
Abstract
Canyoning is a recreational activity that has increased in popularity in the last decade in Europe and North America, resulting in up to 40% of the total search and rescue costs in some geographic locations. The International Commission for Mountain Emergency Medicine convened an expert panel to develop recommendations for on-site management and transport of patients in canyoning incidents. The goal of the current review is to provide guidance to healthcare providers and canyoning rescue professionals about best practices for rescue and medical treatment through the evaluation of the existing best evidence, focusing on the unique combination of remoteness, water exposure, limited on-site patient management options, and technically challenging terrain. Recommendations are graded on the basis of quality of supporting evidence according to the classification scheme of the American College of Chest Physicians.
Introduction
Canyoning (referred to as “canyoneering” in Australia, New Zealand, and the United States) is a recreational activity involving travel through a narrow valley or gorge with steep sides or cliffs. Canyoning requires the use of a variety of techniques and technical skills, including jumps, slides, and walking or scrambling on wet surfaces, rappelling down waterfalls, swimming through cold pools and swiftwater, and employing advanced rope work. 1 Development of specialized equipment and techniques has facilitated commercial operations and exploration of increasingly more difficult canyons. Park officials in the United States and Australia, as well as canyoning associations in Europe, have reported increases in usage in the most popular areas over the past 2 decades.2,3 The associated increase in rescues accounts for 15 to 40% search and rescue (SAR) missions/cost in specific geographic locations.3,4 SAR operations in canyons are frequently necessary when companion rescue fails and often require special considerations because of remoteness, difficult terrain (Figure 1), and limited communication. 1 Specially trained and equipped SAR teams have been established, but there is no international consensus pertaining to minimum requirement levels of medical training and technical training for canyoning rescue. The International Commission for Mountain Emergency Medicine (ICAR MEDCOM) has published recommendations for canyoning rescue for professional guides and for equipment to be used by canyoning rescue doctors. 5 These recommendations, published in 2001, were based on consensus opinions of experts. The goal of the current review is to provide further updated guidance to healthcare providers and canyoning rescue professionals about best practices for rescue and medical treatment through the evaluation of the existing best evidence related to the potential canyoning incidents.
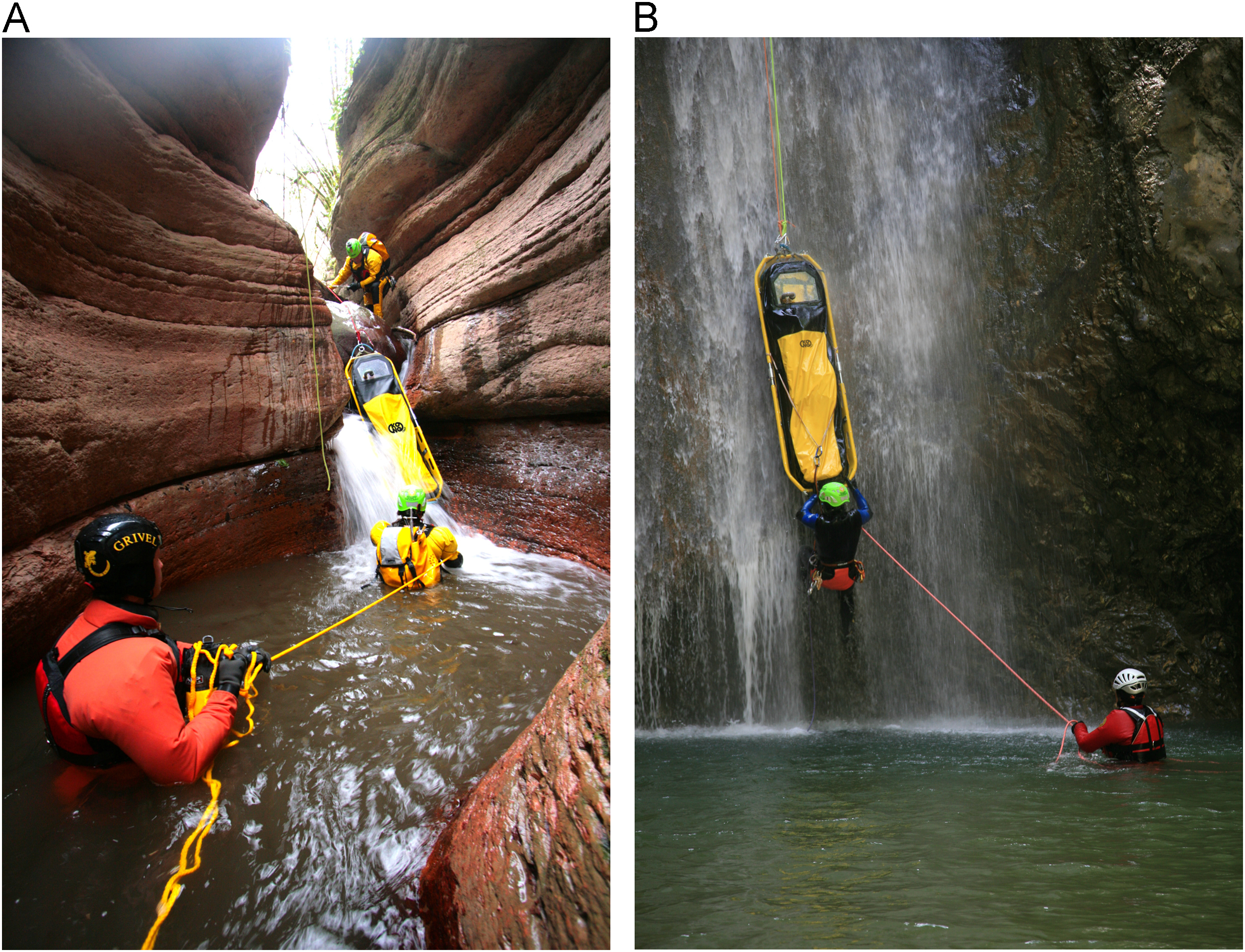
Transport of a stretcher by a canyoning SAR team. A, Floating transport in a water-filled passage during canyon SAR operation. B, High-angle terrain in a wet canyon. (Courtesy of Michael Kammerer. Available at:
Methods
