
Abstract
Introduction
The Megalopyge opercularis caterpillar is covered with spines that break off and release venom on contact, resulting in severe pain, erythema, rash, and other adverse effects. In Texas, these caterpillars are abundant and of potential health threat. This study describes M opercularis caterpillar stings reported to Texas poison centers.
Methods
Cases were M opercularis caterpillar stings reported to Texas poison centers during 2000–2016. The distribution of stings was determined related to exposure circumstances and management.
Results
There were 3484 M opercularis caterpillar stings reported during 2000–2016. The annual number of stings did not consistently change over the 17-year time period. The monthly number of stings was highest in July (12%) and October to November (59%). The patients were female in 53% of cases and aged 20 years or more in 56%. The sting occurred at the patient’s own residence in 91% of cases. The patients were managed outside of a healthcare facility in 89% of cases; 93% of the patients were known or expected to have no or at most minor clinical effects. Dermal clinical effects were reported in 90% of cases, the most common being irritation/pain (84%), puncture/wound (45%), erythema/flushed (29%), and edema (15%).
Conclusions
M opercularis caterpillar stings reported to Texas poison centers were more frequently reported in July and October to November. Most of the patients were adults. The majority of patients were managed outside of healthcare facilities and did not have serious outcomes. Most of the adverse clinical effects were dermal in nature.
Introduction
The Megalopyge opercularis caterpillar, commonly known as the puss caterpillar, asp, wooly asp, Italian asp, opossum bug, wooly slug, and el perrito (the puppy), is one of the most venomous caterpillars in North America. 1 M opercularis is primarily found in the southeastern United States as far north as Virginia and as far west as Texas. 1−3 The M opercularis caterpillar is tear-shaped, 2 cm in length, and 1 cm in width.1,3 It may be white, gray, light tan, yellow, reddish-brown, or a mixture of colors (Figure 1). 1 Two generations of M opercularis caterpillars are produced each year, the first around June to July and the second during September to October. 3

Megalopyge opercularis caterpillar. From
The M opercularis caterpillar has fur that forms a midline ridge along the back. Beneath the fur are concealed tubercular ridges or verrucae (rows of sharp, short, needle-like spines). When these verrucae come into contact with the skin, they break off, embed themselves, and discharge venom.1,3 Contact almost immediately causes severe, intense, burning pain and erythema or rash. Within hours, hemorrhagic vesicles or pustules appear and last for several days. The person may experience numbness in the affected body part, headache, fever, nausea, vomiting, and abdominal pain that may last for several days. 1−5 Hundreds or thousands of M opercularis caterpillar stings may occur each year. 3 Treatment may involve applying tape to the site and pulling it off to remove the spines (stripping), ice packs, antihistamines, and baking soda. 2 ,4,5
The published literature on M opercularis caterpillar stings mostly consists of case reports 6 –12 or a relatively small number of cases. 2 ,4,13 The objective of this investigation was to describe M opercularis caterpillar stings reported to poison centers in Texas, a state where M opercularis caterpillars have been noted to be particularly abundant. 1−3 One previous study characterized M opercularis caterpillar stings using Texas poison center data 4 ; however, that study covered only part of the state and included data from a single year.
Methods
The case definition for the study was M opercularis caterpillar stings reported to the Texas Poison Center Network (TPCN) during 2000–2016. The TPCN consists of 6 poison centers that together serve the entire state, which has a current population of over 25 million. In the United States, a poison center is a telephone communications system that assists in the management of potentially adverse exposures to a variety of substances and products. The poison centers of the TPCN use a common electronic database to document information on all received calls in a consistent manner. The data variables and coding in this database were standardized by the American Association of Poison Control Centers. 14
Cases involving substances or products in addition to the caterpillar sting (n=7) were included in the study. Patients who were not followed to a final medical outcome also were included to provide medical outcome information for all cases. The distribution of cases was determined for the year and month of the sting, caller county, patient age and sex, exposure site, management site, medical outcome, adverse clinical effects, and treatments. The TPCN database does not contain a data field specifically for the body part where a bite or sting might occur. This information might be recorded in the “notes” text field, but if so, it is not documented consistently. Thus, the body part where the M opercularis sting occurred was not analyzed.
