
Abstract
Skeletal tuberculosis, otherwise known as Pott’s disease, has been recognized for centuries. Although typically diagnosed in citizens from countries with endemic tuberculosis, long-term workers in these regions, such as military deployees, can also acquire the disease. We present a case report of a military veteran presenting with neck pain and initially diagnosed with cervical disc disease. The patient’s pain progressed to the point of developing paresthesias in his bilateral upper extremities. Eventually, cervical spine radiographs were obtained that revealed complete cervical vertebral body destruction from spinal tuberculosis. Epidemiology, diagnosis, and treatment of the disorder are discussed.
Introduction
Spinal tuberculosis is a form of skeletal tuberculosis and most commonly affects the lower thoracic or upper lumbar region of the spine. Spinal tuberculosis is an increasingly common manifestation of extrapulmonary tuberculosis, now accounting for nearly half of all cases of musculoskeletal tuberculosis. 1 Named after the British surgeon Percival Pott, the classic manifestations of the disease—destruction of the disk space and vertebral bodies and progressive kyphosis—eventually came to be known as Pott’s disease. It is one of the oldest diseases known to man and has been traced back to Egyptian mummies from the 4th century BC. 1
The exact incidence and prevalence of Pott’s disease are not known due to inconsistent reporting. Of those patients affected by skeletal forms of extrapulmonary tuberculosis, the spine is the most commonly affected site, followed by the hip and knee. 1 Recognition and diagnosis of the disease is important because it commonly affects young adults in their most productive working years. There have been case reports of multidrug resistant spinal tuberculosis, although it is fortunately not yet common. Within the developed world, Pott’s disease is still relatively uncommon and is usually diagnosed in those who have immigrated from, or have spent considerable time in, endemic countries. 2
Traditionally considered a “disease of poverty,” the risk of developing spinal tuberculosis has increased since the advent of the HIV era, with over 90% of all new tuberculosis cases concentrated in sub-Saharan African and Southeast Asia. 3 Despite the increasing prevalence of Pott’s disease, delays in diagnosis are frequent due to missed diagnosis. This is unfortunate because early diagnosis and treatment are crucial in preventing long-term morbidity, deformity, and disability from the disease. 3
Case Report
Our patient was a 36-year-old African-American male military veteran in good health until November 2015, when he woke suddenly one morning with a sharp pain in his neck. He initially attributed the pain to poor posture while sleeping and took over-the-counter analgesics for pain relief. However, over the next several days his pain did not resolve, and he presented to his local Veterans Affairs medical center. Neck radiographs were performed and reportedly revealed only degenerative cervical disease. The patient was advised to use nonsteroidal anti-inflammatory medications and muscle relaxers and to return if his pain did not remit.
He continued to have neck pain and returned to the Veterans Affairs medical center on several more occasions. He was eventually referred for physical therapy. His pain continued despite these treatments, and he gradually began to develop neck stiffness that was diagnosed as muscle spasm. In the following days, the patient’s pain began to spread to his shoulders and upper extremities with a concomitant sensation of cold in his upper extremities and paresthesias bilaterally in his fingers in a “stocking-glove” distribution.
With the onset of these new symptoms, the patient presented to a local urgent care center. By this point, the patient was describing the sensation of an inability to flex or extend his neck with the unusual complaint that he felt like his head might “fall off.” Cervical radiographs were repeated at this visit and revealed complete collapse of his C6 vertebra (Figure 1). He was placed in a cervical collar for neurologic protection and transferred to the emergency department at our local hospital. In the emergency department, magnetic resonance imaging revealed near-complete destruction of the C6 vertebral body with anterior and posterior extrusion of the C6 remnants as well as dural thickening and enhancement of the spinal cord centered at the C6 level with subsequent spinal cord compression (Figure 2).

Cervical radiographs revealing complete compression of the C6 vertebral body with C5 vertebral posterior tilting and impingement upon the spinal canal.