The ICAR MEDCOM convened an expert panel to develop evidence-based recommendations for on-site management and transport of patients in canyoning incidents. Experts were selected on the basis of clinical or research experience with canyoning rescue. The panel agreed not to use a PICO (patient/problem, intervention, comparison, outcome) question strategy for the evaluation process, but generated a set of topics (Table 1) to define the most significant areas of interest. The authors performed an extensive literature search using electronic databases and manual searches. The Medline database was searched for articles using PubMed. No language restrictions were applied. We used the following search strategy: (canyoning [MeSH Terms] OR canyoning [All Fields] OR canyoneering [All Fields] OR barranquismo [All Fields] OR torrentismo [All Fields]). We included studies of canyoning activities that reported data on the epidemiology of canyoning, plus on-site management and transport of patients in canyoning incidents. Peer reviewed articles and abstracts as well as medical theses were considered eligible for inclusion. The authors independently screened the titles of all articles and abstracts identified by the search. Following screening, authors manually reviewed the materials to determine which were suitable for inclusion. The authors also reviewed the reference lists of the articles retrieved by the electronic searches to find other relevant reports not indexed in the electronic databases. Subsequently, the selected panel of experts graded each recommendation on the basis of quality of supporting evidence according to American College of Chest Physicians classification scheme (Table 2). 6 Where necessary, peer reviewed, randomized controlled trials, observational studies, case series, and case reports related to on-site management of specific topics were further used to grade recommendations, or to support expert consensus. Conclusions of review articles and non-peer–reviewed articles or book chapters were only used to provide background information; they were not used for grading recommendations. For those topics of interest where no best evidence was evident, the panel made recommendations based on expert consensus. The recommendations were further examined and consensus was reached at a manuscript meeting in Borovets, Bulgaria, in October 2016.
Set of topics related to on-site management and transport of patients in canyoning incidents
SAR, search and rescue.
American College of Chest Physicians classification scheme for grading evidence and recommendations in clinical guidelines
RCT, randomized controlled trial.
Source: Guyatt et al 6
Findings and recommendations
From a total of 32 citations that were received, 12 peer reviewed articles, 6 peer reviewed abstracts, 6 medical theses, and 1 epidemiological report were found to be relevant and were subjected to full review (Table 3). 2 –4,7–28 Ten additional relevant reports related to on-site management of canyoning-specific topics were added to the references because they were used to grade recommendations.