The caller county is the county from which the initial call to the TPCN originated. This may not be the county where the sting occurred or where the patient resides and may not be known for all cases. The medical outcome or severity of an exposure is assigned by the poison center staff and is based on the observed or anticipated adverse clinical effects. Medical outcome is classified according to the following criteria: no effect (no symptoms due to exposure), minor effect (some minimally troublesome symptoms), moderate effect (more pronounced, prolonged symptoms), major effect (symptoms that are life-threatening or cause significant disability or disfigurement), and death. A portion of exposures are not followed to a final medical outcome because of resource constraints or the inability to obtain subsequent information on the patient. In these instances, the poison center staff records the expected outcome of the exposure. These expected outcomes are grouped into the following categories: not followed but judged as nontoxic exposure (symptoms not expected), not followed but minimal symptoms possible (no more than minor symptoms possible), and unable to follow but judged as a potentially toxic exposure. Another medical outcome category is unrelated effect, in which the exposure was probably not responsible for the symptoms.
In the TPCN database, there are over 130 checkboxes for recording specific adverse clinical effects (eg, hypertension, nausea, vomiting, headache, fever). If a patient has a clinical effect that does not correspond to one of these checkboxes, it is assigned a checkbox for “other.” Also, there are over 60 checkboxes for specific treatments or therapies (eg, activated charcoal, food/snack, benzodiazepines, intravenous fluids) and one checkbox for “other.” The clinical effects and treatments may be documented in the “notes” text field; however, this does not always occur. 15 Analysis of the clinical effects and treatments was restricted to the checkboxes.
