
Abstract
This article describes 3 incidents in which therapeutic or experimental warming of cold individuals caused first- to third-degree burns to the skin. Mechanisms for these injuries are considered. We conclude that active external rewarming of the trunk of a cold patient in the field can be administered safely and burn risk reduced if 1) manufacturer instructions are followed; 2) insulation is placed between the skin the and heat source; and 3) caregivers make regular efforts to observe heated skin for possible pending burn injury. Direct inspection is mandatory for the skin of areas that are on top of a heat source when the patient is lying on the heat source.
Keywords
Introduction
Basic prehospital treatment for accidental hypothermia includes removing the victim from the cold exposure, removing wet clothing if the victim can be protected from the cold, and insulating and applying heat (if available) to the patient’s torso, all preferably following the principles of gentle handling and maintaining a horizontal position as much as possible. 1 –3
A great deal of work has been done to demonstrate the efficacy of many active external warming sources, such as chemical (gel or dry) heat packs or blankets, electrical and charcoal heat pads or packs, warm water bottles or bags, and even portable forced-air warming devices. 4 –6 As long as the heat is focused on the torso and does not involve warm water immersion (eg, a bathtub or shower in a remote cabin) or dry heat (eg, an open oven, fire or fire-heated rocks), prehospital warming is generally accepted as safe. The limited amounts of heat provided by field heat sources will not put the victim at risk of cardiac arrest, ventricular fibrillation, or other symptoms of circumrescue collapse. 2 ,3,5,7
One risk that has received minimal attention is potential burning of the skin during warming. It is generally believed that following manufacturer instructions, which usually include placing some insulating material between the skin and heat source, will provide adequate protection from burns; this is not a guarantee, however. Although burns during rewarming seem rare, a recent incident (see Incident 3) prompted the authors to rethink the importance of burn prevention during care of the cold patient. Therefore, we present 3 incidents in which first- to third-degree burns were caused by active heating of either a clinical patient or research subjects; the last 2 incidents occurred during laboratory studies that were approved by the University of Manitoba research ethics committee.
Reports
Incident 1
On a hot summer day in 1982, a lightly dressed 9-y-old boy (1.34 m tall, weight 28 kg, 1.02 m2 body surface area) was with his parents on a snowfield in the region of Zermatt, at an altitude of approximately 3000 m. He fell through an ice bridge over a glacier stream and into the water. His parents located him and immediately alerted the Swiss rescue system (Rega Air Ambulance). The boy was located by rescue personnel within 30 min of immersion, and another 35 min was required for extraction. At this point he was in deep hypothermic cardiac arrest (asystole) with dilated, nonreactive pupils. Thirty minutes of resuscitation (cardiopulmonary resuscitation and intubation) was immediately carried out onsite but without success. He was then flown directly to the University Hospital in Bern on a 110-min flight. During the flight the team tried to warm him with hot pads applied directly to his anterior torso for ∼ 90 min (specific information relating to the type of the heat source is not available from the medical records).
On arrival at the University Hospital of Bern, after being in a low flow state for ∼ 140 min, he was in ventricular fibrillation. Before being put on cardiopulmonary bypass he had an esophageal temperature (Tes) of 21°C, blood pH of 6.8, and potassium level of 3.4 mmol·L-1 (the low pH may be partly explained by the very high PaCO2 of 131 mm Hg, and the low potassium may be a dilutional effect from multiple infusions). The boy was immediately taken to the operating room for cardiopulmonary bypass rewarming, 8 which was successful (return of spontaneous circulation occurred 52 min later at a Tes of 29.7°C), followed by a remarkably easy postrewarming hospital course. He was extubated and fully responsive with normal reflexes 4 h after intensive care unit (ICU) arrival. He stayed in ICU for 3 d because of bilateral pleural effusions.
However, the boy had second- to third-degree burns on the torso where the hot pads had been applied (Figure 1). These were treated conventionally. Eight days after discharge from the pediatric department of the university hospital, the patient was transferred to his hometown in France, where he needed further hospitalizations for 68 d and required several operations for his burn treatment.

Second- to third-degree burns from hot pads applied directly to the skin during the transportation to the university hospital where the 9-y-old patient was rewarmed by cardiopulmonary bypass through a sternotomy (covered by the dressing).