ICAR MEDCOM consensus guidelines for on-site management and transport of patients in canyoning incidents—grading articles
DGGN, Base du Secours en Montagne de la Gendarmerie Nationale; SAR, search and rescue; SNOSM, Système National d’Observation de la Sécurité en Montagne.
Epidemiology of canyoning incidents
Injuries are the most common complaint in canyoning SAR (81%), followed by medical and environmental illnesses (9%). 8 In the remaining rescues, the subjects had no injury or illness (10%). 8 Data are consistent among epidemiological studies from different geographic locations. 4 ,24,25,28 Medical and environmental illnesses are reportedly less frequent than injuries, but are often considered more severe when based on evaluation by the emergency physician of the mechanism of injury and the clinical parameters with the National Advisory Committee for Aeronautics score in a retrospective observational study.8,29 In particular, fractures and sprains of the lower extremities and injuries of the spine and chest are the most common injuries, closely followed by dislocations, mostly of the upper extremities. 8 Environmental illnesses for consideration include accidental hypothermia, drowning, heat-related illnesses, and illnesses related to contact with water, plants, and animals. Some medical conditions are also related to the intensity and duration of exercise, such as heat-related illness, exhaustion, and acute coronary syndrome.2,18 Regional variations in incidence, injury patterns, and environmental illnesses are evident due to differences in environmental factors (eg, dry vs wet canyons), the typical rescue included in various samples (companion rescue or organized SAR operations), plus the differential development of expertise, equipment, and techniques over time. 2 ,8,20,26 Fatalities occurred in 3–10% of patients in studies of the epidemiology of canyoning rescue operations. 8 ,16,23,28 Drowning and trauma were the main causes of fatalities.4,8
Epidemiology of canyon SAR operations
The proportion of SAR operations that take place in canyons is related to the popularity of canyoning in a given region. Canyon operations account for up 50% of SAR missions in Zion National Park, United States.4,13 SAR operations have seasonal peaks that reflect temporal patterns of recreation. These peaks are usually in spring and summer seasons. 1 ,8,26 In most areas, the mean time from an incident until admission to an acute care facility, or evacuation of uninjured patients, is longer than 1 hour, mainly due to delays in emergency calls and long response and scene times. 8 ,24,25,27 The majority of SAR operations (up to 63% in Spain), require the rescuers to have technical skills and the ability to operate in difficult terrain. 8 ,23,25 The frequency of helicopter support, complete with technical maneuvers such as winch or long line operations, depends on the time of data collection and area of investigation (ranging from 10–90%). 8 ,10,15,26
Risk assessment
Risk assessment in canyon SAR is essential. Multiple factors inform risk assessment during SAR operations in mountainous or remote environments; typically the level of risk is dependent on a combination of incident location, weather, patient condition, available human and material resource, communication challenges, 30 as well as the risk imposed by water. Providers of medical care operating in canyon SAR operations should be specifically familiar with the effects of water hydraulics and principles of swiftwater rescue.1,31 SAR operations often take place during adverse weather conditions, where rising water levels can become increasingly hazardous both for patients and SAR operatives alike. Therefore, before initiating a ground SAR operation that involves entering a canyon, the water flow and the canyon environment, especially in the narrowest sections, should be closely evaluated and where possible water contact should be kept to the minimum during all canyon SAR operations.25,32 Weather conditions should be monitored before and during the rescue to minimize the risk of being caught by a flash flood. Plus, a careful evaluation of the risk of falling debris is also crucial. Becoming stuck in flowing water can rapidly cause drowning. Knowledge of immediate rope release methods and specific pickoff strategies are crucial in this scenario. 1 Moreover, training in canyon SAR should emphasize the benefits of integrating leadership, team decisions, risk reduction methods, and optimal methods of communication in order to best prepare operatives for efficient operation in this particularly hazardous environment.33,34
Drowning
Drowning is a process resulting in primary respiratory impairment from submersion or immersion in a liquid medium. 35 Drowning incidents in canyons are often different than those in other bodies of water. Drownings in canyoning occur primarily due to mistakes, such as entering a hydraulic, or entrapment by undercut rocks or strainers while swimming or rappelling, and occasionally by being caught in flash floods.1,25 High impact injuries associated with drowning are more common than in sea rescue in the canyon environment.8,36
Rescue
If a canyoner is trapped in a hydraulic, the first priority for a rescuer entering the water is personal safety, followed by interrupting the drowning process as rapidly as possible. Drowning interruption can be facilitated by providing flotation or immediate removal from water.35,37 If a drowned person did not fall from a height or a waterslide, the likelihood of spinal injury is low.38,39
Recommendation
When rescuing a patient trapped in water, the first priority is to interrupt the drowning process by providing flotation or removal of the patient from the water, following international guidelines such as the European Resuscitation Council guidelines (expert consensus).