The Texas Department of State Health Services institutional review board considers this research exempt from ethical review.
Results
A total of 3484 M opercularis caterpillar stings were identified during 2000–2016. The annual number of stings varied from year to year, from 43 to 416, with no consistent increase or decrease over the 17-year period (Figure 2). Table 1 presents the monthly distribution of M opercularis caterpillar stings. Peaks in the number of stings occurred in July (12%) and in October to November (59%) compared with the rest of the year.
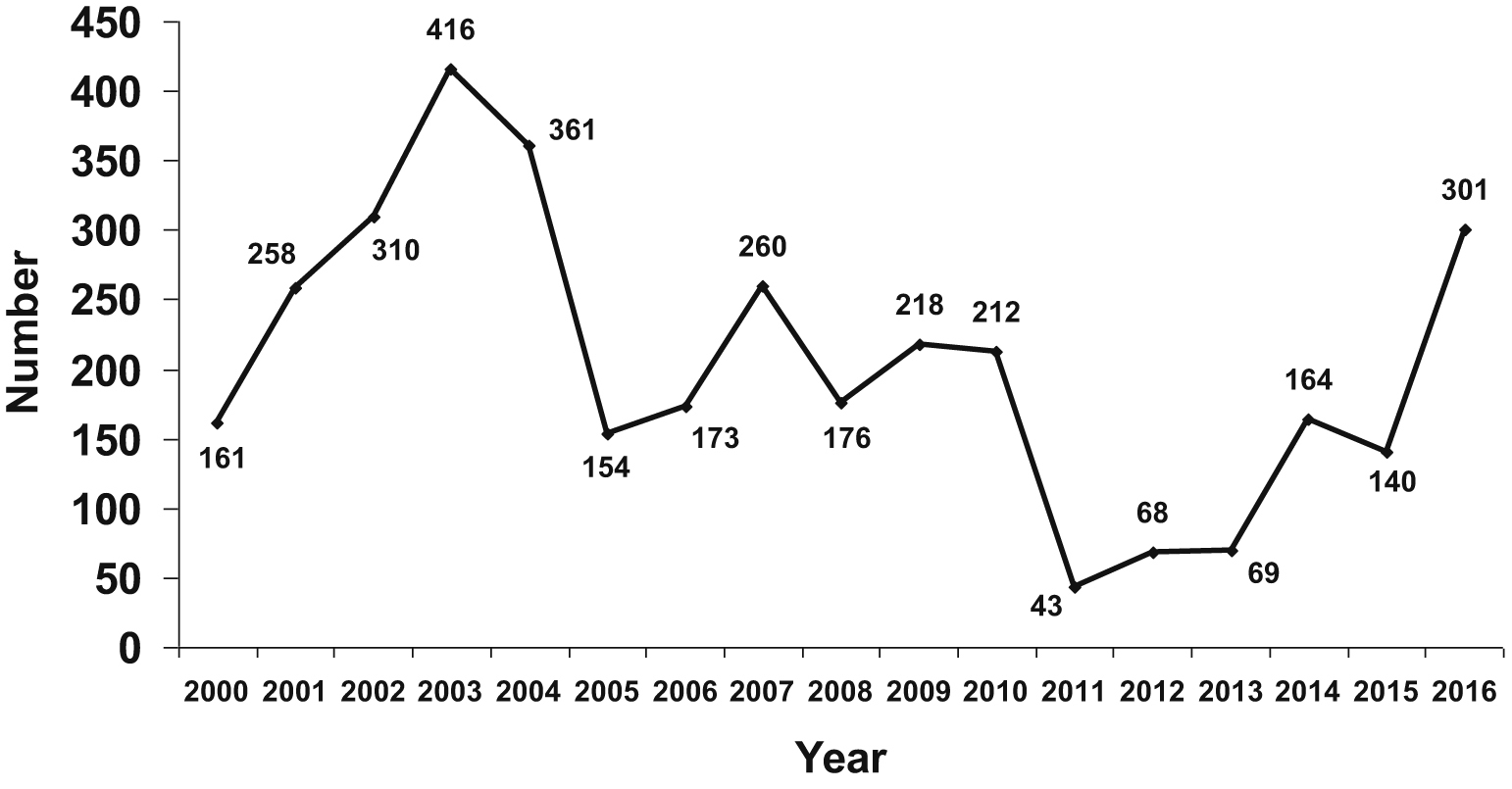
Megalopyge opercularis caterpillar stings reported to the Texas Poison Center Network during 2000–2016 by year.
Monthly distribution of Megalopyge opercularis caterpillar stings reported to the Texas Poison Center Network during 2000–2016
M opercularis caterpillar stings were reported from 133 of the 254 Texas counties (Figure 3). Most reports came from the central and eastern portions of Texas with relatively few coming from the western part of the state. The counties reporting the highest number of stings were those in which the largest cities in central and eastern Texas are located (Table 2); 9 counties accounted for almost two thirds of the reported stings.
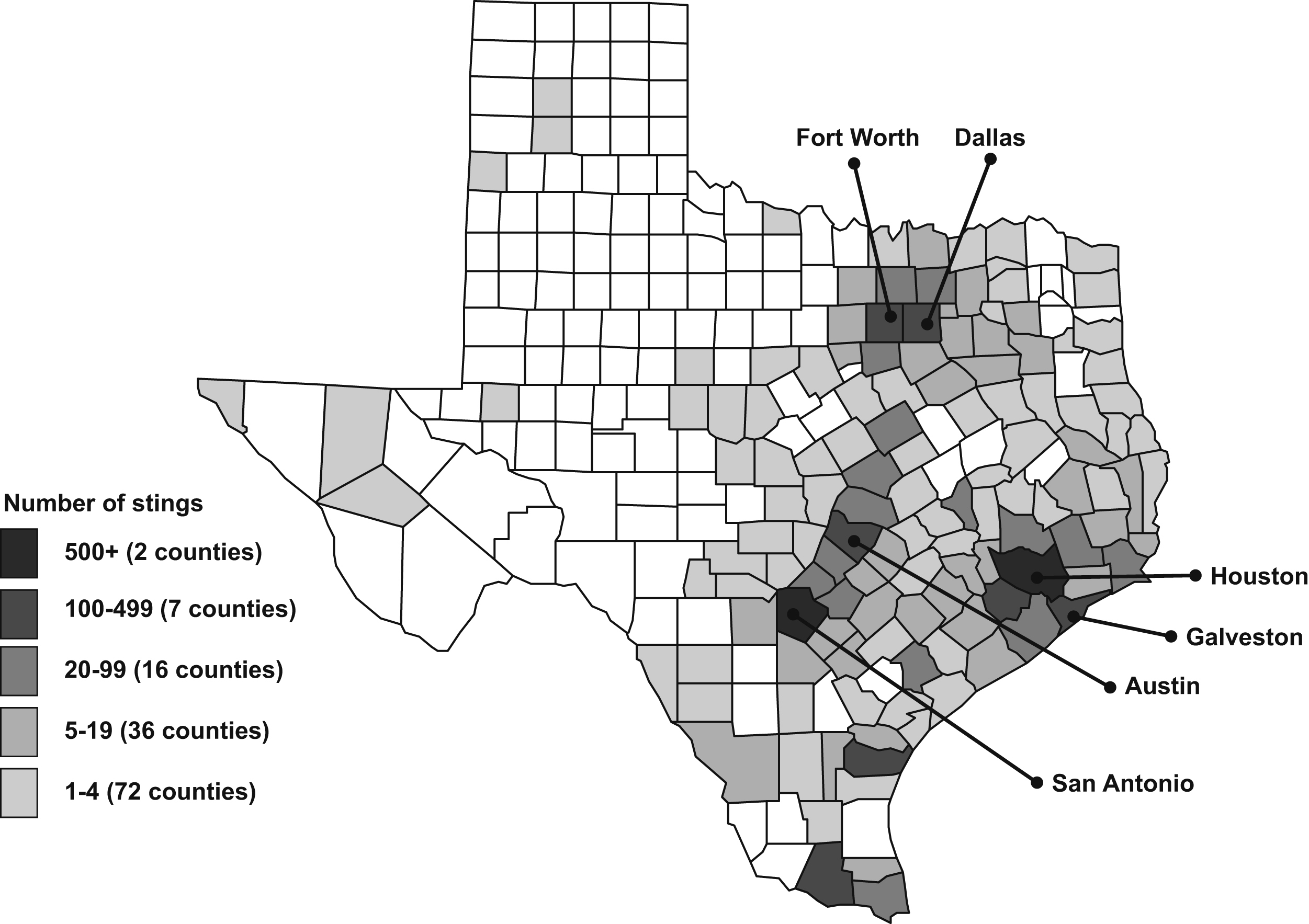
Megalopyge opercularis caterpillar stings reported to the Texas Poison Center Network during 2000–2016 by caller county.
Megalopyge opercularis caterpillar stings reported to the Texas Poison Center Network during 2000–2016 by most common caller counties
The patients were female in 1845 (53%) cases, male in 1629 (47%), and of unknown sex in 10 (0.3%). The patient age distribution was 5 years or less (580, 17%), 6–12 years (615, 18%), 13–19 years (300, 9%), 20 years or more (1940, 56%), and unknown age (49, 1.4%). The majority (3167, 91%) of the stings occurred at the patient’s own residence, 84 (2.4%) at another residence, 81 (2.3%) in a public area, 76 (2.2%) at school, 46 (1.3%) at the workplace, 12 (0.3%) at another location, and 18 (0.5%) at an unknown location.