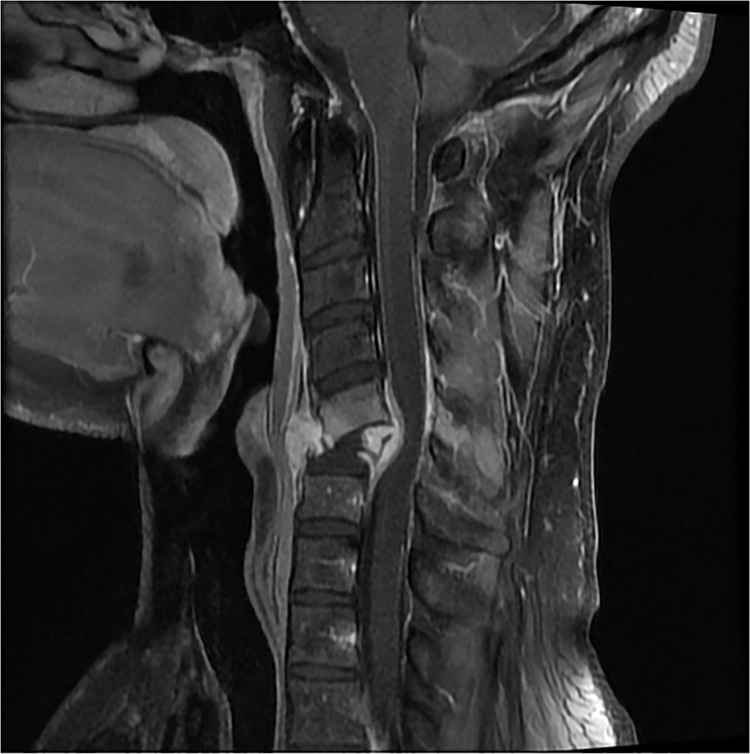
Cervical MRI revealing destruction of the C6 vertebral body with extrusion of the remnants both anteriorly and posteriorly and C6 level spinal cord compression.
The patient was immediately admitted and underwent emergent anterior cervical corpectomies of C5 and C6 with subsequent fusion of the vertebrae. Specimens of bone were collected and sent for culture and pathology. The initial surgical specimens revealed chronic lymphohistiocytic inflammation with giant cells and granuloma formation, suggestive of mycobacterial tubercular infection. Further testing with QuantiFERON gold assay returned positive while the patient was still admitted, and the positive assay plus typical pathologic findings resulted in the patient being diagnosed with suspected tuberculosis of the spine. He was started on a 4-drug therapeutic regimen consisting of isoniazid, rifampin, pyrazinamide, and ethambutol along with vitamin B6. Because of his continued improvement, he was discharged home on this regimen and followed up with an infectious disease specialist. A purified protein derivative test resulted as positive at 17 mm of induration. Roughly 6 weeks after his hospital admission, the patient’s skeletal acid-fast bacilli (AFB) culture grew mycobacterium tuberculosis resistant only to isoniazid. This confirmed the diagnosis of Pott’s disease, and he was continued on 4-drug therapy, with moxifloxacin as an alternative to the initial isoniazid. Several weeks after starting the 4-drug therapy, the patient reported right upper quadrant pain and rash and was found to have an elevation of his liver enzymes. His medications were held until his liver enzymes returned to normal, and he was restarted on ethambutol, rifampin, and moxifloxicin to complete a total of 39 weeks of therapy.
Discussion
Our patient was a middle-aged man who had performed multiple tours of military duty in the Middle East and had had several normal purified protein derivatives before his diagnosis of Pott’s disease. He had reported several months of ongoing neck pain that progressed to include bilateral upper extremity paresthesias. Initial imaging revealed the complete destruction of his C6 vertebral body. Before obtaining the radiographic images, the patient was assumed to have degenerative disease of the cervical spine, a not uncommon cause of neck pain, despite his relatively young age. The differential diagnosis at this point should also include facet joint disease and spondyloarthropathy; other causes of vertebral body collapse are severe osteopenia/osteoporosis, pyogenic spinal infection, and malignancy. 1 The working diagnosis of spinal tuberculosis was not made until we received the results of positive QuantiFERON gold screening performed based on his travel history as well as pathologic analysis of his surgical specimens. The definitive diagnosis was not made until his AFB cultures returned positive.
Although less common in developed countries, recent immigrants to the United States as well as those who travel to, and spend prolonged time in, endemic regions can be at risk for contracting both pulmonary and extrapulmonary tuberculosis. Tuberculosis remains the most common HIV-opportunistic infection worldwide and often presents as extrapulmonary tuberculosis. 1 As with our patient, the majority of those with Pott’s disease present with pain localized to a specific region of the back, muscle spasm, and prominent spinal deformity. 1 The classic form of the disease is destruction of the intervertebral disk space and adjacent vertebral bodies, with the development of often severe and progressive kyphosis. Occasionally, the infection can spread contiguously to adjacent ligaments and the soft tissue surrounding the spine, forming a so-called “cold abscess,” or palpable soft tissue swelling, at the level of infection. Another typical feature of Pott’s disease is known as a “Gibbus formation,” or a structural kyphosis whereby one or more adjacent vertebrae become wedged together. This wedging can lead to cord compression and resultant paraplegia. Those with later sequelae of the disease may also present with more generalized neurological deficits distal to the site of the lesion.
Pott’s disease usually results from hematogenous seeding of tubercular bacilli from another primary site, typically the lungs. Progression of Pott’s disease is slow and indolent, with average duration ranging from months to years. 1 In thoracic disease, spinal kyphosis is considered “the rule rather than the exception,” 3 with occasionally severe kyphosis of >60 degrees angulation forming. Pott’s disease usually affects the lower thoracic and upper lumbar spine, and less commonly the cervical spine.