Resuscitation
Cardiopulmonary resuscitation (CPR) is rarely performed by rescue teams in canyoning incidents.8,21 Long rescue response times in canyon SAR operations 8 lead to very low rates of survival for patients submerged in water.35,40 Duration of submersion longer than 25 minutes is correlated with a very low chance of a favorable outcome. 41 Cold water temperature does not seem to be a predictive factor for survival. 35 In-water ventilator assistance is unlikely to be effective in canyon SAR, especially if the patient is pulseless. The patient should be removed from the water after a drowning incident, since there are usually safe places to provide effective CPR close to swiftwater in canyons. 1 After drowning, the duration of hypoxia is the most critical factor in determining outcome. Once a patient is out of the water, immediate rescue ventilation and early chest compressions, with defibrillation when indicated, result in better outcome if the patient is in cardiac or respiratory arrest.35,42
Recommendation
Restore oxygenation, ventilation, and perfusion as rapidly as possible according to the current recommendations of guidelines such as European Resuscitation Council guidelines (expert consensus). Removal from the water is preferred to in-water ventilation in canyon SAR, especially if the patient is pulseless (expert consensus). An automated external defibrillator should be used during resuscitation of a drowning patient. Use of an automated external defibrillator is not contraindicated in a wet environment (1A).
Advanced airway management
Prehospital airway protection with endotracheal intubation is possible with high success and low complication rate in helicopter-staffed emergency medical mountain rescue. 43 However, advanced airway management is rarely performed in canyoning rescue.8,26 The choice of advanced airway management in canyoning SAR is limited by long evacuation times, transport in difficult terrain, and by the availability of oxygen, monitoring devices, and continuous positive airway pressure. 44
Recommendation
Advanced airway management should be adapted to logistical and environmental factors in canyoning SAR (1C).
Trauma
Lower extremity and spinal injuries are common in canyoning incidents, 4 ,8,24,25,28 but life-threatening injuries (as evaluated by the emergency physician with National Advisory Committee for Aeronautics scores of 4–6) 29 were found in less than 4% of injured patients in canyoning incidents. 8
On-Site management
Assessment and management of patients in canyoning incidents are based on standard principles of trauma care. 45 Steep or rough terrain can make primary and secondary surveys difficult. If the scene is safe for the SAR team, they should move the patient to a suitable place for a primary survey. Suspected cervical spine injuries can be managed based on validated guidelines, such as National Emergency X-Radiography Utilization Study 46 or the Canadian C-Spine Rules, 47 or alternatively based on proposed guidelines such as the Wilderness Medical Society practice guidelines for spine immobilization in the austere environment. 48 In the past, spinal immobilization was recommended for all mountain rescue casualties injured in a fall. 49 When no appropriate commercial device is available, such as Kendrick Extrication Device (Ferno-Washington, Wilmington, OH), it is also possible to use layered ropes and canyoneering packs for improvised spinal stabilization. 1 However, where a time-critical injury or unsafe environment takes priority, spinal immobilization should not be performed before evacuation. 49
Recommendation
Canyon SAR should include trauma care in austere environments. Suspected injuries should be managed according to the specific recommendations of validated guidelines, adapted to injuries typical of canyoning incidents and conditions, especially long rescue time and environmental exposure (1C).
Examination of a patient wearing a wetsuit
Physical examination is difficult in a wet canyon if the patient is wearing a wetsuit, but the assessment should be as thorough as possible and prevent wasted time to avoid hypothermia. The best method is to not to remove the suit but to unzip it temporarily. If necessary, a longitudinal cut in the wetsuit can provide access for examination or interventions such as hemorrhage control. The cut can be closed later with bandages or duct tape, to limit the amount of heat loss. 1
Recommendation
The primary and secondary surveys should be done without removing the neoprene suit. If it is necessary to examine the patient, open the suit or make a simple longitudinal cut (expert consensus).
