
Abstract
Introduction
Cardiac events are one of the leading causes of death in the Spanish population. Given the increase in the nontraumatic medical conditions found in mountain rescues, the objective of this study was to report on the heart conditions of patients rescued in the mountains of Aragón in the Spanish Pyrenees.
Methods
We conducted a retrospective observational study based on data collected from patients’ medical histories for rescues undertaken in from 2010 to 2016 (at altitudes between 500 m [1640 ft] and 3404 m [11,168 ft]).
Results
Of the 2079 individuals rescued from 2010 to 2016, 34 (2%) were diagnosed with heart conditions, accounting for 21% of all nontraumatic medical conditions. The data showed a statistically significant increase in the age of the rescued patients with heart conditions (55±15 y) and those with acute coronary syndrome/sudden death (60±8 y). Eighty-five percent of the rescued patients with heart conditions were men, 62% were rescued above 2000 m (6500 ft), 42% had acute coronary syndrome (of whom 56% had inferior infarction), and 35% died suddenly.
Conclusions
Aragón mountain rescues show an increase in patient age in recent years. The most common medical case among rescued individuals with heart conditions was a hiker over the age of 50 y with cardiovascular risk factors, inferior infarction, and occurrence at an altitude above 2000 m. Based on our observations, appropriate training should be undertaken, especially by older hikers, who may also benefit from cardiac screening, and rescue vehicles/personnel and mountain huts should be equipped with semiautomatic external defibrillators.
Background
The autonomous community of Aragón is located in northeastern Spain, bordering France and the middle of the Pyrenees. In 2015, 32% of all deaths in Aragón were due to circulatory system disorders, the leading cause of death in Aragón.
The considerable variety of tourism options, especially in terms of physical fitness, makes this autonomous community a major tourist center for all age groups. Aragón's ski resorts offer winter sports, and the numerous natural habitats, such as the National Park of Ordesa and Monte Perdido, the natural parks of Posets-Maladeta, and Sierra de Guara and Sierra del Moncayo, provide year-round activities. Many of Aragón's mountain peaks are above 3000 m (9800 ft). These characteristics make Aragón's mountains a remote and rugged area, especially important for conducting mountain emergency rescue services.
The 061 Mountain Rescue Unit of Aragón, which is staffed by physicians and nurses, has been working jointly with rescue specialists and the Spanish Air National Guard since 2002. These collaborations have improved the medical care provided in the field and reduced the transfer time to definitive care facilities.
In recent years, there has been an increase in Aragón in the number of rescues and patients with nontraumatic medical conditions. From 2010 to 2016, 8% of rescued patients had nontraumatic medical conditions, the most common of which were heart conditions (21%), resulting in more than half of the deaths. 1
Given the significance of cardiac events in the general population and the nonnegligible rate of heart conditions in rescued patients, we conducted a broader study of this type of rescued patient. Our ultimate objective is twofold: we aim to describe the main characteristics of rescues involving heart conditions and, based on these characteristics, we aim to provide recommendations for patients and healthcare staff to most effectively deal with the combination of heart disease and mountain activity.
Methods
An observational, descriptive, retrospective study was conducted of patients who presented with cardiac events and were treated by the 061 Mountain Rescue Unit of Aragón between July 2010 and December 2016. The study was authorized by the management of 061 of Aragón and by the clinical research ethics committee of Aragón.
The data were collected by members of the 061 Mountain Rescue Unit, who consulted the rescued patients’ medical records and the database that stores information on rescues. The selection/inclusion criterion was presentation with a heart condition, defined by the presence of any of these symptoms: chest pain, palpitations, or syncope. Patients were diagnosed clinically through history and physical examination in the field and with electrocardiogram when possible. We excluded neurocardiogenic syncope with normal electrocardiogram and anxiety disorders. We analyzed the records of 34 patients and assigned each an identification number.
