
Abstract
Snakebite envenomation is an important public health problem in tropical countries. We report a case of bilateral adrenal hemorrhage in a 28-y-old man with Russell's viper bite that occurred in the Sathyamangalam forest range in the Indian state of Tamil Nadu. In this case, a combination of early bite recognition, hospital-based supportive care, corticosteroid therapy, and timely administration of polyvalent antivenom resulted in a favorable clinical outcome.
Introduction
Snakebite envenomation is an important public health problem in tropical countries, especially in rural regions. 1 Russell's viper (Daboia russelii) is a venomous snake belonging to the family Viperidae. In the Indian subcontinent, Russell's viper bite forms a significant proportion of snake bite incidents. In Sri Lanka, for instance, the Russell's viper contributes to 30 to 40% of all snakebites, 2 but in the specific district of Anuradhapura in Sri Lanka Russell's viper is responsible for as much as 73% of all snakebites. 3 India has the highest number of snakebite deaths in the world, 3 and Russell's viper is a leading cause of snakebite deaths in India. 4 Additionally, in neighboring Myanmar (Burma), Russell's viper contributes to over 70% of snakebite deaths. 4 Addisonian crisis is an uncommon complication of Russell's viper envenomation. Herein, we present a case of Russell's viper envenomation–associated Addisonian crisis.
Case Report
A 28-y-old male shepherd was bitten by a snake in the right leg while working in the field. This incident occurred in the Sathyamangalam forest range in the Indian state of Tamil Nadu. The snake that was killed thereupon was easily identified as a Russell's viper (D russelii) (Figure 1) by a herpetologist who was summoned to the local hospital where the patient was initially treated.

Russell's viper (Daboia russelii).
The geographic locale where the patient was bitten was 35 km from the local hospital. The bite-to-hospital time was 2 h. The patient was administered 150 mL of polyvalent antivenom as per protocol when he started exhibiting both local and systemic signs and symptoms of envenomation. The bite-to-needle time was 2.5 h. The patient responded to treatment and improved clinically. His hematologic, metabolic, biochemical, and coagulation parameters were noted to be normal after the aforementioned therapy.
On the fourth day after the bite, he developed sudden-onset lower abdominal pain and vomiting. He was initially managed conservatively for about 6 h but later became febrile and hypotensive and was transferred to a tertiary care hospital. On admission, he was found to be drowsy, disoriented, febrile (39°C [102°F]), tachycardic (114 beats⋅min-1), tachypneic (26 breaths⋅min-1), and hypotensive (blood pressure 60/40 mm Hg). Abdominal examination revealed mild abdominal distention with diffuse tenderness and decreased bowel sounds. Examination of other systems did not reveal any overt abnormalities. He was resuscitated with 2 L of intravenous 0.9% saline, and dopamine infusion was started at a rate of 10 μg⋅kg⋅min-1, to which he failed to respond. His electrocardiogram showed sinus tachycardia, and transthoracic echocardiography revealed normal left and right ventricular size and function, without any significant valvular disease. He was connected to a FloTrac sensor hemodynamic monitoring system (Edwards Life Sciences, Irvine, CA), which demonstrated high cardiac output and low systemic vascular resistance. As a result, noradrenaline was administered with a titrating dose ranging from 2 to 5 μg⋅kg⋅min-1 to maintain a reasonable mean arterial pressure. Meanwhile, his blood arterial gas analysis was obtained, which revealed severe metabolic acidosis (pH 7.01, HCO3 8.7 mEq⋅L-1, lactate 12 mEq⋅L-1). His serum sodium, potassium, and random blood glucose levels were found to be 110 mEq⋅L-1, 6.1 mEq⋅L-1, and 60 mg⋅dL-1, respectively. Other investigations included blood urea nitrogen, creatinine, complete blood count, and coagulation profile, which were within the normal range. Blood and urine cultures were sterile. Computed tomographic scan of the abdomen showed bilateral homogeneous, smooth, adrenal enlargement with high attenuation, consistent with bilateral adrenal hemorrhage (Figure 2). His symptoms, physical examination, laboratory work, and imaging all pointed toward a diagnosis of adrenal insufficiency, which was eventually confirmed with definitive testing. His serum 0900-h cortisol level was found to be 235 nmol⋅L-1, and a short Synacthen test revealed a cortisol level of 229 nmol⋅L-1 at 30 min and 200 nmol⋅L-1 at 60 min after administration of 250 mg tetracosactide, which established the diagnosis of adrenal insufficiency.