Incident 2
A pilot study was conducted in 1998 on an adult male subject who was cooled in 8°C water to a Tes of 36°C (unpublished observations). Core rewarming was attempted with a negative pressure warming device used previously in hypothermic surgical patients. 9 The device included a water-perfused blanket applied directly to 1 forearm. The forearm and blanket were then inserted into a rigid cylinder, which was sealed around the arm so negative pressure (−30 to −40 mm Hg) could be applied to the forearm and hand (inflow water temperature gradually increased from 42 to 46°C; Figure 2). This device was a prototype for the Thermostat warming device (Aquarius Med, AZ). 10
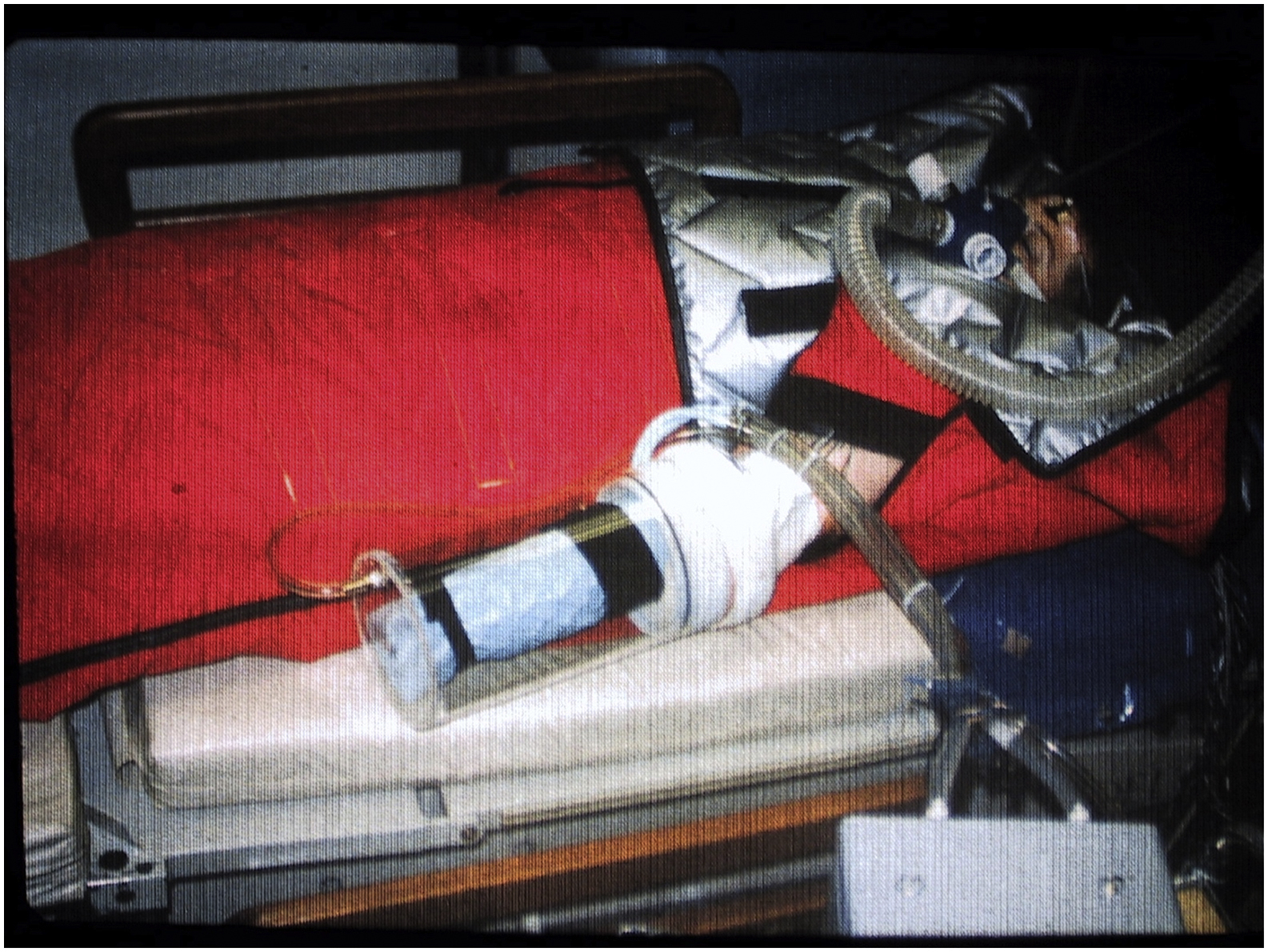
Apparatus for prototype negative pressure warming system applied to 1 arm.
