
Abstract
Introduction
In 2011, our hospital on the Izu peninsula began to hold meetings to discuss how to manage patients with decompression illness (DCI) to establish a cooperative medical system. We retrospectively investigated the influence of these meetings and the changes subsequently effected.
Methods
A medical chart review was retrospectively performed to investigate all cases between January 2005 and December 2017 in which the transport of patients with DCI via a physician-staffed helicopter emergency medical service (HEMS) was attempted. The patients were divided into 2 groups: the preprogram group and the postprogram group.
Results
There were 63 patients in the preprogram group and 65 in the postprogram group. There were no cases in which a patient's symptoms deteriorated during transportation by the HEMS. The frequency of dispatch to the scene for direct evacuation in the postprogram group (86%) was greater than that in the preprogram group (74%), but the difference was not statistically significant (P=0.09). In the postprogram group, the duration of activities at the scene or the first aid hospital was significantly shorter in comparison to the preprogram group (P=0.01).
Conclusions
This retrospective study revealed simultaneity between the introduction of the yearly meetings and a reduced duration of the HEMS staff's activity at either the scene or the first aid hospital.
Introduction
A physician-staffed helicopter emergency medical service (HEMS) was introduced in eastern Shizuoka, Japan, in 2004. The HEMS, which covers the whole of eastern Shizuoka, including the Izu peninsula, has an arrival time of <20 min and provides early medical intervention and transportation for patients with various critical illnesses. 1 –6 Our facility (Juntendo University Shizuoka Hospital, Izunokuni) serves as the base hospital and is responsible for eastern Shizuoka (population: approximately 1.1 million). It is also the leader of the medical control council (MCC) system, which oversees the activities of the fire department as members of the Japanese Medical Association (Figure 1).
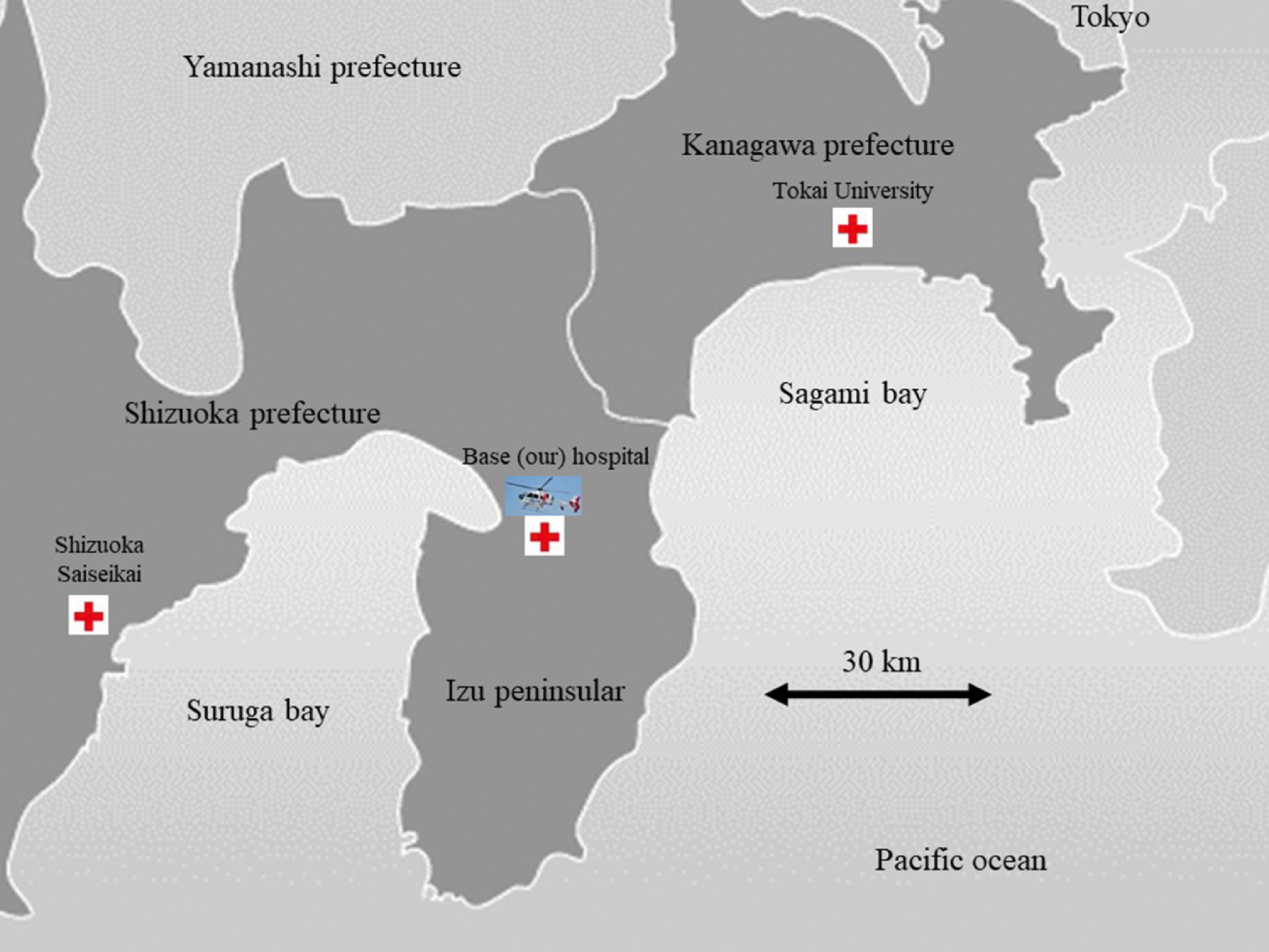
The system in which patients with possible DCI after diving are transported by helicopter to a medical facility with large recompression equipment. Patients with DCI encountered on the eastern shore are mainly transported to Tokai University Hospital, whereas those encountered on the western shore are mainly transported to Shizuoka Saiseikai Hospital. Red cross: Our hospital, Tokai University Hospital or Shizuoka Saiseikai Hospital. Helicopter: base (our) hospital.
The Izu peninsula, which is a popular location for recreational scuba diving, is located near Tokyo. Search and rescue for patients with decompression illness (DCI) is mainly conducted by professional divers who belong to local dive shops and/or the coast guard. 7 After reaching shore, transportation to the hospital is carried out by the fire department for recompression treatment with hyperbaric oxygen (HBO) therapy. A helicopter is necessary for such cases because there are no suitable hospitals in the Izu peninsula; only the Juntendo University Shizuoka Hospital has a monoplace chamber for HBO therapy. 