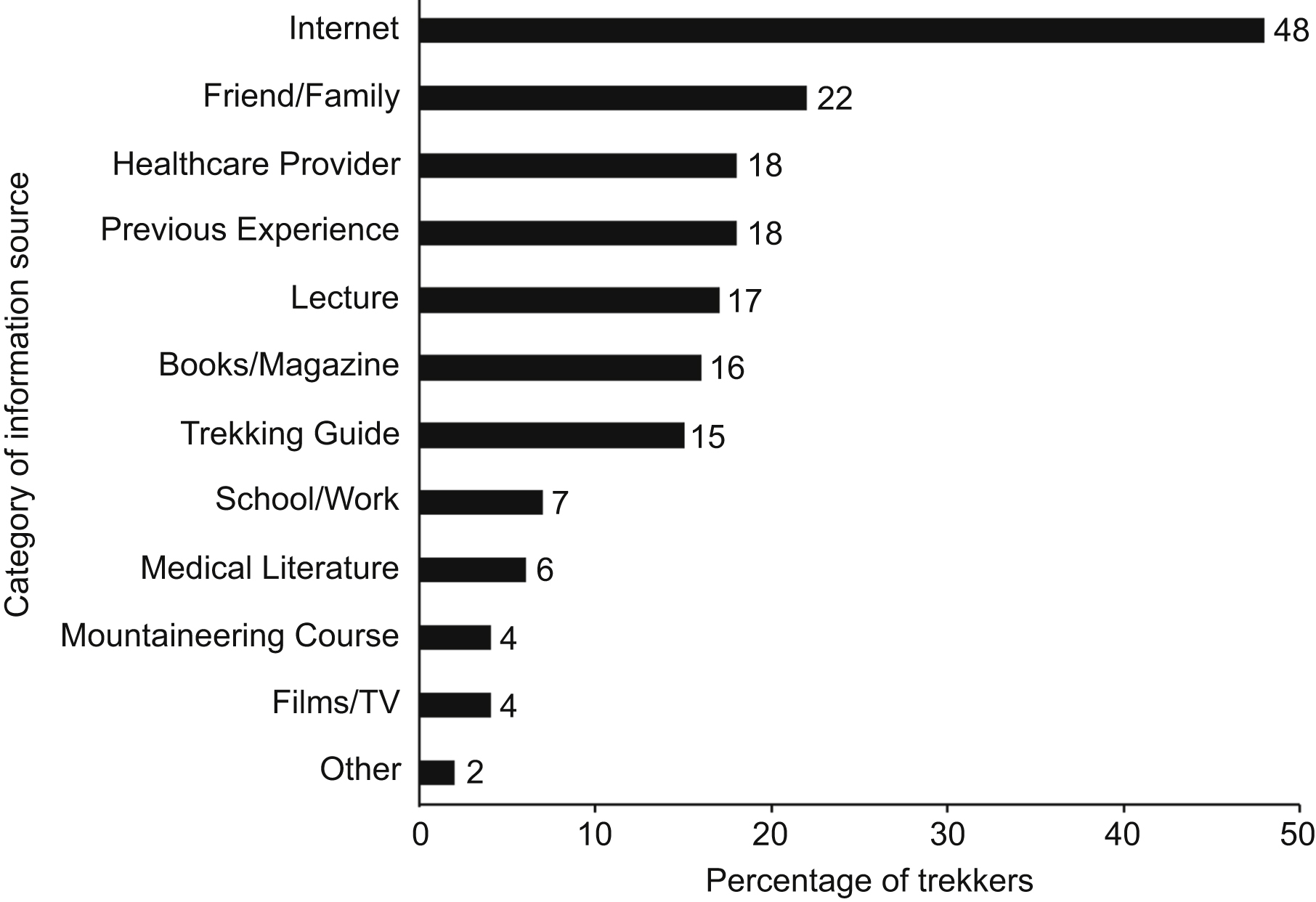
Percentage of individuals who specified a specific type of education resource that they used during preparation for their trek.