The premise of the device was that negative pressure would mechanically counteract the thermoregulatory vasoconstriction in the arm, such that heat provided by the water blanket could be transferred back to the heart via the venous circulation, causing core warming. This general strategy was shown to be effective when arteriovenous anastomoses were opened during immersion of all 4 distal limbs in warm (45°C) water. 11 However, mixed results have been seen with negative pressure warming applied to only 1 distal limb (the arm). 9 ,10,12 After 155 min of warming, with no increase in core temperature, the blanket was removed, revealing first-degree burns in the pattern of the blanket tubing (Figure 3). The burn spontaneously resolved over the next week, and the subject had no further sequelae.

First-degree burn of forearm in a cold adult subject who was warmed with a warm water perfused blanket on a forearm, which was placed in a prototype negative pressure warming device.
It was concluded that the negative pressure did not counteract the thermoregulatory vasoconstriction; therefore, the applied heat was not transferred from the arm to the core. Instead, the heat built up on the arm, causing the burns to the skin.
Incident 3
In a more recent incident (2017), adult volunteer subjects were cooled in 8°C water to a Tes of 36°C. They were then warmed by a charcoal heater (HEATPAC personal heater, Emergco, Vancouver, Canada) applied either to the head or chest, after shivering was pharmacologically suppressed with IV meperidine (maximum cumulative dose of 3.3 mg·kg-1). 6 The HEATPAC consists of an combustion chamber (24 × 12 × 6.5 cm) containing a charcoal briquette and a small fan that blows warm air from the chamber through 4 flexible, noncollapsible heating ducts (110 × 2.5 × 1 cm). Manufacturer instructions indicate the chamber should be inserted into the supplied insulated pouch, but the heating ducts can be applied directly to the skin.
For the chest heating trials, the charcoal combustion chamber was placed on the chest, and the heating ducts were run up over the shoulders and under the back, then forward under the axillae and over the chest. At the end of 1 chest warming trial, 1 male subject had experienced significant reddening of the skin on the side of the neck (an area in direct contact with the heating ducts), which later blistered, indicating a second-degree burn (Figure 4). Conservative treatment involved keeping the wound clean and avoiding breaking the blisters. The injury resolved over the next 2 wk, and the subject experienced no further sequelae.

Second-degree burn on neck of a mildly hypothermic adult subject who had a charcoal heater placed on the chest and the flexible noncollapsible heating tubes placed over his shoulders/neck and wrapped under his back and on to the chest. Top, day 0; middle, day 1; bottom, day 13.
Discussion and Implications
During the past few decades, considerable research has been published indicating the safety and therapeutic value of active external warming of cold patients, with heat applied to the upper torso (axillae, chest, and even the back). 3 ,4,7 It is generally accepted that virtually all sources of external heat that might be available in prehospital scenarios (except for warm water immersion, open stoves, and fire and fire-warmed rocks) are moderate and safe and will not trigger circumrescue collapse. 13 Circumrescue collapse involves symptoms ranging from physical collapse, to syncope, to cardiac arrest or ventricular fibrillation. One significant precipitating factor is anything that increases blood flow to the cold limbs (especially the legs); this can cause hypotension and further core cooling as blood cools in the periphery and returns to the heart (afterdrop) or return of harmful metabolites from the cold periphery. 2 ,3,6,7
Application of any portable heat source to the torso will not significantly increase peripheral blood flow and can be considered hemodynamically safe. 2 ,3,6,7 However, the 3 incidents reported here have emphasized a potential risk in that active external warming may cause first- to third-degree burns. Burn injuries may occur through misuse or unexpected consequences,14,15 warranting careful attention to manufacturer instructions and vigilant monitoring. Skin burns are dependent on several factors, including but not limited to high skin temperature (usually higher than 43°C), 16 duration of heating period (usually 1–3 h), 17 pressure on the skin, and poor skin perfusion.18,19 Skin blood flow can be compromised either by intrinsic factors (thermoregulation 20 or vascular insufficiency 21 –23) or extrinsic factors (pressure exerted by, or on top of, the heat source24,25).26,27
There are several case reports of burns in surgical patients undergoing forced-air warming during anesthesia. 14 ,15,28 One patient experienced first-degree burn, likely because of the extended period of warming (3 h). 28 Two other cases were caused by a common misuse of the systems, wherein the heating hose was not connected to a manufacturer-provided cover but simply placed under a blanket (a practice commonly referred to as hosing).14,15 In the series of incidents reported here, the burns were caused not by forced air but by direct skin contact with a warming device. Indeed, burns have also been reported for patients lying on electric heating pads, due in part to the pressure caused by lying on the pads. 29 Thankfully, most, if not all, risk factors for burns can be mitigated by a combination of proper use, regular monitoring, and potentially product design. The following recommendations may reduce the risk of burning a cold patient during the prehospital warming process.