8 –11 This monoplace chamber is used for patients with stable vital signs and who are alert, presenting with sudden deafness, ileus, intractable ulcer, or some forms of the bends. The HEMS can transport patients from the scene to a suitable hospital within 15 to 20 min. In contrast, a ground ambulance would take at least 1.5 h to reach the receiving hospitals (Figure 1). However, professional divers belonging to local dive shops and the coast guard operate outside of the regular MCC system.
In January 2011, our hospital, which is a leader of the Izu peninsula MCC, began to hold meetings concerning the management of patients with DCI to establish a cooperative medical system for such patients in the Izu peninsula. 7 Representatives from the fire department, coast guard, HEMS, and professional divers belonging to local dive shops in the Izu peninsula joined the meeting. This meeting has been held annually since 2011. At this meeting, we hold lectures concerning new topics related to DCI; review the at-the-scene management of patients with DCI using videos; discuss how to recognize DCI; share information on the diving profile using a diving checklist; and review the proper, prompt management of patients with DCI, including early transportation. 7 Before development of the cooperative medical system, patients were transported to a hospital with HBO therapy by the HEMS without triage for the treatment of almost any symptom arising during or after diving, and there was no unified information about the patient's diving history or symptoms. However, according to recent international consensus statements, diving incidents may be managed differently based on the severity of DCI manifestations; for example, ambiguous and certain so-called mild symptoms may be treated by normobaric oxygen and medical surveillance, whereas severe cases with unstable vital functions must be stabilized and resuscitated before evaluation for any further treatment by HBO. 12
Since development of the cooperative medical system, patients with mild symptoms (type 1), 12 symptoms that were not related to DCI (judged by diving history, or with cardiac arrest due to DCI have been transported to our hospital (Juntendo University Shizuoka Hospital) by the HEMS; our hospital only has a monoplace chamber for HBO therapy. There are currently no guidelines concerning HBO therapy for cardiac arrest owing to DCI. However, because there have been no reports of patients who fully recovered after entering cardiac arrest following DCI, probably because of the poor prognosis of respiratory arrest (hypoxia-induced cardiac arrest) in comparison with cardiogenic arrest, our district decided to transport such patients to our hospital. In addition, the HEMS started to send patients with DCI to the receiving hospital for HBO therapy with unified information concerning the patient's diving history. This was obtained using a diving checklist concerning personally identifiable information, diving profile, years of experience of diving, vital signs, and prehospital treatments 11 and was started in January 2011 when the agreement to use the checklist was made in the meeting.