The diagnosis of Pott’s disease can be made clinically, radiologically, or with microscopy and culture, depending on the region in which the patient presents. In endemic regions in which advanced microscopic diagnosis may not be readily available, diagnosis can be difficult because of the nonspecific features and subacute course of the disease. 3 Another challenge to diagnosis is that patients may have no concomitant evidence of active pulmonary disease. Constitutional symptoms typically associated with pulmonary tuberculosis, such as weight loss, night sweats, and fever, are less common in spinal tuberculosis. Clinicians should remain alert to other clinical clues, such as a history of travel to an endemic country, contact with a known tuberculosis contact, or history of an immunocompromised state.
The gold standard of skeletal diagnosis is culture and microscopy of biopsied skeletal tissue.2,4 AFB and histopathology are not capable of revealing the diagnosis in all cases; therefore, biopsied specimens should be subjected to culture and sensitivity as well as polymerase chain reaction when available. 3 Sensitivity of staining for AFB is highly variable, and culture requires a long incubation period of 4 to 6 weeks. 3 Fortunately for our patient, the AFB testing did indeed return as positive, confirming the diagnosis and allowing for continued treatment of his disease.
In 2010, the World Health Organization endorsed the Xpert MTB/RIF assay, an automated molecular assay for rapid diagnosis of tuberculosis and detection of rifampin resistance. 5 Essentially a point-of-care test, this assay provides results of testing within 2 h, allowing the patient to be started on the appropriate treatment the same day. 6 The World Health Organization now strongly recommends use of the Xpert MTB/RIF as the initial diagnostic test for those suspected of having multidrug resistant or HIV-associated tuberculosis. 5
Beyond culture and the Xpert MTB/RIF assay, other laboratory testing is often not useful in making the diagnosis. Commonly obtained laboratory testing may show relative leukocytosis with an elevated erythrocyte sedimentation rate, although this is nonspecific. A positive Mantoux, or purified protein derivative skin test, is also considered nondiagnostic in endemic regions owing to the prevalence of use of Bacillus Calmette-Guerin immunization. 2
In resource-poor nations, plain radiographs remain the cornerstone of spinal imaging and therefore diagnosis. 1 Cold abscesses are occasionally seen as soft tissue shadows adjacent to the spine. Computed tomography and magnetic resonance imaging (MRI) both allow for improved diagnosis of spinal tuberculosis. Computed tomography can better show vertebral lesions and paravertebral abscess, and MRI is better used to determine the spread to soft tissue and the degree of spinal cord involvement. 1 MRI can also at times detect tubercular lesions before they are evident on radiographs; it has a sensitivity nearing 100% and specificity of 88%. 3
Early diagnosis and treatment are necessary to minimize potential spinal deformity and prevent possible long-term sequelae of the disease.1,3 Antituberculosis treatment with standard 4-drug therapy should be started as soon as possible in patients with spinal tuberculosis. 1 At times, treatment may need to be started empirically, before the actual clinical diagnosis is reached, due to the risk of complications from the disease, specifically vertebral destruction. For patients with HIV infection, treatment of tuberculosis follows the same general course with antitubercular medications plus use of antiretroviral therapy. One must keep in mind, however, the potential interactions between many antiretroviral drugs and rifampin. 1
The majority of antitubercular drugs have good penetration into bone. 1 Obtaining serial radiographs is often not helpful in measuring response to treatment because the disease can appear to progress on imaging studies during treatment. 7 Therefore, treatment response should be gauged clinically by perceived pain relief, decrease of any apparent neurological deficits, and—at times—correction of spinal deformity. Three- or 4-drug medical therapy is generally sufficient to treat spinal tuberculosis, although there have been a few recent reports of multidrug-resistant spinal disease. 8
Patients with neurological deficits, potential or actual mechanical instability, and moderate to severe kyphosis require surgical intervention. 9 Surgery is also often indicated in infection of the craniovertebral junction (as in our patient) because this represents a potentially dangerous complication of the disease. Surgery should also be considered when a paravertebral (“cold”) abscess has not responded to 4 to 6 months of medical treatment. 9 Treatment options for craniovertebral junction spinal tuberculosis are controversial owing to the lack of well-established treatment guidelines. 10 Paraplegias with active disease can be secondary to mechanical pressure on the spinal cord, secondary to abscess formation or granulation tissue, or result from mechanical instability produced by subluxation or destruction of the vertebral body. 3 Occasionally, this form of tuberculosis has responded well simply to medical treatment, but surgery should still be carefully considered. 10
Author Contributions: Study concept and design (JW); drafting of the manuscript (JW, JS), critical revision of the manuscript (JW, JS); and approval of final manuscript (JW, JS).
Financial/Material Support: None.
Disclosures: None.