
Abstract
Stingray injuries to the chest are rare but potentially life-threatening. They may occur in remote areas where advanced emergency healthcare services are unavailable. We describe the case of a 24-year-old man with tension pneumothorax due to a Himantura fai stingray injury to the left chest. The chest wound was unremarkable, with no external bleeding or evidence of a foreign body. Decompression was performed at the scene with an improvised knife procedure and a hollow writing pen, which served as a chest tube. At the local hospital, a standard-sized chest tube was inserted, the wound cleaned, and the patient given antibiotics active against marine organisms. Computed tomography visualized the stinger and revealed hemopneumothorax and pneumomediastinum. The local hospital did not have a thoracic surgeon, and the patient was transferred to a larger hospital with a thoracic surgery center. After surgical removal of the stinger, segmental lung resection was required to control bleeding. Management of life-threatening stingray injuries to the chest should begin at the scene. After stabilization, the patient should be transferred to a hospital equipped for cardiovascular and thoracic surgery. Surgery may be required to remove the retroserrated stinger and can be challenging.
Introduction
The growing worldwide interest in sea sports is increasing opportunities for human contact with marine animals, some of which may be dangerous. Stingrays are fish with 1 or more stingers at the base of their tail. They are ubiquitous in all temperate and tropical oceans worldwide and are even found in many tropical freshwater river systems. They are divided into 2 superfamilies: Myliobatoidea and Dasytoidea. Myliobatoidea have a stinger measuring 5 to 12 cm in length; that of Dasytoidea can be up to 30 cm long. The spine is composed of bonelike cartilaginous material. 1
Whiptail stingrays flick their tail up to sting their victims. The stinger may break off and remain in the wound. The stinger is hard, with a sharp, pointed tip and retroserrated edges. Venom glands are located along the underside of the stinger. Thus, the injury consists of both tissue damage and envenomation. The venom causes severe pain. In the United States, 1500 to 2000 stingray injuries are reported per year. Most stingray injuries affect the lower legs or arms, where they usually cause limited damage.1,2 Injuries to the chest or abdomen, however, can be life-threatening. 3 –7
Mayotte is an archipelago in the Indian Ocean located in the Mozambique Channel between northwestern Madagascar and northeastern Mozambique. Several stingray genera are found in the waters around these islands: 6 Dasytoidea (Himantura fai, Himantura uarnak, Neotrygon kuhlii, Pastinachus sephen, Taeniurops meyeni, and Urogymnus asperrimus) and 1 Myliobatoidea (Myliobatis aquila). 8
We describe the case of a 24-year-old man with tension pneumothorax due to a stingray injury to the left chest while spearfishing in Mayotte.
Case report
A 24-year-old man who was spearfishing near an isolated coral reef saw an H fai stingray (Dasytoidea family) and swam with it. The stingray struck him suddenly, first in the neck and then in the left chest. He immediately developed respiratory distress but was able to call for help and was rescued by 2 witnesses. Two doctors were nearby and immediately came to assist. The victim had difficulty speaking but was able to report the stingray attack. He had respiratory distress, agitation, severe facial and cervical edema, and a blowing puncture wound in the neck over the trachea. He was brought up on the beach, where there was no telephone network connection or rapid access to emergency medical services.
Examination revealed another puncture wound in the left thorax, with no air escaping from it and no external bleeding. This wound was 0.5 cm in diameter, with no visible foreign body. The cervical edema extended down to the left upper thorax. Crepitus was felt on palpation. Breath sounds were absent over the left hemithorax. The respiratory distress rapidly worsened, with bradypnoea, obtundation, and tachycardia. On inspection, thoracic expansion was only occurring on the right side. A left-sided tension pneumothorax due to stingray injury was suspected.
Decompression was achieved by inserting a fillet knife into the fifth intercostal space on the midaxillary line (Figure 1). A hissing sound was heard through the wound. A pen was then inserted to serve as a chest tube (Figure 2). Sterile technique was impossible on the scene. The patient began to improve, with regression of the subcutaneous emphysema and an increased breathing rate. When emergency medical assistance arrived 1 hour later, he was stable with a heart rate of 109 beats·min−1, breathing rate of 22 breaths·min−1, blood pressure of 133/84 mm Hg, and a blood oxygen saturation level of 97%. Morphine was initiated, and the pen was replaced by a chest tube.

Fillet knife used to decompress the tension pneumothorax.
Pen used as a chest tube.
The patient was transferred by helicopter to Mayotte hospital. This local hospital has 371 beds, including an intensive care unit and a surgical department with a 24/7 medical staffing surgical block. A radiology department there can perform standard radiology, computed tomography, and magnetic resonance imaging. The hospital also has an endoscopy department and a laboratory.