Management of fractures and dislocations
Splinting and immobilization were the most common on-site medical interventions in canyon SAR operations in Spain (71%) and France. 8 ,23,24 Before evacuating a patient, if there is risk of water contact during evacuation, water-resistant splints should be placed (eg, neoprene bandages, PVS First Aid, Milano, Italy). Alternatively, standard splints and bandages can be covered with plastic wrap and duct tape. Reduction of a dislocation dramatically relieves pain and reduces the risk of vascular and neurologic compromise. 50 Therefore, despite concerns about safety, reduction should be considered viable at the scene if trained providers of medical care are present. Less than 1% of patients 20 to 30 years old with a shoulder dislocation also have a fracture. 51 Risk can be further mitigated by evaluating clinical factors that predict the presence of a fracture. 52 Reduction of dislocations, especially of the shoulder and ankle, were completed in 7% of patients in canyon SAR operations in Spain. 8 The ideal technique would be simple, easy for a single provider to perform, rapid, atraumatic, relatively painless, and would not require any medication. After reduction, the patient should be reassessed for comfort, distal circulation, sensation, and motor function in the affected extremity.
Recommendation
Rescuers should train regularly to perform splinting and stabilization using suitable equipment for a wet canyon environment (1C). Providers of medical care operating in canyon SAR should have specific skills to reduce dislocations in austere environments (1C).
Fluids and drug administration
In one study, vascular access was obtained in 6% of patients and was followed by fluid administration in most cases. 8 Analgesia was the second most common on-site medical intervention in canyon SAR operations in Spain (34%). 8 Routes other than intravenous access (eg, intramuscular, intraosseous, oral, subcutaneous, and transmucosal) can be considered, but long rescue times (over 24 h) 53 and water contact are potential limiting factors. 23 If intraosseous access is chosen in a critical care situation, it should be replaced by intravenous access as soon as possible. A practical method is to give fluids and analgesia in boluses before evacuating the patient via winch operation or by moving the stretcher in a manner described as technical maneuvers/confined spaces. 54
Recommendation
Routes of fluid and drug administration other than intravenous should be considered in canyon SAR operations, based on patient status and logistical challenges (1C).
Wounds and infections
Wound care serves to remove contaminants, debris, and dirt and to prevent infection, even with minor scratches and abrasions. 55 High pressure irrigation using sterile or potable water should be performed at approximately 40–80 kPa (6–12 psi) with compressible fluid bags and syringe-based systems. 56 This will likely lower wound infection rates, especially in the case of open fractures, unless there is profuse bleeding. 56 –60 Zoonoses, such as leptospirosis, have been reported after canyon activities, even in European areas. 7 ,9,14 Despite recommendations that systemic antibiotic prophylaxis should be administered only for open fractures, 59 wounds in poorly vascularized areas (ie, hand, foot, lower and upper limb) are at high risk of infection in canyon environments. Therefore, it might be prudent to administer prophylactic antibiotics in selected cases of patients with severe wounds, risk of zoonoses, and long duration rescue times. 61 If there is a risk of contact with water, all bandages should be made waterproof (eg, with plastic wrap and duct tape). No commercial devices are available at this time. 1 Comfort, distal circulation, sensation, and motor function in affected extremities should be periodically reassessed.
Recommendation
Wounds should be irrigated to decrease infection rates (1A). Systemic antibiotic prophylaxis should be administered for open fractures (1A) and is reasonable in severe wounds (expert consensus).
