
Abstract
Greenland is not only the largest island in the world, it is also the least densely populated country on the globe. The majority of Greenland’s landmass lies within the Arctic Circle. Weather conditions in Arctic areas can be extreme, thus exposing locals and visitors to a high risk of acquiring frostbite injuries. More than two thirds of Greenland is covered by a permanent ice sheet, and temperatures can drop to below −70°C. In addition, frequent storms, occupational exposure, and alcohol all contribute to an increased risk for frostbite injury. Frostbite may cause major morbidity, including tissue loss and limb amputation. Hence, proper diagnosis and treatment of frostbite injuries is of utmost importance. We present 6 cases of frostbite injuries in Greenland, ranging from mild to severe frostbite in both locals and foreign visitors. The cases illustrate some of the known risk factors for frostbite injuries. The etiology, pathophysiology, clinical presentation, and recommended management of frostbite are summarized. Novel treatments for frostbite and frostbite sequelae are discussed in the context of the Greenlandic healthcare system. Furthermore, cultural aspects and reasons for a seemingly low incidence of frostbite injuries in Greenland are explored.
Introduction
The circumpolar areas are characterized by extreme weather conditions. Freezing temperatures, strong winds, snow, ice, and long polar nights with perpetual darkness are all mainstays of Arctic winters. Greenland constitutes a significant fraction of the landmass in the Arctic, with the majority of its 2,166,086 km2 located above the Arctic Circle (Figure 1). Around 85% of Greenland is covered by a permanent ice sheet, which measures around 3 km at its thickest. Due to the Arctic climate, temperatures can drop to −70°C (−94°F) in the coldest places.
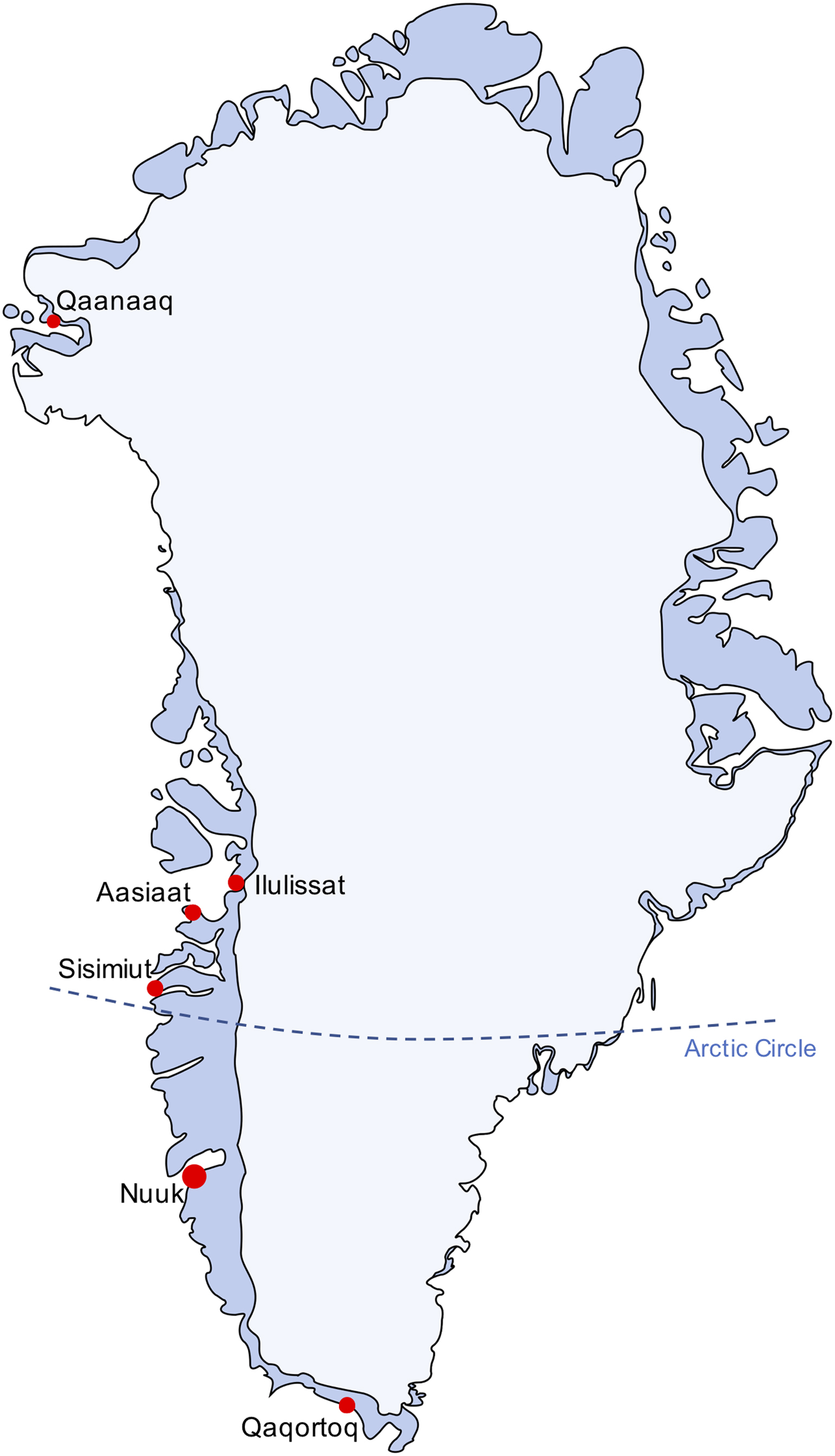
Map of Greenland. More than two thirds of Greenland’s landmass is covered by a permanent ice sheet. Around 17,000 of Greenland’s 57,000 inhabitants live in the capital city Nuuk. The other major cities are Sisimiut (5500 inhabitants), Ilulissat (4500 inhabitants), Qaqortoq (3500 inhabitants), Aasiaat (3000 inhabitants), and Qaanaaq (600 inhabitants), which is the most northern city in Greenland.