Laboratory blood analysis, including hemoglobin level, was normal. Chest radiography was not performed. Computed tomography of the chest revealed pneumomediastinum, left hemopneumothorax with contusion of the upper lobe, cervicothoracic emphysema (Figure 3), and a foreign body. Computed tomography reconstruction was performed at the same time and revealed an 8-cm–long, slender, rodlike, intrathoracic foreign body extending from the first left intercostal space to the center of the chest (Figure 4). The patient was transferred to the intensive care unit, where antibiotic therapy with piperacillin and tazobactam were started. The neck wound was cleaned, disinfected, and dressed.

Computed tomography of the chest, showing the intrathoracic foreign body, pneumomediastinum, left hemopneumothorax, contusion of the superior lung lobe, and thoracic emphysema.
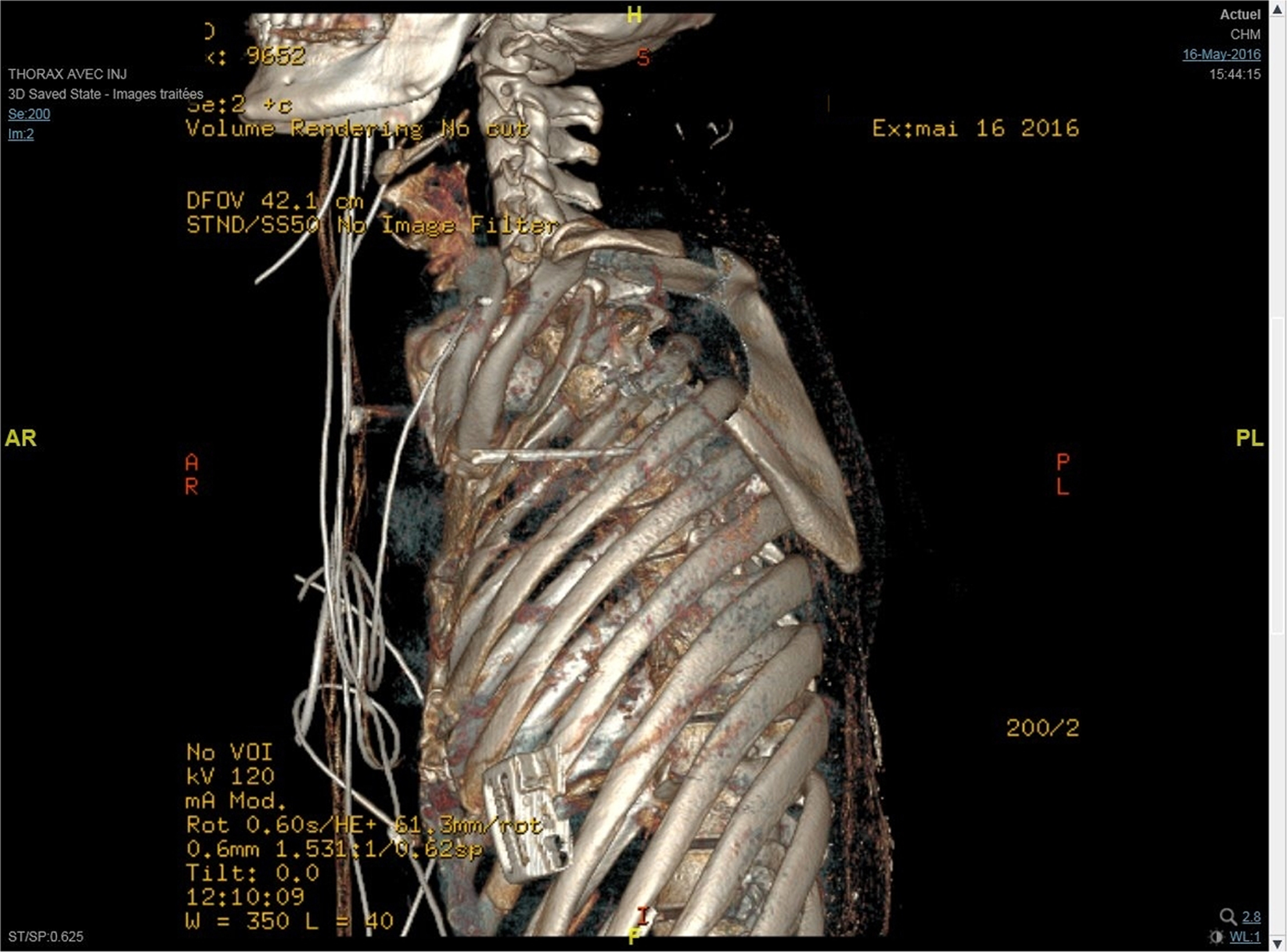
Three-dimensional computed tomography scan; note the foreign body extending from the first left intercostal space to the center of the chest.