We also found with statistical significance that the age of participants who used the Internet as an educational resource was 36±12 y. This was slightly lower than the mean age of participants who did not use Internet sources, which was 39 ± 14 y (Figure 2).
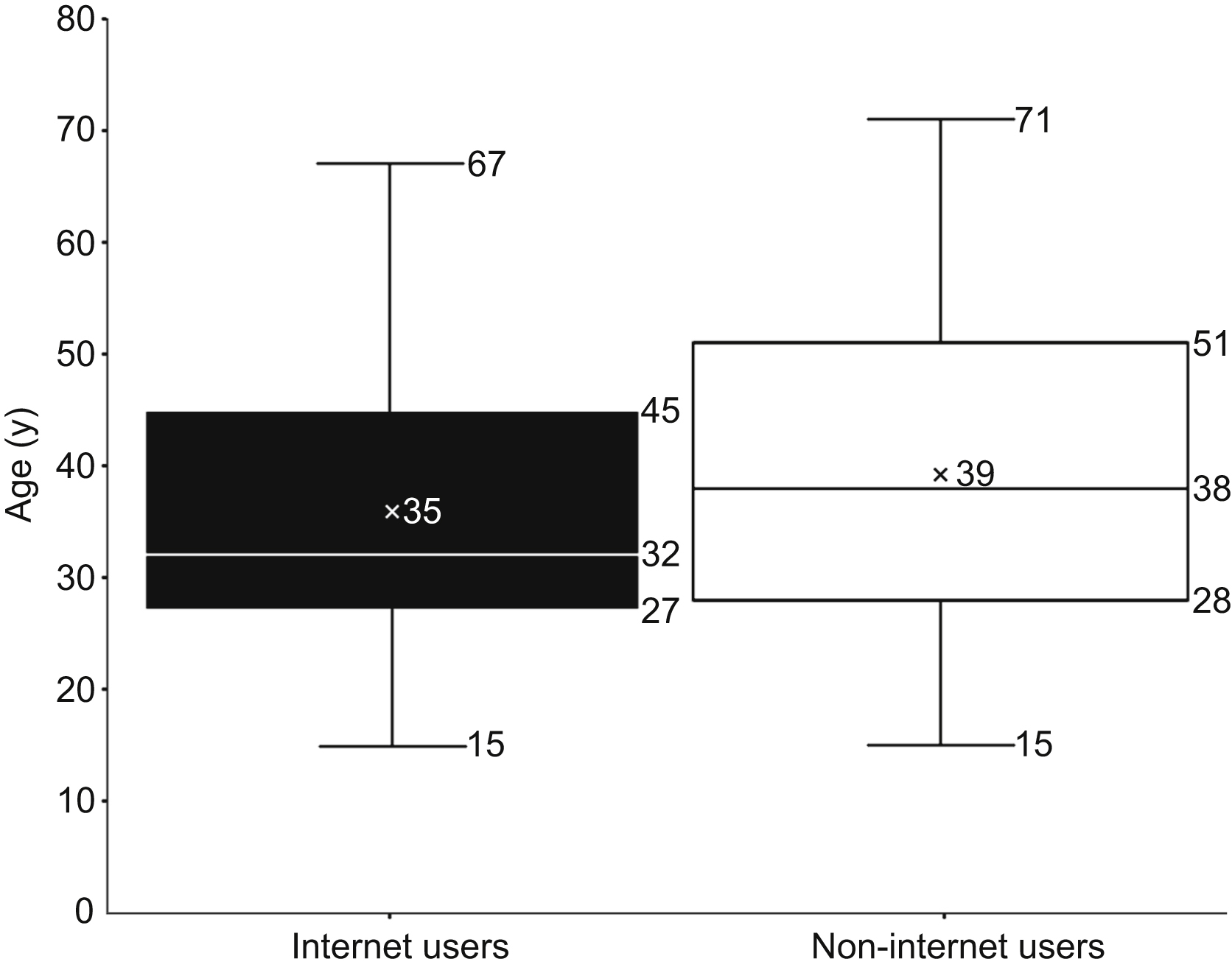
Age of participants who indicated they received altitude illness information from Internet sources compared to age of those who did not use Internet sources.