Greenland is a land of extremes. The largest island on the globe, it is also the least densely populated country in the world. Spanning 2600 km from north to south, the country is vast. The Greenlandic population of around 57,000 inhabitants is dispersed in settlements along the coastline; the 18 cities and 120 villages constitute small clusters of human habitation amidst the masses of rock and ice. No roads exist between cities in Greenland, the main transportation routes are by airplane, helicopter, boat, snowmobile, and dogsled. The majority of the Greenlandic Inuit employ themselves with fishing and hunting, which often requires multiple-day dogsled expeditions, lengthy hunting trips, and long boat excursions during all seasons of the year. In addition to prolonged exposure to icy winds and freezing temperatures in the wintertime, the journeys often venture deep into the Greenlandic icescape, and thus further away from medical care.
The healthcare system consists of 1 referral hospital, Queen Ingrid’s Hospital in the capital city Nuuk; 4 regional hospitals in the largest cities Sisimiut, Ilulissat, Qaqortoq, and Asiaat (Figure 1); 13 physician-staffed health clinics; and 48 rural health clinics staffed by a nurse or a healthcare worker. The regional hospitals serve as referral hospitals for the smaller health clinics. Physicians from the regional hospitals undertake medical visits to the regions’ rural settlements 2 to 4 times a year. In addition, a telemedical system is in service all over Greenland, allowing the rural-based nurse or healthcare worker to send electrocardiograms, clinical photographs, otoscopic images, stethoscopic sound files, and live video transmission to the regional hospital. In cases of medical emergency or trauma, the regional physician on call is contacted and can initiate evacuation by snowmobile, boat, helicopter, or airplane, depending on the level of critical illness of the patient. The geography, climate, and infrastructure can make the provision of healthcare in Greenland a logistical challenge, as patients from rural settlements who experience severe trauma or acute life-threatening illness might not be easily evacuated due to Arctic storms, heavy snowfall, low-visibility conditions, or limited availability of evacuation transportation vehicles.