Unfortunately, there is no thoracic surgeon in Mayotte Hospital and there was only 1 available commercial flight per day for transfer to a higher level of care. Seats are booked every day on commercial flights for medical transfer. If the patient needs to lie down during transfer, more seats are requisitioned and a stretcher is placed on them. When the patient arrived at Mayotte Hospital, the plane had already left. He was transported the next day by commercial flight (air ambulance) to a hospital on Reunion Island, 1500 km away, where the nearest thoracic surgery center is located. The risk of clinical deterioration during the flight was considered. The patient was thus transferred with a 1-way valve on the thoracic drain and given supplemental oxygen. At the Reunion Island hospital, bronchoscopy revealed a puncture wound in the anterior aspect of the trachea. No esophageal wound was seen during upper digestive tract endoscopy. Thoracoscopy identified a spine in the left lung (Figure 5). Removal of the spine through the thoracic trocar was followed by severe bleeding, which required segmental pulmonary resection. The patient was discharged 6 days after surgery. One year later he was in good health, with no complications.
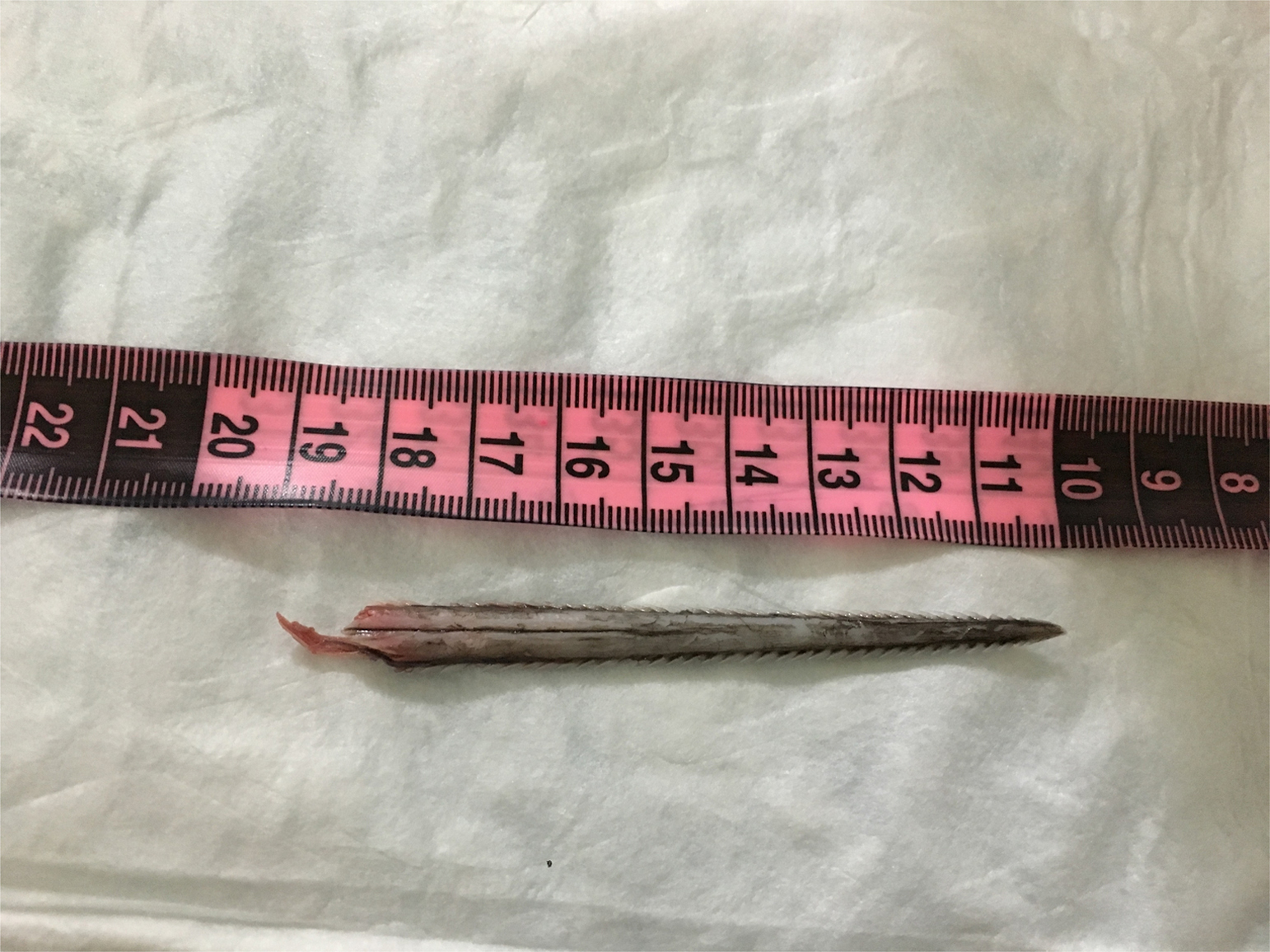
Stinger removed from the lung.