The following information was collected: demographic (age, sex, country of origin), clinical (type of condition, history, and risk factors), treatment (reperfusion therapy), and activity- and rescue-related (type of activity, year, season, altitude at which the patient was found, and transfer in an advanced life support [ALS] vehicle).
Data are presented as mean±SD (with range as appropriate). We performed a statistical analysis of the quantitative and qualitative variables using Student's t tests and χ2 tests, respectively. We analyzed the pattern of the number of rescues per year using a linear regression. The differences were considered statistically significant at P<0.05. All significant statistical tests reported in this article have power=1–β greater than 95%.
Results
During the study period (2010–2016), 2079 patients were rescued, 2% of whom had some type of heart condition. The number of rescued individuals with heart conditions was 5±3 (range 1-10) per year. The data do not show any clear trend, except for a noticeable increase in 2016 (Figure 1).
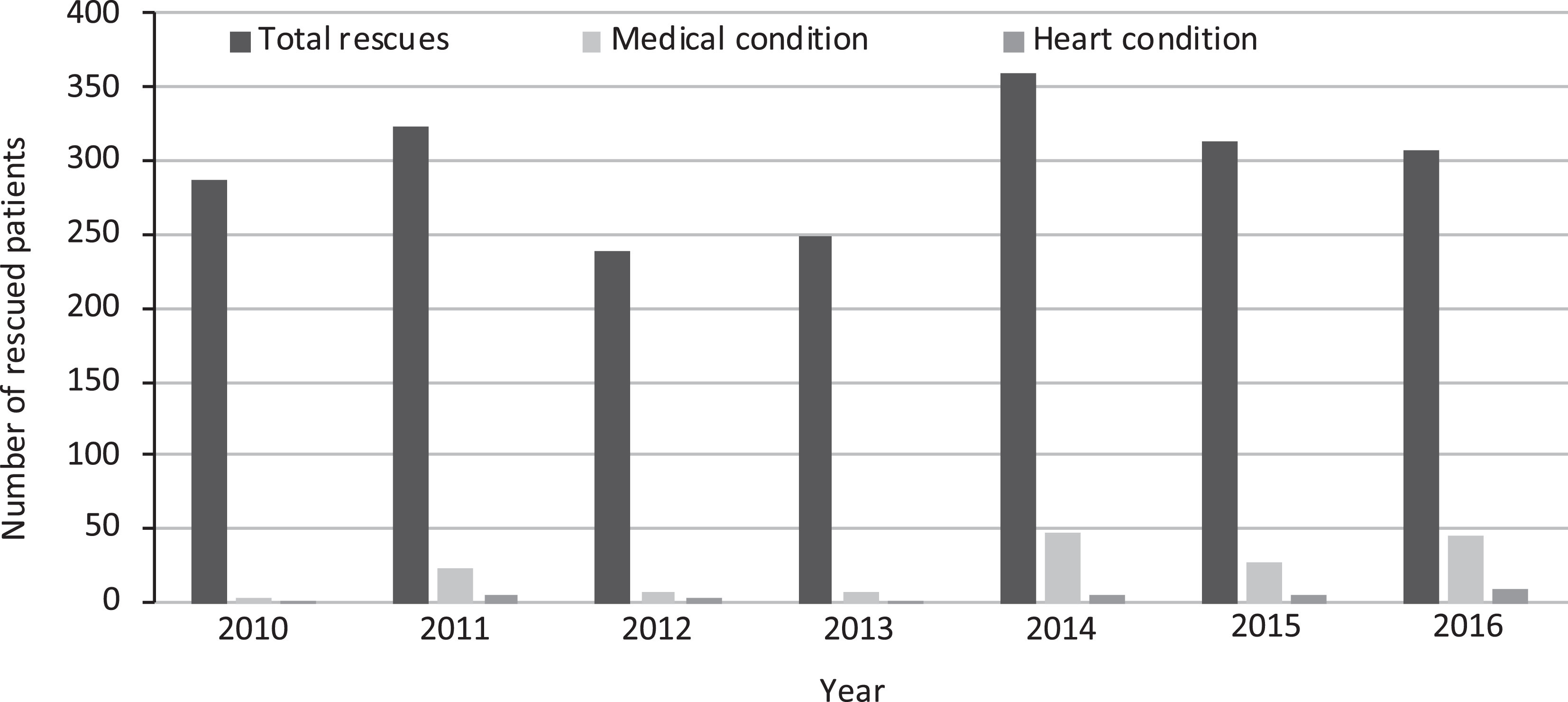
Evolution in the number of medical and heart disease rescues during the study. Mean±SD number of rescued individuals with heart conditions: 5±3 (range 1–10).