Frostbite is a cold injury often encountered in circumpolar areas. 1 It occurs when body tissue is exposed to temperatures below 0°C (32°F) for long enough for ice crystals to form. The pathophysiology of frostbite has been extensively reviewed elsewhere2,3 and includes vasoconstriction, ischemia, ice crystal formation, and cell disintegration. Rewarming leads to reperfusion, causing an inflammatory surge, vascular leak, thrombosis, and embolization. Refreezing of thawed tissue triggers further inflammatory reactivity, resulting in significant tissue damage. 3
Clinically, frostbite injuries present with loss of sensation and a pale, waxy, bluish skin discoloration. Blisters and edema may be present in the affected areas. 3 Symptoms include numbness and paresthesia, followed upon rewarming by significant pain, to the extent that parenteral analgesia can be necessary. Frostbite injuries can be classified into 4 stages based on clinical findings. First-degree frostbite presents with numbness and erythema; a white, firm, elevated plaque in the frostbitten tissue; mild edema; no gross tissue infarction; and no blisters or necrosis. Second-degree frostbite presents with erythema, edema, and bullae containing clear or milky fluid. Tissue destruction is confined to the dermal layer. First- and second-degree frostbite represent superficial frostbite injuries, in which there is no or minimal anticipated tissue loss. 2 Third-degree frostbite is defined by tissue destruction extending to subcutaneous levels and presents with deep hemorrhagic blisters, skin necrosis, and a blue-gray discoloration. Fourth-degree frostbite affects deeper layers of tissue, including muscle and bone, and presents with little edema and deep red or cyanotic skin, which later becomes dry, black, and mummified. 3 Third- and fourth-degree frostbite comprise deep frostbite injuries, in which significant tissue loss should be anticipated. In addition to possible tissue loss, other long-term sequelae include chronic pain, increased vulnerability to future cold injuries, neuropathy, cold hypersensitivity, and diminished sensation and numbness. 3 –6 Chronic pain may be difficult to control. A novel case study reported reduced cold sensitivity and improved somatosensory nerve function after treatment with botulinum toxin in a soldier with bilateral second-degree frostbite in both hands. 7
Risk factors for the development of frostbite include temperature, wind chill, immersion, fatigue, malnutrition, smoking, alcohol and substance abuse, and medical conditions including peripheral vascular disease, diabetes, neuropathies, dementia, and mental illness.4,8 Digits, nose, cheeks, and ears are often affected. Frostbite largely affects healthy individuals aged 30 to 49 y, 9 ranging from military personnel operating in cold regions, industrial workers, and the homeless population, to people engaging in recreational activities such as skiing, hiking, mountaineering, and ice climbing. 4
Current guidelines for the management of frostbite injuries have recently been summarized by an expert panel; 2 however, evidence is often low quality due to a lack of randomized controlled trials. The proposed management of frostbite includes rewarming of the frostbitten extremity; administration of aspirin or ibuprofen; debridement of clear blisters; use of aloe vera gel; and splinting, dressing, and elevation of the affected body part. 3 Adjunctive therapies such as hyperbaric oxygen therapy, sympathectomy, thrombolytic therapy, and vasodilating agents such as iloprost, reserpine, pentoxiphylline, and buflomedil have been proposed as agents for frostbite treatment, although evidence is mainly limited to case reports and retrospective studies. 3 ,4,10–13 An interesting treatment protocol includes administration of aspirin and prostacyclin for severe frostbite injuries, and thrombolysis with recombinant tissue plasminogen activator for selected patients. 10
Depending on the degree of frostbite injury, amputation and severe morbidity may follow. The incidence of frostbite injuries in Greenland is currently unknown, but with the extreme weather conditions and thus increased risk of cold-induced injuries, knowledge of frostbite and its treatment is important for medical professionals and nonmedical visitors and inhabitants of the Arctic.
Case presentations
We present 6 cases of frostbite injury that occurred in the Arctic winter between December 2016 and February 2017 in Northwestern Greenland (Figure 1).
Case 1—Single digit frostbite, fisherman, Ilulissat
On a routine fishing trip, a 46-year-old fisherman experienced cold exposure of his right hand due to cold ambient temperature and wind. He was sailing in his motorboat in mid-winter and wore no gloves. One week later, he sought medical help due to severe pain and a dark discoloration on the tip of his right first finger. Upon examination, he presented with a 4×7 mm area of tissue necrosis due to second-degree frostbite on the tip of the right first digit (Figure 2).