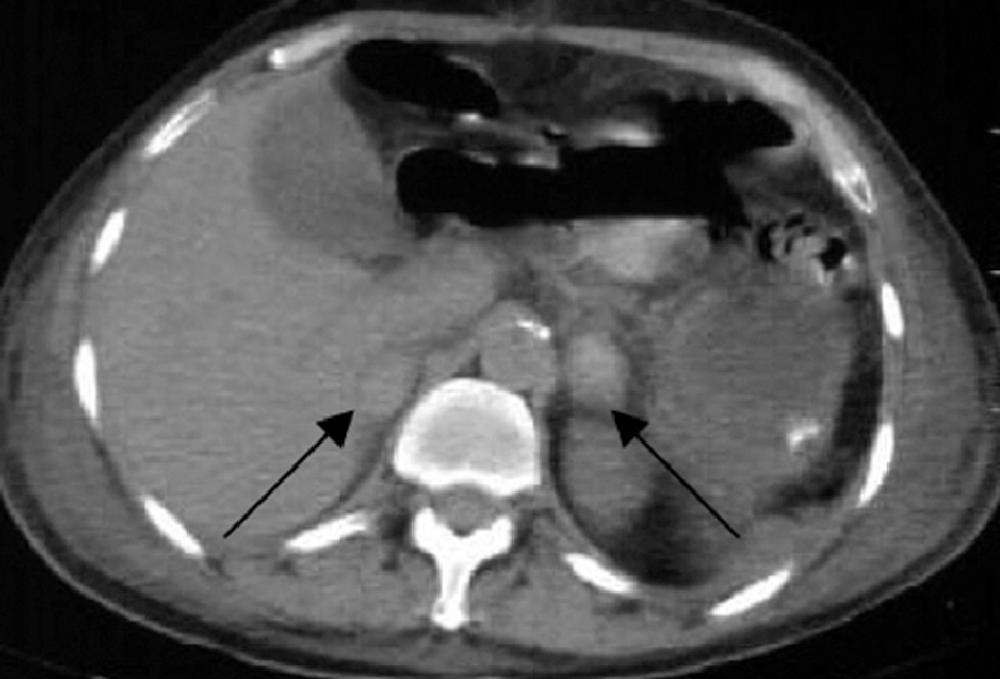
Axial computed tomography image demonstrating bilateral adrenal gland enlargements and diffuse hemorrhage (black arrows).
After starting intravenous hydrocortisone at a dose of 100 mg every 8 h, there was a dramatic improvement in his clinical condition, and he was weaned from all inotropes and vasopressor agents within 12 h. The stress dose of hydrocortisone regimen was tapered to oral prednisolone. His symptoms continued to improve, and within a week his abdominal pain subsided. He was finally discharged on day 9. He required no further steroid supplementation. Repeat computed tomography scan of the abdomen performed 4 wk later showed complete resolution of the previous findings. Retrospective interrogation revealed that there was no history of oral or inhaled steroids, illicit drugs, prescription medications, anticoagulants, herbal medications, or recent surgery.