First, some insulation should be placed between all heat sources and the skin. Even though a responder might be tempted to apply the heat directly to the skin to maximize heat transfer (which it will), manufacturer instructions should be read and followed carefully. With the exception of the HEATPAC, instructions usually indicate that some material should be placed between the heat source and the skin to insulate the skin from too much heating. It may be prudent to add this recommendation for the HEATPAC as well. With this device, the configuration of running the heat ducts over the shoulder and under the back ensures tight contact on the back but also along the neck. This increased pressure may have facilitated the burn injury in Incident 3.
The requirement for skin insulation is an unfortunate, but necessary, reality of burn prevention because the insulation decreases the amount of heat that can be transferred, thus wasting valuable heat energy. However, some insulation of the skin with all heat sources would be prudent practice, with the possible exception of devices that use a feedback loop to control skin temperature at a desired safe level (see the suggestion regarding electric heating pads below). It should be noted that following manufacturer instructions is no guarantee that burns will not occur. Therefore, the following suggestions should also be considered.
Second, it is preferable for heated skin to be monitored to prevent burning. Many prehospital scenarios require the patient to be wrapped and warmed for extended periods while waiting for, or even during, transport. It would therefore seem prudent to make attempts to visually inspect the heated skin at regular intervals if possible, to observe for excess reddening or other signs of pending burns; in these cases, active heating should be stopped in the affected areas. It should be noted that frequent observations may not always be feasible. Potential constraints include opening the hypothermia wrap to the cold environment, difficulty accessing the patient during transport, the impact of frequent disturbance of the patient, and poor lighting making it difficult to observe the skin adequately.
Third, due to the effects of pressure in increasing the burn risk, rescuers must be aware of this increased risk in areas in which the patient is lying on top of a heat source. Thus, we suggest altering advice to preferentially add heat to the chest and axillae and to only consider heating the back if 1 of 2 conditions can be met: 1) rescuers are able to regularly observe this area for the development of burns; or 2) the system can vary the heating to maintain a lower safe skin temperature (see later).
Fourth, some technical solutions could be investigated. It would be an advantage if gel chemical heat packs (which can rapidly reach a peak temperature of above 47°C but drop rapidly thereafter) 30 could have their chemical makeup altered to provide a lower and safer initial temperature increase, which would remain at a plateau for a longer period. This would reduce the risk of burns and improve the core warming capacity.
One solution to limitations in direct skin observation could be skin temperature sensors that provide continuous feedback and warnings when skin temperature is too high. This could direct rescuers to adjust or remove heat before a burn occurs.
It would also be an advantage to use a heat source (eg, an electric resistive heating pad) that uses a feedback loop to control skin temperature at a desired level. It would be especially useful if this control could vary across the surface of the heat source and therefore different pressure or insulation zones could receive the most efficient heating within safety margins.
Conclusions
Three incidents have been presented that emphasize that active external warming of cold individuals, although physiologically safe, can cause first- to third-degree burns. However, the authors are confident that active external warming is beneficial and can be considered safe if proper precautions are taken to provide some insulation between the skin and heat source and to avoid placing the heat in high-pressure areas (eg, the back of a supine patient) unless the skin can be observed regularly. Efforts should also be made to monitor the skin (either visually or electronically) for excessive skin temperature or signs of burn risk.
Author Contributions
GG and BW: report conception, case review, manuscript preparation and review.
Financial/Material Support
None.
Disclosures
None.