Discussion
Most stingray injuries may be preventable through education and avoidance. When disturbed, stingrays usually swim away rather than attack. Divers should not intentionally induce encounters with stingrays and should leave an exit path for the animal. Diving suits and diving boots do not prevent stinger penetration.
The management of life-threatening stingray injuries to the chest should begin at the scene. The victim should be removed from the water as soon as possible. Potentially life-threatening organ failure should be assessed and treated immediately. Tension pneumothorax requires emergency decompression. Normally, we use a needle with a large-bore angiocatheter introduced into the fourth/fifth intercostal space over the anterior axillary line. 9 When even improvised tools are unavailable, decompression can be performed by finger thoracostomy in the prehospital setting. 10 The case we describe highlights an improvised method consisting of decompression with a knife followed by insertion of a pen to serve as a chest tube. This modified prehospital intervention proved to be life-saving in this case and could potentially be so in future cases in remote settings with limited resources.
Stingray injury results in direct trauma and venom injection, causing local inflammation and severe pain. The venom is reported to be heat-labile. Some experts recommend immediate submersion of the wound in the warmest water the victim can tolerate for 90 min 1 However, scientific evidence demonstrating beneficial effect is limited.11,12 In the case we describe, hot water was unavailable on the scene. Analgesia should be provided quickly.
As soon as the clinical situation allows, the patient should be transferred to a hospital. Simple x-ray radiography may help to locate the cartilaginous barb, which is usually radiopaque.1,7 If the stinger is still in the wound, it may prove difficult to extract without causing additional tissue damage. Surgical exploration may be necessary to remove all fragments.
Thoracic and cervical wounds caused by a stingray barb are rare but can be fatal. Steve Irwin (“The Crocodile Hunter”) was the most famous victim. He was stung in the chest by a stingray barb while filming an underwater documentary. He pulled the barb out immediately but died within minutes due to cardiac tamponade. Another unusual death by cardiac tamponade occurred in North Queensland. A 12-year-old boy died 6 days after being injured in his left chest by a stingray. First examination revealed a 2-cm, curved laceration under the left nipple with slow bleeding. After controlling the bleeding and cleaning with chlorhexidine, the visible wound was unremarkable. Chest radiograph was performed and described to be normal. He was admitted to hospital for observation. He was stable with no complaints or cough and discharged home after 24 h. His father described continuous improvement until 6 days after the injury, when he suddenly developed cardiac arrest. An autopsy was performed the same day. The cause of death was cardiac tamponade due to chemical myocardial necrosis from a penetrating stingray wound. 13
Three cases of traumatic pneumothorax caused by stingrays have been reported, but no cases of tension pneumothorax. An 81-year-old man survived a transfixing cardiac injury and pneumothorax caused by a stinger barb. 6 Jhamb and Corsetti reported the case of a 47-year-old man who survived a stingray wound with liver injury and pneumothorax. 7 Recently, Suzuki et al reported a case of traumatic pneumothorax after a neck injury, presumably caused by a stingray barb. 12 When the injury is in the chest or abdomen, hemodynamic and respiratory stabilization must be achieved before transferring the patient to a hospital equipped for cardiovascular and thoracic surgery. 2
The marine environment is also inhabited by potentially pathogenic microorganisms, including the gram-negative bacterial species Vibrio and Alteromonas. Patients with deep stingray wounds should be given prophylactic antibiotics active against marine microorganisms, such as trimethoprim/sulfamethoxazole or a third-generation cephalosporin.1,14 Tetanus immunization is recommended, as for any wound.
Our case highlights the risk of life-threatening thoracic injuries from stingrays and the multidisciplinary nature of their management. Such injuries may constitute an extreme medical emergency, even though the external wound can appear unremarkable during the first hours. Tension pneumothorax must be recognized and quickly decompressed. If surgical instruments are unavailable, a simple knife and a pen with a hollow shaft can prove helpful and temporizing. Decompression can also be done by finger thoracostomy. 10 Surgery may be required to remove the retroserrated stinger.
Acknowledgments: The authors thank François Angoulvant and Loïc Epelboin for technical assistance.
Author Contributions: Patient care (SL, OM, AR, PD, HC, CL); drafting of case report (SL, RB).
Financial/Material Support: None.
Disclosures: None.