Accordingly, we retrospectively investigated the influence of the cooperative medical system developed during these meetings and the changes that were observed concerning the management of patients with DCI.
Methods
The present study was approved by the review board of Juntendo Shizuoka Hospital, and the examinations were conducted according to the standards of good clinical practice and the Declaration of Helsinki.
To investigate the significance of the DCI meetings, we performed a retrospective medical chart review to investigate all cases in which the transportation of patients with DCI via the HEMS was attempted; the study period was January 2005 to December 2017. The patients were divided into 2 groups: One was the preprogram group, which included cases in which transportation via the HEMS was attempted between January 2005 and December 2010; the other was the postprogram group, which included cases in which transportation via the HEMS was attempted between January 2011 and December 2017. Patient age, sex, symptoms (mild or severe), 12 frequency of dispatch to the scene or transportation from the first aid hospital to the receiving hospital for HBO therapy, duration from the onset of DCI to the HEMS request, duration of HEMS staff activity at the scene or the first aid hospital, frequency of transportation to the base hospital or the receiving hospital for HBO therapy, and duration from the onset of DCI to arrival at final destination were analyzed. Mild pain, skin symptoms, and unspecified symptoms such as nausea without abnormal vital signs were classified as mild symptoms. Neurological abnormalities, respiratory symptoms such as dyspnea, loss of consciousness, vertigo, and cardiac arrest were categorized as severe cases. Combinations of mild and severe symptoms were classified as severe symptoms. In addition, the final outcome of the patients with DCI who were transported to the base hospital was also analyzed. The final outcome was classified into 4 categories: 1) cancellation of dispatch (cancellation or return to the hospital because of misdiagnosis of DCI); 2) return home (mild symptoms subsided with infusion and normobaric oxygen therapy as initial treatments); 3) survival after admission (the patient was alive at the time of discharge); and 4) fatal outcome (the patient ultimately died). Infusion referred to fluid resuscitation being performed with Ringer's lactate solution to correct hypovolemia.
The statistical analyses were performed using the non-paired Student's t test for age and duration; the χ2 test for sex, frequency of dispatch, and final destination; and a contingency table analysis for the final outcome. P values of <0.05 were considered to indicate statistical significance. All data are presented as the mean±SD.
Results
The pre- and postprogram groups included 63 and 65 patients, respectively. No patients with DCI were transported via the HEMS in 2004. There were no cases in which a patient's symptoms deteriorated during transportation by the HEMS.
The results of the analysis of the study population are shown in Table 1. There were no significant differences with regard to sex, age, duration from the onset of DCI to the HEMS request, or duration from the onset of DCI to arrival at final destination. The frequency of dispatch to the scene for direct evacuation in the postprogram group (86%) was higher than that in the preprogram group (74%); however, this difference was not statistically significant (P=0.09). Minor symptoms in the preprogram group (10%) were observed significantly more frequently than in the postprogram group (1.5%). The duration of activities at the scene or the first aid hospital in the postprogram group was significantly shorter than that in the preprogram group. In contrast, the frequency of transportation to the base hospital by the HEMS in the postprogram group (26%) was significantly greater than that in the preprogram group (6%).
Results of the analysis
HEMS, physician-staffed helicopter emergency medical service; HBO, hyperbaric oxygen therapy.