The age of patients with heart conditions (55±15 [range 16–77] y) and of patients with acute coronary syndrome (ACS)/sudden death (60±8 [range 46–72] y) was significantly higher than the age of all rescued patients (41±15 [range 1–90] y) (independent samples t test, P<0.001) (Figures 2 and 3). There was a statistically significant difference in the age distribution, with heart conditions more common beyond 50 y of age.
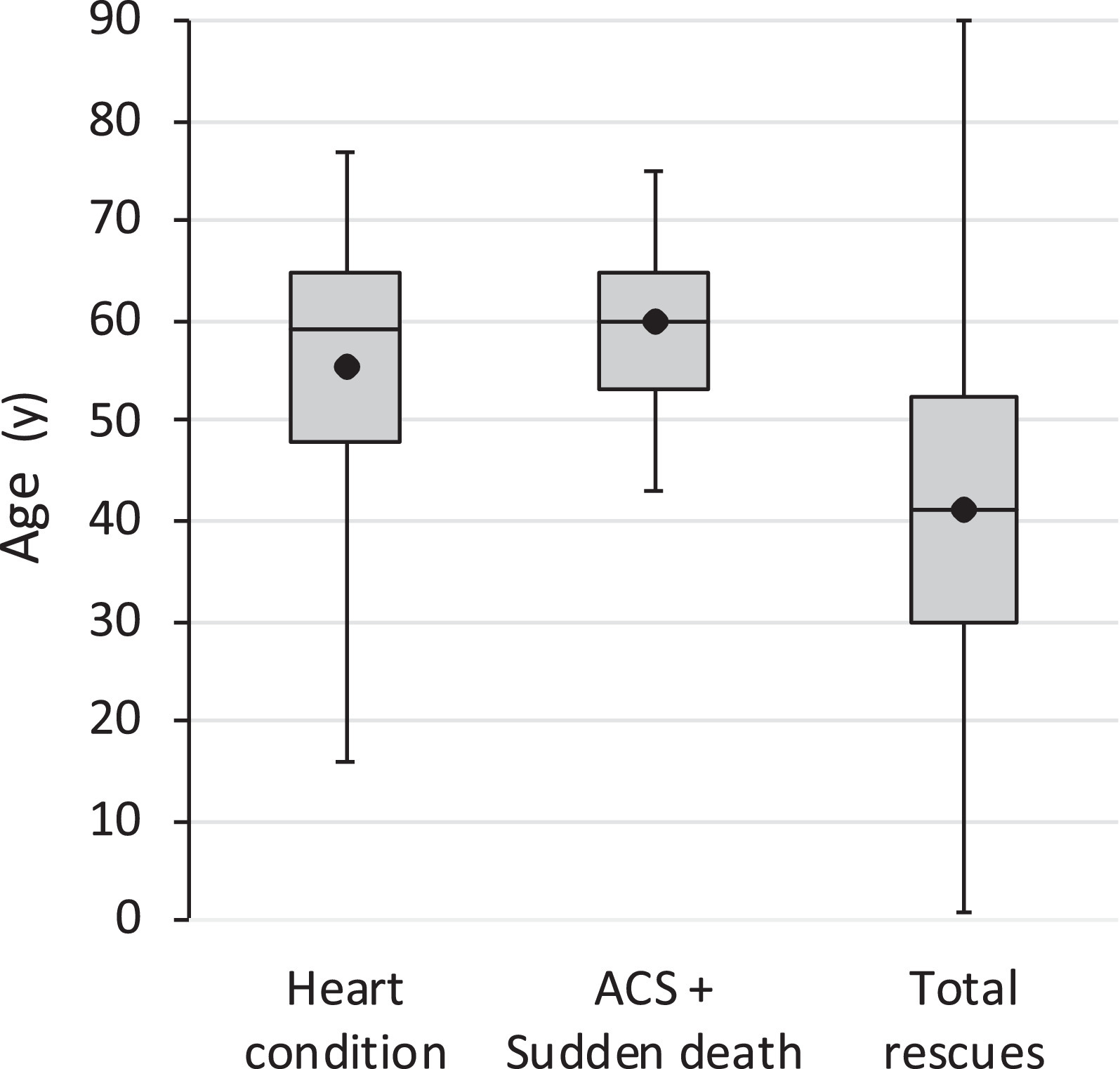
Box plots: From left to right, age of the rescued patients with heart disease, age of those with acute coronary syndrome (ACS) and sudden death, and age of the total of rescued patients (independent samples t test, P<0.001). For each dataset, the point represents the mean. Horizontal lines correspond to the 3 quartiles, and the ends of the whiskers show the minimum and the maximum of the dataset.
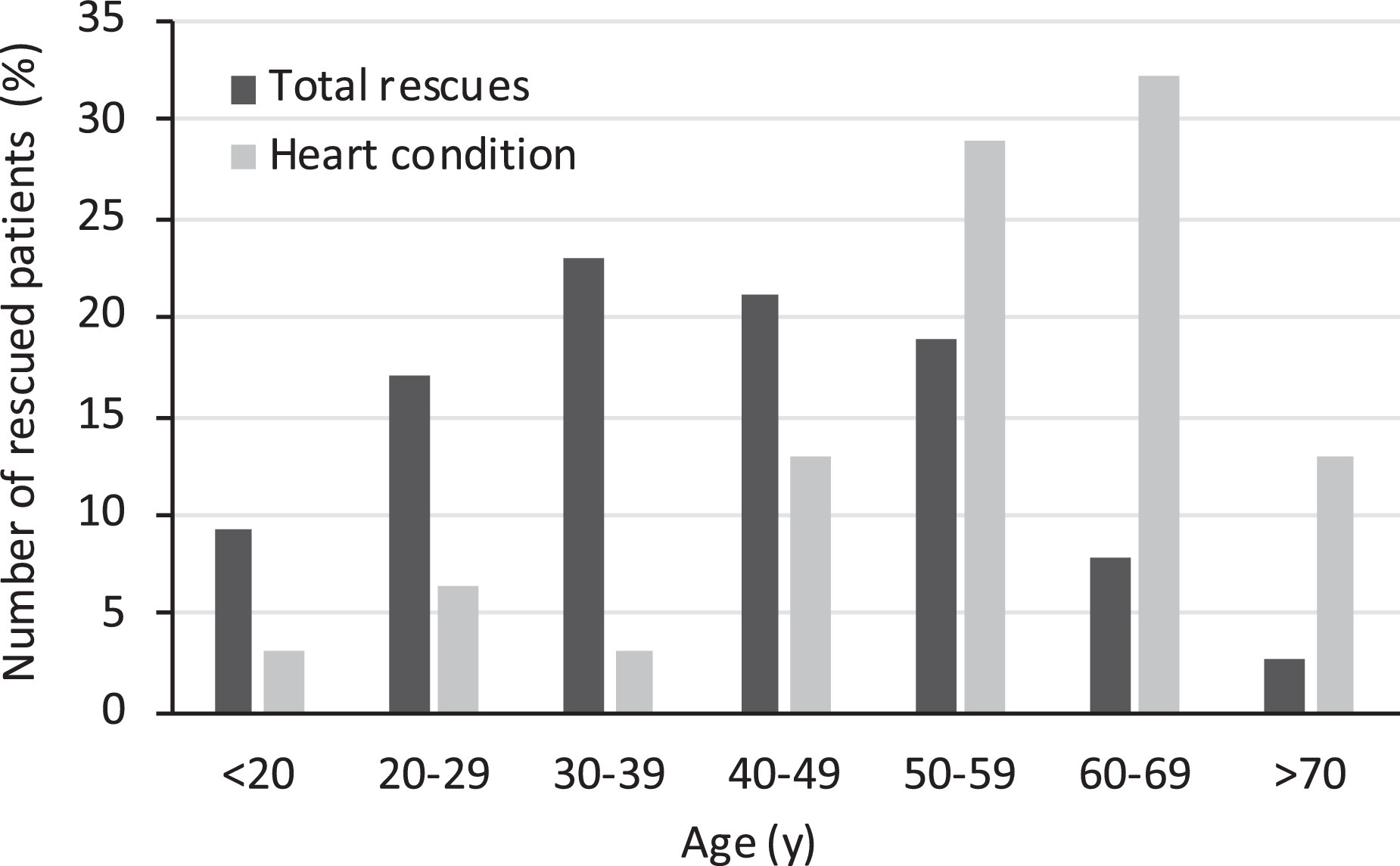
Distribution by age group of all rescues and of the patients with heart disease. Seventy-four percent of the patients with heart conditions were aged 50 years or older. The distributions are significantly different (χ2 test, P<0.001).
In terms of sex, 85% of the rescued patients were men. The age of the rescued men and women with heart conditions was 56±13 (range 16–77) y and 49±21 (28–72) y, respectively, with no statistically significant association.