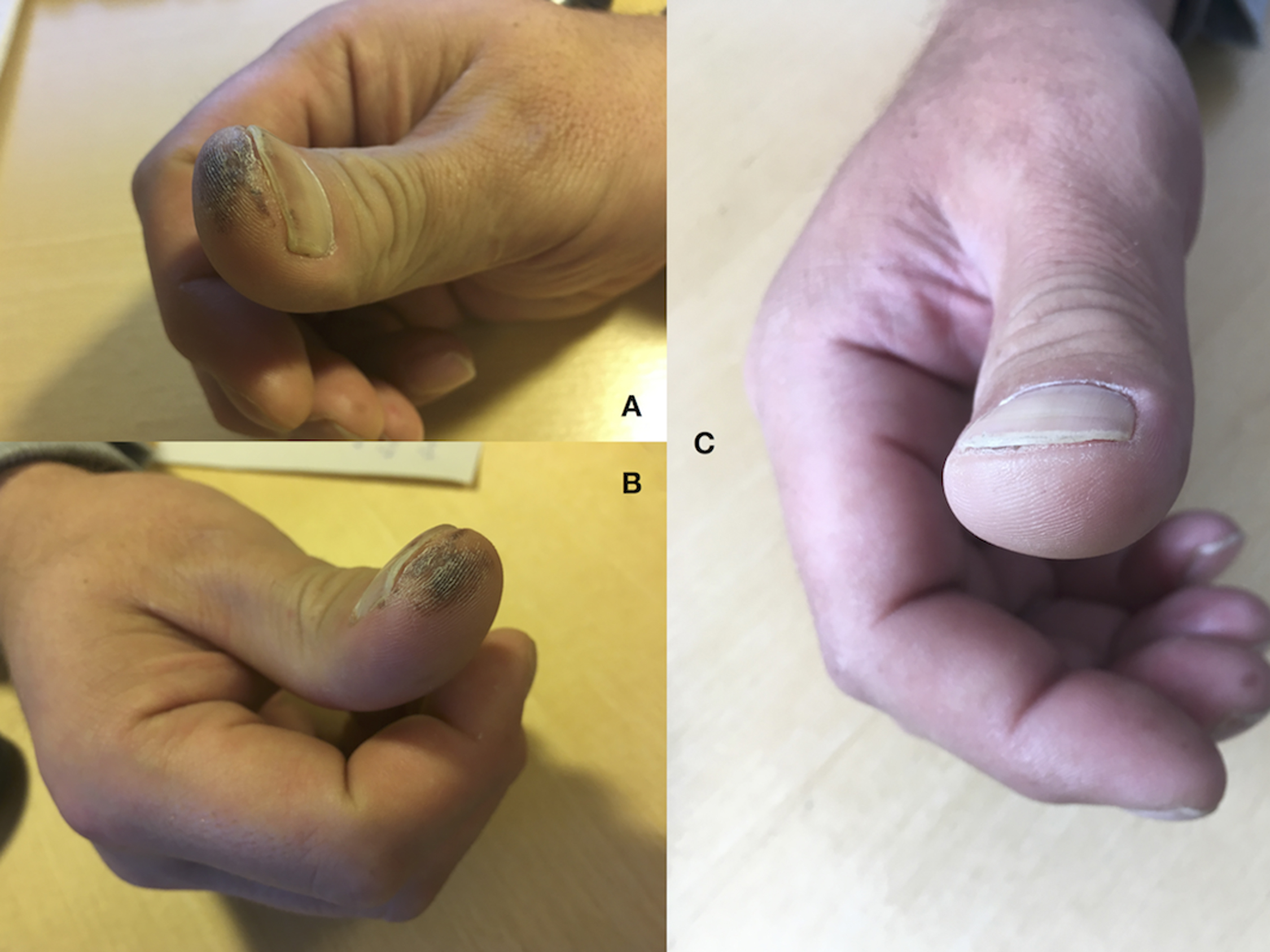
Case 1—Single digit frostbite, fisherman, Ilulissat. A, B, Frostbitten area at 2 wk postinjury. C, Digit at 6 wk postinjury.
The frostbite lesion was treated conservatively, and ibuprofen plus paracetamol was given for pain control. At follow-up 1 week later, he still experienced significant pain in the frostbitten area, interfering with his ability to work. Tramadol was added to his medical therapy but proved insufficient to obtain full pain control. After switching to gabapentin, he was able to commence work again but still experienced pain in the frostbitten area at 6-mo follow-up (Figure 2).
Case 2—Frostbite on foot sole, Ilulissat
About to leave from a party, a 31-year-old man was unable to find his right shoe. Tired and under the influence of alcohol, he decided to walk home without it. A few days later, he discovered a dark discoloration on the sole of his right forefoot and sought medical care. He was seen in the emergency room with second-degree frostbite under his right forefoot (Figure 3). He experienced no pain, had intact sensory function in the frostbitten area, and ambulated freely. He was treated conservatively with topical silver sulfadiazine, paraffin gauze, and bulky gauze dressings, changed several times weekly over the next 45 d. Wound debridement was carried out until the necrotic tissue was shed. Ten weeks after the initial injury, the wound had healed and there were no sequelae (Figure 3).