Accidental hypothermia
Accidental hypothermia (core temperature <35°C) is a risk in canyons regardless of season and ambient air temperature. Heat loss in water is reportedly 25 times more rapid than in air. 62 The rate of heat loss is also increased on exposure to combined environmental factors, such as low ambient temperature, water, and wind, especially in exhausted or immobilized patients.63,64 The risk of immersion hypothermia is present in water colder than 25°C and is more severe in water colder than 15°C. 65 Patients cannot usually recognize symptoms of hypothermia in themselves, making it a priority for SAR operatives to diagnose and manage appropriately. Mild hypothermia has been reported in up to 11% of the victims in canyon SAR operations. 24
Circumrescue collapse
Hypothermic canyoners may collapse and die suddenly from hypotension or lethal dysrhythmias on removal from water 63 or as a result of having to perform work to assist in rescue, for example, by having to climb out of a pool,63,66 Mechanical stimulation has been shown to produce lethal arrhythmias in a porcine model of hypothermia. 67 The threshold for ventricular fibrillation is reduced significantly at a core temperature of 28°C. 68 Ventricular fibrillation due to hypothermia can also occur at higher core temperatures. The upper limit of core temperature at which there is a risk of ventricular fibrillation is not known. No case of rescue collapse caused by life threatening hypotension has been reported in canyoning, but data are limited.
Recommendation
A patient with suspected moderate to severe hypothermia (core temperature <32°C) should be handled gently, avoiding rough movement (1B), and kept horizontal if possible (1B), especially during rescue from water.
Insulation
An experimental study in conditions similar to a narrow section at the bottom of a canyon (ambient temperature of 5°C; wind speed of 3 m·s−1), found that mean skin temperature in healthy subjects wearing wet clothing increased with the addition of a vapor barrier under an ordinary ambulance blanket. 69 A vapor barrier can easily be fashioned from a garbage bag and is effective even if the patient is still wearing wet clothing. 1 ,69,70 Cold exposure can be reduced by insulating the body from the ground and by minimizing heat loss, including heat loss from the head. Field methods of external rewarming, such as the Norwegian charcoal-burning HeatPac (Normeca, Loerenskog, Norway) or large chemical heat pads are useful in both shivering and nonshivering patients.71,72
Recommendation
An injured or ill canyoner should be protected against further heat loss with dry, low-conductivity, whole-body insulation covered by a vapor barrier outer shell (1B). Rewarming devices should be used in conjunction with vapor barriers and insulation (1C).
Resuscitation
Guidelines for resuscitation of hypothermic patients differ from guidelines for resuscitation of patients who are not hypothermic. 35 In a hypothermic patient, the absence of signs of life is unreliable for declaring death. In the prehospital setting, resuscitation should be withheld only if cardiac arrest is known to have occurred before hypothermia or is clearly attributable to obvious fatal injuries, such as decapitation, open head injury with loss of brain matter, truncal transection, or if there is obvious decomposition. 73 Before starting CPR, an attempt should be made to find a carotid pulse for 1 minute, while also checking for respirations. Cardiac rhythm should be assessed if a cardiac monitor is available. 35 In a hypothermic patient CPR should be started as soon as cardiac arrest is diagnosed, or if there is any doubt, and continued until there is return of spontaneous circulation, or if there is clear evidence that attempted resuscitation is futile. 35 CPR should be delayed only if the scene is unsafe. Mechanical chest compression devices can facilitate prolonged CPR, but their use may be limited by contact with water. In a severely hypothermic patient CPR can be performed intermittently throughout the evacuation in difficult terrain where maintaining CPR may be hazardous or impossible. 74 Management with advanced life support may be limited by long evacuation times, transport over difficult terrain, and the availability of monitoring devices.
Recommendation
In canyoning SAR, treatment of hypothermia should follow the Wilderness Medical Society practice guidelines for out-of-hospital evaluation and treatment for accidental hypothermia or the European Resuscitation Council guidelines (expert consensus).