Table 1 lists the conditions found according to the patients’ sex and final disposition. There was a predominance of ACS (42%) and sudden death caused by this syndrome (35%) in men. In terms of the patient's final disposition, 56% of the patients were transferred to a hospital, 26% of whom were transferred by ALS vehicles, 12% by emergency medical units, and 15% by medical helicopters of the 112 emergency unit. Some 58% of the patients with ACS were transferred to hospital in an ALS transport.
Cardiac or heart events found, patient's sex, and final outcome
AMI, acute myocardial infarction; ACS, acute coronary syndrome; ECG ab., electrocardiogram abnormalities; PSVT, paroxysmal supraventricular tachycardia.
Table 2 shows epidemiological characteristics regarding the most prevalent conditions in our patients. In terms of the patient's country of origin, Spain represented 65% of cases, and France represented 29%; however, there was an equal number of Spanish and French deaths. In terms of patient sex, 80% of the women were French, and all were hikers. In terms of the altitude of event occurrence, 62% were rescued from above 2000 m. The most common altitude range for ACS and death was 2000 to 2500 m. There were more cases of sudden death at altitudes above 2000 m (64%). There were no reports of patients with ACS rescued above 2500 m, although 1 of the patients was above this altitude engaging in sport activity before the coronary event. When relating altitude above 2000 m with the onset of ACS or sudden death, there were no statistically significant differences compared with the other conditions (χ2 test P=0.8).
Epidemiological characteristics
ACS, acute coronary syndrome.
The patients who died in the field as a result of a cardiac event represented 32% of the rescued patients with heart conditions. The number of annual sudden deaths was 2±1 (range 1–3), and the maximum number of deaths occurred both in 2014 and 2016.
The unit treated 12 patients with ACS, including 1 with cardiopulmonary arrest (CPA) who recovered after an acute myocardial infarction. The 12 patients corresponded to 35% of those rescued with heart conditions and were all men. The annual number of ACS cases was 2±2 (range 0–5) with 5 (42%) of all studied cases of ACS occurring in 2016. This could well be related to the fact that a year before, the infarction code registry of Aragón was implemented. All of those patients were transferred to a hospital, 58% in an ALS-equipped transport to optimize treatment and speed.