Discussion
Adrenal hemorrhage, a rare cause of adrenal insufficiency, is often diagnosed by coincidence or after the onset of hypotensive crisis in a patient. The pathophysiology of bilateral adrenal hemorrhage is poorly understood; nevertheless, it is most likely multifactorial. 5 It is most frequently seen as a consequence of trauma—occurring, for instance, after extracorporeal shock-wave lithotripsy or electroconvulsive therapy. Additional predisposing factors that result in damage to the adrenal glands include chronic steroid use, prolonged administration of exogenous adrenocorticotropic hormone, sepsis, surgery, hypovolemia, coagulopathy, and burns. 6 Existing theories hypothesize that the adrenal glands may be particularly vulnerable to hemorrhage because of the anatomy of their vascular supply coupled with the factors described earlier.7,8 Although the adrenal glands are supplied by numerous arteries, they are drained by a single vein. Hence, any pathology that results in arteriolar dilation and pooling of blood in the capillary and venous system without adequate drainage could result in increased pressure in the adrenal glands and subsequent hemorrhage. This may eventually present as hyponatremia and hyperkalemia leading to Addisonian crisis, as noted in our case. 9
Warrell 10 described the case of a 17-y-old Burmese farmer bitten by a Russell's viper who experienced vomiting and diarrhea followed by unresponsiveness associated with grunting, grimacing, and extensor spasms of the limbs on the ninth day of hospital admission. These findings could have been explained by an acute episode of hypoglycemia. Therefore, serum glucose level was analyzed and found to be 18 mg⋅dL-1. Plasma cortisol was also analyzed during this acute episode and was found to be 5.4 μg⋅dL-1. Other hormones analyzed were luteinizing hormone (5.6 μIU⋅mL-1), growth hormone (9.7 μU⋅mL-1), and thyroid stimulating hormone (2.0 μIU⋅mL-1). These laboratory findings were suggestive of acute pituitary/adrenal insufficiency. 10
Than-Than et al 8 and Tun-Pe et al 11 reported the case of another 17-y-old Burmese farmer who was bitten on the foot by a Russell's viper. He was initially managed at a rural health clinic where he received an unknown amount of antivenom but was later transferred to a tertiary care hospital 21 h after the snakebite. On presentation to the tertiary care hospital, he had nausea and vomiting and an unrecordable blood pressure. He was found to have atrial tachycardia with ventricular ectopic beats and was subsequently administered 40 mL antivenom, 500 mL Rheomacrodex (a plasma expander), 0.25 mg digoxin, and 5 μg⋅kg⋅min-1 dopamine. Consequently, his blood pressure improved for a time. Over the course of his hospital admission, the patient had recurrent episodes of unconsciousness and fluctuations in blood pressure. He was further administered 25 mL of 50% dextrose and 300 mg of hydrocortisone, but he died 36.5 h after the snakebite. An autopsy performed 5 h after death revealed adrenal, pituitary, and epicardial hemorrhages. This case provides evidence that Russell's viper envenomation can result in adrenal hemorrhage.8,11
It has been found that Russell's viper venom (RVV) in the presence of lipoid cofactor clots the plasma of hemophiliacs and proconvertin (factor VII)-deficient patients within 5 s. However, RVV is unable to clot proaccelerin (factor V)-deficient plasma rapidly. Thus, the clotting behavior of the venom-lipoid is similar to convertin, which acts independently of proconvertin (factor VII) present in the plasma. 12
RVV is also nephrotoxic in vitro. One of the most surprising histopathologic changes observed is the lysis of the vascular smooth muscule, which may also augment the action of the so-called hemorrhagins present in RVV. 13 Vasolysis and mesangiolysis coupled with the action of hemorrhagins might lead to the leakage of blood into the adrenal glands of a susceptible individual. On the other hand, formation of venous clot in the draining vein resulting in bilateral adrenal hemorrhage is less likely in general.
In summary, our patient experienced adrenal hemorrhage resulting from the vasculotoxic effects of venom despite completing a course of antivenom therapy and achieving normalization of coagulation profile. He presented with the onset of acute abdominal pain with features of hypotension not responding to conventional inotropes, which can be a bedside indicator of adrenal insufficiency. Adrenal insufficiency and hemorrhage after Russell's viper envenomation is unique, and published literature on the topic is limited. In this case, a combination of early bite recognition, hospital-based supportive care, corticosteroid therapy, and timely administration of polyvalent antisnake venom resulted in a favorable clinical outcome.
Footnotes
Acknowledgments
The lead author thanks Dr E. Ravi, Consultant Radiologist, Sri Gokulam Hospital, Salem, Tamil Nadu, India, for interpreting this patient's CT imaging.