Most (3117, 89%) of the patients were managed on site (outside of a healthcare facility), 322 (9%) were already at or en route to a healthcare facility when the poison center was contacted, 19 (0.5%) were referred to a healthcare facility by the poison center, 23 (0.7%) were managed at an unspecified other location, and 3 (0.1%) were managed at an unknown location. The distribution by medical outcome was 45 (1.3%) no effect, 1002 (29%) minor effect, 203 (6%) moderate effect, 31 (0.9%) not followed but judged as nontoxic exposure (clinical effects not expected), 2171 (62%) not followed but minimal clinical effects possible (no more than minor effect possible), 25 (0.7%) unable to follow but judged as a potentially toxic exposure, and 7 (0.2%) unrelated effect. No major effects or deaths were reported.
Table 3 lists the reported adverse clinical effects. The most frequently reported clinical effects were dermal in nature, particularly irritation/pain, puncture/wound, erythema/flushed, and edema. Gastrointestinal (nausea, vomiting), neurologic (numbness), cardiovascular, ocular, and respiratory clinical effects also were reported, but only in a small fraction of cases.
Adverse clinical effects with Megalopyge opercularis caterpillar stings reported to the Texas Poison Center Network during 2000–2016
A case may include more than 1 clinical effect.
The most commonly reported treatments were dilution/irrigation/wash, antihistamines, steroids, and antibiotics (Table 4). Unspecified other treatments were reported in over two-thirds of the cases.
Treatments with Megalopyge opercularis caterpillar stings reported to the Texas Poison Center Network during 2000–2016
A case may include more than 1 treatment.