Clinical and treatment variables of the patients with ACS are described in the following. The most common risk factor of cardiac events in these patients was smoking; 50% of patients were smokers or had quit within the year before the event. Other risk factors were arterial hypertension (33%) and dyslipidemia (25%). One-third of these patients had a personal history of ischemic heart disease. The infarction was located in the inferior wall in more than half of the patients (56%), and an anterior location was found in 33% of the patients.
In terms of the coronary revascularization therapy administered to these patients, percutaneous coronary intervention (PCI) was performed in at least 50% of cases, half of which were included in the infarction code registry of Aragón (the other PCIs were performed before the implementation of this protocol). In one case, fibrinolysis was performed followed by a rescue PCI.
Discussion
We have found no other article that analyzes mountain rescue cases with associated heart conditions in detail. Nonetheless, we have found studies that reported rates for rescues with associated heart conditions very similar to those found in our sample. In recent years, there has been a noticeable increase in nontraumatic medical conditions in patients rescued in Aragón, from 8% to 12% in the past 3 y (2014–2016). Heart disease was the second leading nontraumatic medical condition after environmental medical conditions, representing 21% of patients rescued from 2010 to 2016. 1 In New Zealand, medical conditions represented 12% of rescue operations conducted from May 2010 to December 2011, and cardiovascular events were reported as the most common. 2 The rates were similar to those found in US studies in which the predominant cause of death within nontraumatic events was cardiovascular disorder. 3 In the United States, similar rates of heart problems and sudden death were reported for rescues in Denali (approximately 17%), and cardiac arrest after AMI was considered the largest single cause of death observed in Baxter State Park.4,5
The progressive increase in the number of rescues and patients with heart conditions is reflected globally in North America, Europe, and Asia. 6 This trend suggests there will be a greater concern for increased surveillance and for the implementation of preventive measures to keep up with the growth of recreational sports practice in modern society.
At the start of the 1990s, the mean age of those rescued was 37 y. By 2012, that age had increased to 45 y, and by 2016 (ie, our study's period), the age had reached 55 y. 6 The age increases to 59 y if we include ACS and sudden death, with a clear majority of the patients being men. 7 The longer life expectancy and the greater availability of leisure time could explain the increase in the mean age of those rescued in recent decades. Atherosclerosis gradually progresses with age, and therefore age is a predominant risk factor in coronary artery disease. 8
Hiking, the most popular physical fitness activity, 1 ,2,4,9,10 has benefits associated with healthy lifestyles and increased longevity. However, a lack of physical fitness, dehydration, excessive exercise intensity, and exposure to altitude can trigger adverse cardiac events in individuals with risk factors. 11
Although 62% of the patients who had a heart condition when rescued were found at an altitude higher than 2000 m (increasing to 64% for the patients who died), there was no statistically significant association. However, there are studies that have related myocardial ischemia with altitude. Reports from Mont Blanc have indicated between 5 and 10 cases of myocardial ischemia per year, probably because of the lack of high altitude adaptation and the rapid performance of intense activity. 7
Hypoxic conditions stimulate the sympathetic system, increasing the heart rate, cardiac contractility, and platelet aggregation. The onset of respiratory alkalosis can trigger arrhythmias, and the increased cardiac demand can cause myocardial ischemia.8,12 This situation, coupled with environmental conditions, intense exercise, dehydration, diet change, and emotional stress from dangerous conditions, can precipitate myocardial dysfunction.