Case 2—Frostbite on footsole, Ilulissat Hospital A, Frostbite lesion 10 d postinjury. B, 10 wk later, there are no visible sequelae, and none reported by the patient.
Case 3—Multiple toe frostbite, Northern Greenland Expedition
During a multiweek ski expedition in Northern Greenland, a 44-year-old man experienced frostbite injuries on the toes of both his right and left foot. The injury arose from exposure to extremely cold temperatures and significant wind chill, combined with tight-fitting skiing boots and several layers of socks. Due to the nature of the expedition, this patient did not come under medical care until 3 mo postinjury and probably experienced several cycles of freeze–thaw–freeze during the expedition. Upon presentation at Ilulissat Hospital, the distal phalanx of the left first to third toes were necrotic, dry, and mummified, indicating third- or fourth-degree frostbite. Only the most distal tip of the right first and second toes were affected (Figure 4). The patient sought definitive care in his home country and was lost to follow-up.

Case 3—Multiple toe frostbite, Northern Greenland expedition. A, B, Fourth-degree frostbite injuries on the distal phalanx of the left first to third toe 3 mo postinjury. The toes are dry and necrotic with a clear demarcation line. C, Right forefoot, on which necrosis is only present on the tip of the most medial toes.
Case 4—Bilateral cheek frostbite during Arctic storm, Qaanaaq
In December 2016, a piteraq raged in the Northern Greenlandic village of Qaanaaq. A piteraq (meaning “that which attacks you” in Greenlandic) is an Arctic storm with winds reaching up to 50 m·s−1 (180 km·h−1, 112 mph). Due to an ambient temperature of −22°C (−7.6°F), the wind chill factor reached around −60°C (−76°F). A 32-year-old woman walked a few meters’ stretch from one house to another, covering her face and cheeks with a woolen scarf during the brief minutes she was exposed to the storm. Four days later, she presented in the health clinic with first-degree frostbite on both cheeks, with injuries most profound on the right side (Figure 5). She experienced no pain, and upon follow-up 5 mo later she had no long-term sequelae except for intermittent decreased sensibility on both cheeks.

Case 4—A, B, Bilateral cheek frostbite during Arctic storm, Qaanaaq. First-degree frostbite on both cheeks, 4 d after the Arctic storm during which the frostbite injuries arose. C, At follow-up 5 mo later, no tissue loss had occurred.
Case 5—Frostbite on both hands during Arctic storm, Qaanaaq
During the same piteraq in Qaanaaq, a 53-year-old man experienced second- or third-degree frostbite injury on both hands (Figure 6). Walking outside in the storm under the influence of alcohol, he fell several times and had difficulty getting up. This caused his bare hands to be exposed to the icy wind. He presented to the health clinic the following day. All digits were covered with clear bullae, some extending proximal to the metacarpophalangeal joint. Due to delayed presentation, rewarming was not initiated. He experienced severe pain in all digits, and parenteral opioid analgesia was necessary for pain control initially. All bullae were drained and debrided under sterile conditions. Topical silver sulfadiazine and barrier dressings were applied and changed daily. Pain control was managed with tramadol 50 mg 4 times daily, combined with paracetamol and ibuprofen. He was also given antibiotics prophylactically. Twenty days later, only a mild pinkish discoloration of the affected areas was visible (Figure 6). At latest follow-up 6 mo postinjury, there was full motor and sensory function in all digits, and no objective findings upon examination. However, he experienced chronic pain that was manageable with paracetamol and had increased cold sensitivity in all digits, due to which he wore gloves at all times, including indoors.

Case 5—Frostbite on both hands during Arctic storm, Qaanaaq. Second- or third-degree frostbite on both hands, with edema and multiple bullae filled with clear fluid on day 1. The patient was treated conservatively with a silver sulfadiazine ointment and wound dressings daily for 21 d. He experienced no tissue loss but had significant cold hypersensitivity after 6 mo. Note the slight discoloration of the nails as the only objective finding at 6 mo follow-up.