Heat-related illnesses
Increased body temperatures and heat-related illnesses have been reported in canyoning as the main medical or environmental reason for a SAR operation. 2 ,8,18,24 There can be a net heat gain through convection and radiation due to external heat exposure (high environmental temperatures), dehydration, and increased internal heat production due to prolonged and strenuous exertion, plus impairment of heat dissipation by evaporative cooling. 75 –77 Evaporative cooling can be limited by clothing, or by a wetsuit or drysuit, especially when there are alternating wet and dry sections in a canyon. 1 The overall mortality of heat stroke in various settings is 10–50%, 78 but no data for canyoning are currently available. When prevention via heat acclimatization, adequate fluid intake,79,80 and advanced planning of activities for cooler times of the day is not successful, optimal field management of heat-related illness becomes constrained. Factors such as the available human and equipment resource, contingency plan, canyon topography, whether the canyon is wet or dry, and whether pools are present become integral in the management of heat stress. The wetsuit or drysuit should be removed as soon as possible. Ideally, a patient should be cooled by whole body cold water immersion. Alternatively, evaporative and convective cooling can be done by spraying or dousing the victim with water while facilitating convection with air movement by fanning.75,81
General measures
Canyoning safety
Safety of the rescuers is the first priority during rescue. Evaluation of scene safety and potential hazards is mandatory. In some areas up to 90% of interventions are done with the use of helicopters, usually in conjunction with rope or ground rescue operations.8,23 Suitable equipment and knowledge of progression techniques are essential for safety of the rescuers. 1 ,3,82 Suitable harnesses, helmets, and canyoning-specific equipment help to avoid injuries. Specially designed canyoning shoes may reduce the risk of fall hazard, as well as the occurrence of foot injuries. 17 Progression with the use of a rope requires releasable rappels and special descenders in wet canyons. In wet canyons, rappelling is commonly done on a single strand of rope without a secondary conditional self-belay to prevent being trapped under a waterfall.1,82 To avoid getting trapped in a hydraulic at the base of a waterfall or slide a final knot should not be used and ropes should be kept above the water.1,82 Rescuers are at risk of zoonoses, such as leptospirosis. 7 ,9,14 In France vaccination is recommended for water sport professionals who are at risk of being exposed to leptospirosis. 83
Recommendation
Ground and air rescuers operating in canyoning SAR should have specific personal gear and equipment for progression (1B). They should undergo specific training, including the use of single-rope technique without a self-belay (1C) and consider specific zoonosis prevention (1C).
Transport
The evacuation and transport of victims in canyoning rescue are strongly influenced by environmental and logistical factors (Figure 1), mainly narrow and vertical passages, exposure to water in waterfalls and swiftwater, and the difficulty of evacuating patients by helicopter (including by winch operation and other technical maneuvers). 1 ,8,23,28 In France, the mean time from the incident to evacuation (or to admission to a healthcare facility) was 170 min (range 35 min to 19 hours). 25 A special harness that incorporates both a patient harness and an extrication device can be used for hoist evacuations. 84 Stretchers for canyoning SAR have been developed with special features, including buoyancy, the ability to keep victims out of the water, protection of the victim from impact, suitability for sliding and rope transport, and the possibility to monitor the patient. 1 ,19,54
Medical equipment
Most canyoners carry a basic first aid kit. 2 ,3,22 In canyoning SAR, medical equipment can rarely be brought directly to the site of the incident by helicopter, but requires ground transport, including water transport. 1 ,8,25 Water damage is the main risk for medical equipment and materials. Medical kit bags generally have modules for airway management and ventilation, circulation with hemorrhage control, analgesia and medication, splinting and immobilization, and insulation material. 1 ,22,23,85
Organized rescue
Protocols for canyon SAR operations should be integrated into wilderness and search and rescue emergency medical service protocols. France implemented specific training protocols beginning in the 1990s. 25 In the United States, the National Park Service provides canyon SAR operations. 1 ,11,12 In most SAR operations medical interventions are provided on site by physicians, paramedics, or other rescue personnel. 1 ,8,23,25
Conclusions
Canyoning has become one of the fastest-growing wilderness recreational activities. The associated increase in rescues has motivated the development of the current recommendations for management of canyoning incidents, graded on the basis of quality of supporting evidence. Data regarding on-site management and transport of patients in canyoning incidents are still limited. It is difficult to conduct randomized, controlled trials, plus it remains challenging to simulate canyoning incidents. Future research should be directed towards evaluating the efficacy of medical interventions and SAR operations in the canyon environment, specifically focused on the unique combination of challenging parameters encountered (ie, remoteness, water exposure, limited on-site patient management options, and technically challenging terrain).
Footnotes
Acknowledgements
Acknowledgments: The authors thank ICAR MEDCOM members (
Author Contributions: Study concept and design (GS); drafting of the manuscript (GS, OR, FA, KZ, IS); critical revision of the manuscript (GS, OR, FA, KZ, GZR, LLG, IS); and approval of final manuscript (GS, OR, FA, KZ, GZR, LLG, IS).
Financial/Material Support: None.
Disclosures: None.