Additionally, the data showed that the distribution of resources used was generally similar when each geographic cohort was compared. Using χ2 goodness of fit analysis among geographic groups, we found more frequent Internet use in Oceania compared to the overall trekking population, with 65% individuals using the Internet as a resource (χ2(1, n = 102)=9.7, P < 0.01).
Discussion
We found that the majority of the individuals who participated in the survey travelled from countries in North America, Europe, and Oceania (Australia and New Zealand). This demonstrates the popularity of trekking in the Himalayas among people from these developed countries. We also found that the Internet was the most commonly used educational resource for individuals preparing for their trek in the Himalayas. Individuals using this source were slightly younger than the general trekker population, although this difference is of unclear importance. Although it may suggest that Internet sources have been adopted by trekkers of all ages, it could also reflect a generational change in how trekkers obtain their information. The prevalence of Internet access and ease of finding information through advanced search engines makes online sources attractive for individuals who seek quick access to up-to-date information. However, the wilderness medicine community must promote high-quality and accurate health content if the Internet is to realize its full potential as an accessible and accurate healthcare resource.
Internet information sources offer a number of advantages over traditional printed information sources, but perhaps the most important of these is accessibility. Printed materials feature content that is often difficult to locate, uses complex language, or is expensive to purchase. Online search engines allow users to overcome these obstacles through easy-to-use tools and rapid return of results.
However, this improvement in access is not without its disadvantages. Search engine queries link to sources that are automatically indexed without any formal curation and therefore do not always carry reliable, verifiable, or appropriate information.4,9 Further complicating this problem is that not all Internet users are able to distinguish between high- and low-quality information. 9 This contrasts with books, lectures, and medical literature, which are scrutinized for accuracy and reliability prior to publication. Despite their advantages in reliability, these traditional sources were significantly less used by trekkers in this study, regardless of age.
These conclusions raise an important question: If medical literature and expert knowledge are the most accurate resources, how can physicians and medical educators ensure that quality information reaches patients and potential travelers? Overall knowledge of AMS and its prevention is lacking among high altitude travelers, and adequate education can reduce the incidence of AMS.5,10 Physicians and medical experts remain the most trusted sources of information, and although the Internet has increasingly been used to obtain medical information, these providers play a vital role in patient education. Therefore, it is important that healthcare providers encourage trekkers, guides, and outfitters to scrutinize their online searches and help direct them to sources of evidence-based information. As trekking becomes more popular among younger individuals, more effort should be put into developing and promoting online resources that give high-quality information while focusing on accessibility to their users.
LIMITATIONS
This study relied on collecting data from individuals attending HRA clinic altitude illness lectures during a specific time period, resulting in a convenience sample. Given that numbers of trekkers vary depending on the year and not all trekkers attend altitude illness lectures, the included participants are not likely to represent all trekkers in the Himalayas. Data were collected from 2 different sites and 2 different years, and the sources used by trekkers may be different at the present time. Additionally, the survey was written in English, which may have resulted in overrepresentation of individuals from English-speaking countries. This survey was also written for internal use by the HRA, and we were unable to change questions to collect a broader range of patient information. Finally, although the mean age of Internet and non-Internet users is statistically significant, the large sample size may have created an overpowered test, which could incorrectly identify a relationship between age and Internet use.
Conclusions
Among the trekkers we studied, there was an overall preference for Internet resources as educational materials for AMS prevention. Trekkers who used the Internet as a source tended to be younger than those who did not. Because the Internet allows for improved accessibility of information, emphasizing high-quality sources may improve education and potentially reduce altitude illness in the trekking population.
Footnotes
Acknowledgments
We acknowledge the help and support of the Himalayan Rescue Association for their assistance in data collection.
Author Contributions
Study concept and design (BS, NC); obtaining funding (NC); acquisition of the data (NC); analysis of the data (BS, NC); drafting of the manuscript (BS); critical revision of the manuscript (BS, NC); and approval of final manuscript (BS, NC).
Financial/Material Support
None.
Disclosures
None.