Case 6—Single digit frostbite, Qaanaaq
A 57-year-old man with several previous digit amputations due to frostbite injuries experienced a fourth-degree frostbite injury on the distal phalanx of his right third finger while ice fishing in cold and windy weather. The injury was treated conservatively, and due to pain in the frostbitten tissue, paracetamol, ibuprofen, and codeine were initiated while awaiting mummification and spontaneous amputation. Two months postinjury, the wound became infected. Oral antibiotic therapy was initiated and contained the infection; however, pain levels increased with need for tramadol for pain control. One month later, the patient still experienced severe pain, and although demarcated, the dry necrosis showed no signs of immediate spontaneous amputation (Figure 7). Two weeks later, swelling, edema, and purulent discharge was found upon examination, and surgical amputation at the midlevel of the middle phalanx was performed under local anesthesia. The nerve endings were identified, shortened, and revised. At follow-up 11 d postsurgery, the wound had healed, there were no signs of infection, and the patient experienced no pain.

Case 6—Single digit frostbite, Qaanaaq. A, B, Fourth-degree frostbite injury at 3 mo after the initial injury. The necrotic distal phalanx is clearly demarcated. C, Two weeks later there was edema and purulent discharge from the wound, indicating infection, and surgical amputation was performed.
Discussion
In Greenland, a large number of risk factors for developing frostbite injuries are present. Despite the harsh polar environment, the native Greenlandic Inuit have not only existed in the barren icy masses of the land, but have developed a thriving culture there as well. The traditional hunting and fishing lifestyle of the Greenlandic Inuit, using traditional kayaks and dogsleds, is still a common way of living in many parts of Greenland. Modernization, however, has brought snowmobiles and motorboats, which have largely replaced the traditional means of transportation. Both kayaking and driving a dogsled require a high degree of physical activity, as the dogsled musher often runs alongside the sled in steep terrain. Snowmobiling or sailing a motorboat, on the other hand, requires no physical exertion. Whether modernized transportation methods have altered the occurrence of frostbite injuries one can only guess, but long hours of physical inactivity on a fast-moving snowmobile or motorboat does pose a significant risk factor for developing frostbite injuries.
In the present article, 6 cases of frostbite injuries in Arctic Greenland are reported. One case describes a fisherman who acquired a superficial frostbite injury on a routine fishing trip in his motorboat. In this case, pain control was a challenge, and in spite of several types of pharmacological treatment, the patient still experienced chronic pain at 6-mo follow-up. Gabapentin, which is not usually the drug of choice for chronic pain management after frostbite injuries, 2 gave slightly better pain control than classical analgesics. At present, botulinum toxin is available in Greenland, but it has not yet been applied for the treatment of frostbite. 7
The Greenlandic weather conditions and occasional Arctic storms constitute a major risk factor for frostbite injuries. In 2 of the presented cases (cases 4 and 5), patients acquired frostbite injuries during a piteraq. The brief amount of time that the patient in case 4 was exposed to the wind demonstrates the power of wind chill factor. Even though she wore protection from the wind and was only exposed for a few minutes, she obtained first-degree frostbite on both cheeks. Case 5 illustrates this and another point—alcohol is a major risk factor for frostbite. Alcohol became easily available to the Greenlandic Inuit in the 1950s. Since the 1980s alcohol consumption has decreased by 50%, which also has caused a major reduction in alcohol-related morbidity. However, alcohol is still a significant cause of morbidity, as drinking patterns are characterized by heavy alcohol consumption over a couple of days, instead of daily drinking. Alcohol influences decision-making abilities in addition to motor skills, and this in combination with an extremely cold climate can lead to frostbite injuries, as case 2 also illustrates.
Travel to Arctic areas and expeditions into the lesser-visited corners of the planet are becoming more prevalent, with more people than ever seeking adventures off the beaten track. The number of people attempting to summit Mount Everest has increased drastically in recent years, 14 and skiing expeditions to the poles and other Arctic areas are offered by a variety of adventure companies. These are examples of humans taking on the extremes of nature, and many come out on the other side unscathed. However, exposure of the human body to the extremes of nature can have a price, as case 3 shows. Greater risks than frostbite are of course present, such as major trauma from crevasse falls, hypothermia, and so forth, but amputations due to frostbite injuries can cause extensive morbidity and a major impact on the life of an otherwise healthy individual.