A third of the patients in our sample had a history of ischemic heart disease, the symptoms of which can be exacerbated by altitude. Heart conditions are more common among older untrained men during the first 5 days of high altitude exposure. An optimal level of training is therefore recommended, along with appropriate acclimatization (at least 5 d), optimal medication control (especially statins and aspirin), and a stress test to assess the body's capacity for exercise and the potential onset of ischemia. 7 With this in mind, most older patients with heart disease can tolerate exposure to high altitudes safely with a minimum increase in risk. 8
Such cases will inexorably occur, and when they do, they will have to be managed in remote locations far from advanced medical services. The expertise of first responders and the rapid application of emergency services are vital to prevent disastrous results.
In urban settings, survival rates for CPA outside hospitals are low, with a 70 to 98% failure rate for resuscitation attempts. 13 The continuity of the survival chain is essential for favorable results14,15 and represents a major challenge for CPAs in remote locations.
Patients in mountaineering environments are expected to have poorer survival rates than those in urban areas because of the remoteness of their rescue location,whose characteristics (access difficulty, terrain, restricted means, and personnel) most often delay the start of treatment and the subsequent transfer to hospital. However, this finding is balanced somewhat by the fact that patients who engage in these types of activities are generally healthier than those in urban studies of CPA. 16
Studies have shown that training and the systematic use of semiautomatic external defibrillators (SAEDs) help reduce mortality. 17 In 2006, the International Commission for Alpine Rescue recommended the use of SAEDs, stating that approximately 50% of deaths during mountain hiking were from sudden death by cardiac arrest.
Rescue teams are therefore advised to carry an SAED to improve the results of emergency care in these cases.18,19 Supplying SAEDs to mountain huts and youth hostels in the mountains of Aragón is essential, as is promoting the training of mountain rangers and mountaineers in the use of SAEDs and first aid techniques. These initiatives increase survival chances by minimizing the time to the first defibrillation. The only patient with CPA in our study who was successfully resuscitated benefited from cardiopulmonary resuscitation carried out by on-scene bystanders and the use of an SAED located in a nearby mountain hut.
Treatment for patients with ACS has been optimized through Aragón's current infarction code protocols, 20 shortening the time to diagnosis, increasing survival, and minimizing the time to revascularization therapy (through fibrinolysis and/or PCI). These protocols require the support of ALS vehicles for fibrinolysis and/or transfer to an equipped hospital.
STUDY LIMITATIONS
Despite covering 7 y, the study's small sample size resulting from the low incidence of submitted cases precludes us from establishing unequivocal conclusions. The fact that there are no studies on mountain rescues with details on the heart condition of rescued patients prevents us from comparing the results.
The epidemiological characteristics of rescued patients may justify further research and observational work, both to efficiently guide practitioners toward the patient type that could be encountered and to establish effective preventive mechanisms.
Conclusions
Cardiac disease is an important cause of morbidity and mortality in the Pyrenees among those requiring rescue. Age is directly associated with a greater risk of presenting with adverse cardiac events. We are faced with an increasingly longer-lived population with more leisure time and an enjoyment of outdoor activities, with all the risks that this implies.
Based on our observations, the most common medical case among rescued individuals with heart conditions was a summer hiker over the age of 50 y with a history of cardiovascular risk factors (smoking, hypertension, or history of ischemia) who experienced an infarction (most frequently an inferior wall infarction) and occurrence at an altitude above 2000 m. This type of patient will probably need to be transferred to a hospital and could benefit from an SAED-equipped rescue team.
In terms of prevention, progressive and healthy training is therefore recommended. For the same reasons, a stress test to unmask silent ischemic heart disease should be considered before the performance of any remote activity that requires strenuous exercise, at least by the population with cardiovascular risk factors.
Footnotes
Acknowledgments
The authors thank the 061 Mountain Rescue Unit of Aragón for sharing their data. They are very grateful to L. Izquierdo for his patience and guidance during the study. They thank the editor and the anonymous reviewers whose comments helped us to improve this article.
Author Contributions: Study concept and design (CM, ES); data acquisition (ES); analyzing data (CM, ES); drafted and critically reviewed the manuscript (CM); approved final manuscript (CM, ES).
Funding/Material Support: None.
Disclosures: None