Airlift of 2 patients was canceled after the dispatch of the HEMS because of misdiagnosis of decompression illness.
The final outcomes of the patients who were transported to our hospital are shown in Table 2. Six patients in the preprogram group and 17 patients in the postprogram group were transported to our hospital. No dispatches were canceled in the postprogram group, but 2 were canceled in the preprogram group because of misdiagnosis of DCI. With regard to the 4 outcomes, the numbers and frequencies of the patients who were able to return home (after their symptoms subsided), survived after admission, and sustained a fatal outcome were greater in the postprogram group than in the preprogram group. However, these differences were not statistically significant (P=0.06). All patients with fatal outcomes were in cardiopulmonary arrest when the emergency medical technician and physicians of the HEMS checked them. Among the 8 total patients classified as having severe symptoms, 5 had loss of consciousness and 3 had dyspnea either during or after diving, but they were nevertheless transported to our hospital. These 8 patients became free of symptoms before the physicians of the HEMS checked them. They all received normobaric oxygen from emergency medical technicians and then received Ringer's lactate solution infusion from the staff of the HEMS in the prehospital area. The 5 patients with loss of consciousness were diagnosed with syncope by vasovagal reflex, and the 3 patients with dyspnea were diagnosed with aspiration of seawater based on the results of physiological, radiological, and biochemical examinations, including an ultrasound study at our hospital. All were introduced to local medical facilities near their residence to follow their medical condition, and we received no reports of any delayed DCI from the local medical facilities. One of the mild patients who had knee pain (bends) did not experience any symptom improvement with normobaric oxygen or infusion of Ringer's lactate solution, so that patient received 1 session of 60 min of HBO (2 atmospheres absolute, which was the standard treatment pressure used at this facility) after admission. After this treatment, symptoms improved, and the patient was discharged the next day.
Final outcome of patients who were transported to the base (our) hospital (n=23)
Discussion
This report revealed that the duration of the HEMS staff activity at the scene (scene time) or the first aid hospital significantly decreased, and no improvement in final outcome was achieved based on a few minutes’ difference in the interaction time onsite or transport time. This result suggests that the discussions about the prompt management of patients with DCI at the annual meetings might be effective. Before the meeting, there was inconsistent reporting of cases on patients with DCI; instead, information was randomly collected from the patient or from professional buddy divers at the diving shop. After the meeting, according to the cooperative medical system protocols, the professional divers at the diving shop and the emergency medical technicians attempted to collect information based on the diving checklist before the arrival of the HEMS. These activities might have helped to reduce the duration of activity at the scene. Even though the duration of the HEMS staff activity at the scene or the first aid hospital was decreased, this did not reduce the time from the onset of DCI to arrival at final destination. This may be because the HEMS staff members were transported to the scene from a rendezvous zone by an ambulance to provide early medical intervention, because dispatching to the scene increased the time to reach the final destination.
This report revealed that the number of requests for dispatch of the HEMS for divers and mildly symptomatic patients significantly decreased in the postprogram group. This might be because after implementation of the annual meetings, we attempted to perform triage when selecting the final destination. In addition, trained clinicians after 2011 tended to perform more detailed examinations, revealing symptoms of severe decompression sickness that might have gone unnoticed on a cursory examination. 13 Thus, we attempted to transport patients whose symptoms had subsided after the initial treatment or the most severe cases (patients in cardiac arrest) to the base hospital, which only has a monoplace chamber for HBO therapy. The Japanese Society of Hyperbaric and Undersea Medicine recently suggested that patients with mild-type DCI receive HBO therapy in a monoplace chamber. 14 In addition, even normobaric oxygen therapy could result in symptom improvement for some patients with DCI. 15 Accordingly, our institute attempted to treat the mildest cases of DCI, which involved patients whose symptoms subsided after the initial treatments. Although there might be some criticism that loss of consciousness is a symptom of possible severe decompression sickness and that this symptom is typically aggressively treated with a hyperbaric chamber, the 5 patients who were transported to our hospital showed no sequelae from not being treated with a hyperbaric chamber. However, we should have treated these divers with the use of a multiplace hyperbaric chamber.