Discussion
This study described over 3000 M opercularis caterpillar stings reported to Texas poison centers over a 17-year period. M opercularis caterpillars are among the most venomous caterpillars in North America, with contact resulting in severe pain, erythema, rash, and other adverse effects. 1−5 It is important to understand its distribution, seasonal variation, and range of symptoms to assist in diagnosis and prevention.
The number of reported M opercularis caterpillar stings varied from year to year. Previous reports have observed the abundance of the caterpillar to vary annually.3,16 The abundance of the caterpillar may be related to weather, the availability of food, and the relative number of M opercularis caterpillar predators.3,16 Although M opercularis caterpillar stings were reported throughout the year, reports of stings demonstrated a bimodal seasonal pattern with peaks occurring in July and again in October to November, with the peak being higher in the latter 2-month period. The double hump in the seasonal pattern is consistent with previous observations that the caterpillar has 2 generations each year, the first developing in summer and the second in fall, with the caterpillars seeming to be especially abundant during September to October. 3 Education and prevention activities might target these 2 time periods for greatest effect.
The majority of M opercularis caterpillar stings were reported from central and eastern Texas, with very few from western Texas. This agrees with a previous Texas investigation that reported the caterpillar from Dallas in north-central Texas southward in the central-eastern part of the state. 3 Moreover, a large portion of the M opercularis caterpillar stings were reported from those counties in which the largest cities in this region are located. This information may be useful in targeting education and prevention activities to those geographic areas where M opercularis caterpillar stings are most likely to occur.
The majority of stings occurred at the patient’s own residence, and most patients were managed outside of healthcare facilities. This is consistent with a 1958 survey of Texas physicians, which reported that only 0.4% of M opercularis patients with caterpillar sting were hospitalized. 5 This might be expected considering 93% of patients were known or expected to have no or at most minor clinical effects. The reported adverse clinical effects were predominantly dermal in nature and included irritation/pain, puncture/wound, erythema/flushed, and edema. Clinical effects involving other systems such as nausea, vomiting, abdominal pain, numbness, dizziness/vertigo, headache, and fever/hyperthermia were reported, however, these were found in only a small number of the patients. The clinical effects reported in this investigation are consistent with the literature. 1−5
The most frequently reported treatments were dilution/irrigation/wash and administration of antihistamines, treatments advocated in the literature.2,4 The literature also suggests other treatments, such as applying tape to the site and pulling it off to remove spines and applying ice packs and baking soda. 2 ,4,5 Such treatments might have been recommended and/or used with patients in the present study; however, the TPCN does not specifically track these treatments. It is possible these treatments were listed as “other,” which was used in 69% of the cases.
Limitations
There are limitations to this investigation. Reporting of M opercularis caterpillar stings to the TPCN is voluntary, and those that are reported may not be representative of all such exposures that occur in Texas. Moreover, the report that an M opercularis caterpillar was involved in the sting was usually based on information provided by the caller and not independently confirmed by a healthcare provider. Furthermore, the majority of patients were not followed to a final medical outcome.
Conclusions
M opercularis caterpillar stings reported to Texas poison centers varied from year to year but were more frequently reported in July and October to November. The stings primarily came from the central and eastern portions of the state, particularly from counties with major cities. Most patients were adults, and the majority of the stings occurred at the patient’s own residence. Most of the patients were managed outside of healthcare facilities and did not have serious outcomes. Most of the adverse clinical effects were dermal in nature.
Future research efforts may examine poison center data from other states or nationally, utilize other databases (eg, hospital visits), and investigate information not easily identifiable in United States poison center databases (eg, body part affected).
If an M opercularis caterpillar sting occurs in the US, it may be helpful to contact a poison center at 1-800-222-1222 for assistance in treatment or triage. M opercularis caterpillar stings may be managed by removal of the spines using adhesive tape. A mixture of one part bleach to 9 parts water may be used as a wound compress/soak for 15 min. Antihistamines, corticosteroids, or analgesics may be given. The wound may be kept clean with mild soap and water and antibiotic ointment applied.
Author Contributions: Study concept and design (MF); obtaining funding (MF); acquisition of the data (MF); analysis of the data (MF); drafting of the manuscript (MF); critical revision of the manuscript (MF); approval of final manuscript (MF).
Financial/Material Support: None.
Disclosures: None.