The natural course of a severe frostbite injury is demarcation between viable and nonviable tissue after 1 to 3 mo and ultimately auto-amputation. 2 Premature amputation should be avoided and surgery delayed if possible, as natural tissue demarcation often reveals a larger amount of viable tissue than would initially be excepted, thus ensuring a better functional end result and lower levels of morbidity. Early surgical intervention can prove more damaging than beneficial.4,5 In case of infection, as seen in case 6, premature amputation may be necessary to halt further tissue damage. Also, auto-amputation may take several months, and surgical amputation may be considered after an appropriate period of time when proper demarcation has occurred. Amputation at this late stage might improve the functional result and shorten recovery time. The patient presented in case 6 had several previous amputations due to frostbite. Perhaps lower degrees of frostbite injuries had previously occurred in remaining digits, leaving them more susceptible to repeated frostbite injuries. The clinical picture of frostbite also comprises a challenge because infection, rewarming methods, and refreezing of tissue can turn less severe frostbite, or a nonfreezing cold injury, into becoming more critical (ie, a second-degree injury can progress to a third-degree injury). 3 –5 Cases 1 through 5 illustrate that conservative treatment performed properly over the long term should be encouraged to reduce tissue and limb loss. Full recovery can be achieved even with severe frostbite lesions.
Telemedicine provides a framework for fast and accurate diagnosis and planning of adequate treatment measures. The standard medical care for frostbite injuries in Greenland is conservative treatment, and newer medical interventions such as thrombolysis and vasodilating agents have not yet been used for frostbite in Greenland. Advanced telemedical technology is available throughout the country, allowing rural healthcare workers to consult on cases with physicians at local hospitals. In turn, the physicians at regional healthcare posts can contact regional or national specialists in surgery, or even international experts on frostbite, to best decide the further course of therapy. For cases of severe frostbite, novel therapies such as thrombolysis might significantly decrease the risk of amputation. 10 Thus, the framework for instituting educational programs on the treatment of frostbite exists and could ensure adequate treatment for frostbite regardless of the patient’s geographical location.
Frostbite is more prevalent in Arctic areas due to extreme weather conditions. The exact incidence of frostbite lesions in Arctic Greenland, however, is unknown. A Finnish study examining the incidence of frostbite from 1986 to 1995 found 1275 patients admitted to a hospital with frostbite injuries, corresponding to an incidence of 2.5/100,000 inhabitants. 15 In spite of multiple risk factors for frostbite in Greenland, in our clinical experience, the incidence of frostbite is relatively low. Over a 3-mo period in Northwestern Greenland, only a few cases of frostbite occurred. Many of the rural Greenlandic healthcare workers and nurses are highly experienced in treating cold-related injuries. In addition, the majority of patients with minor frostbite injuries probably do not seek medical care, as injuries might occur on multiple-day fishing or hunting trips far away from a health clinic. Thus, milder degrees of frostbite injuries in Greenland are likely never seen by doctors, and the incidence of frostbite injuries consequently is underestimated. The establishment of an Arctic Frostbite Registry, including data from remote clinic sites across the Arctic, could better elucidate the actual incidence of frostbite and allow for investigation into variation in occurrence between polar regions.
Even though the perceived rate of frostbite injuries is higher in Arctic Greenland than in other parts of the world, which appears logical considering the extreme weather conditions, we have the impression that the Inuit population better tolerates extremely low temperatures without being affected by frostbite, possibly due to certain factors within the population. 16 Given the prolonged exposure of hunters and fishermen to temperatures reaching −40°C (−40°F) in the Arctic winter, the scant occurrence of frostbite injuries in our region might point to a lower occurrence among the Greenlandic population, although repeated cold exposure does not decrease the risk of cold-related injury. 17 Future research into the thermoregulatory physiology of Greenlandic Inuit could shed light on whether the Inuit are genetically, anatomically, or physiologically more resilient to frostbite compared with other populations.
Conclusion
The presented cases illustrate that frostbite injuries are not normally life-threatening, unless disorders such as trauma, simultaneous hypothermia, or complications like sepsis occur. However, with frostbite comes the risk of severe morbidity due to loss of limbs and tissue. Hence, proper treatment and diagnosis of frostbite injuries is of utmost importance.
Author Contributions: Acquisition of the images and clinical descriptions (AKL and LP); drafting of the manuscript (AKL and LP); critical revision of the manuscript (AKL and LP); and approval of final manuscript (AKL and LP).
Financial/Material Support: None.
Disclosures: None.