Decompression sickness during diving is often complicated by drowning; however, the rate of favorable survival after drowning due to cardiac arrest remains extremely low because such patients experience respiratory arrest. 16 In addition, we could not find any reports describing full recovery after cardiac arrest due to both DCI and drowning. Accordingly, after implementation of the annual meetings, we began to treat these cases, for which prognosis was dismal, in our hospital. We consider multiplace HBO chamber therapy inappropriate for diving-related cardiac arrest patients without return of spontaneous circulation because this would require them to be taken to a receiving hospital by the HEMS. This did not apply to those with return of spontaneous circulation. In addition, the reason for the high fatality rate at our hospital (approximately 50%) was associated with the fact that our hospital treated patients who experienced cardiac arrest while diving.
Therapy with HBO, which remains the mainstay of DCI treatment, should be initiated as soon as possible. 17 Divers Alert Network (DAN), a worldwide network promoting scuba diving safety, provides emergency assistance, medical information resources, and educational opportunities for divers. International DAN, which has various locations around the world, also provides expert emergency medical and referral services to regional diving communities. A report on the triage and emergency evacuation of recreational divers based on DAN hotline data showed that the median time from injury to arrival at a treatment facility was 20 h; that time did not influence the outcome because there were few severe cases, and the recognition of DCI by divers themselves was delayed. 18 In addition, the DAN hotline takes calls from all over the world, often from divers in remote areas, and transport delays are normal. 14 In contrast, the cooperative medical system for patients with DCI that was implemented in the Izu peninsula treated many severe cases and transported all patients with DCI within a few hours, free of charge.8,9
In Scotland, although the fiscal responsibility for recompression in the treatment of DCI is covered by the National Health Service, 19 the treatment of divers with DCI is provided by a single, coordinated clinical service. The vast majority of cases are initially processed through a single telephone hotline through a consultant at the hyperbaric facility. 20 The physician will advise on the most appropriate treatment pathway in terms of the recompression chamber to which the patient should be transported and the best form of transportation (including air evacuation) based on a discussion with the diver, local medics, and/or emergency services. 20 As a result, the median time from onset to treatment in patients with severe DCI who were transported by air was 3 h. 20 Although differences in the reporting/calling attitude of the examined population were noted, the average time from onset to treatment in our system was 2 to 2.5 h. The coordinated and combined use of public servants and civilian resources in response to cases of DCI, with a mutual understanding of how to improve patient outcomes, is beneficial for managing patients with DCI. The importance of the early recognition of DCI by EMS personnel and the appropriate consideration of ground vs flight transportation to the nearest hyperbaric center for patients with DCI has also been reported. 21
The present study has several limitations, including the small study population and the retrospective nature of the study. In addition, we only had a monoplace chamber at our institution, which was not suitable for treating severe cases of DCI. Furthermore, we were unable to investigate whether the change in dispatch patterns resulted in saving resources for communities even if the HEMS did not transport the severely ill or transported very stable patients. Moreover, we were unable to analyze the final outcomes of patients with DCI who were transported to receiving hospitals for HBO therapy; thus, we were unable to evaluate whether our attempts improved the outcomes of patients with DCI. Accordingly, we plan to invite members of the receiving hospitals that perform recompression treatment to our meetings in the near future to evaluate the final outcomes of patients with DCI.
Conclusions
This retrospective study revealed simultaneity between the introduction of the yearly meetings and a reduced duration of HEMS staff activity at either the scene or the first aid hospital. All of the participants in the meetings cooperated in preparing for the management of patients with DCI with a mutual understanding of how to improve the outcomes of patients with DCI.
Footnotes
Author Contributions
All authors (YY, MO, YN, HN, IK, KJ, SM, HO, KI, KO) made substantive contributions to the study, and all authors endorse the data and conclusions.
Financial/Material Support
This manuscript obtained financial support from the Ministry of Education, Culture, Sports, Science and Technology (MEXT)-Supported Program for the Strategic Research Foundation at Private Universities, 2015–2019. [The constitution of a total research system for comprehensive disaster medical management, corresponding to wide-scale disaster].
Disclosures
None.