
Abstract
Exposure to leeches in the wilderness setting is common. Leeches may attach themselves to exposed skin or pass through one of the body’s orifices and attach internally. The condition of leech attachment is known as hirudiniasis, which can result in serious morbidity and, rarely, mortality. A comprehensive review of the literature was performed to detail the prevention of leech attachment, as well as both anecdotal and studied methods of removal. Complications from leech attachments include ongoing bleeding, wound infection, and poor wound healing. Although medicinal leeches are the most well-studied variety, this review examines all aspects of leech attachment, prevention, and management.
Keywords
Introduction
Leeches have been an object of both public fascination and repulsion and have been used medicinally for thousands of years. 1 Today, many outdoor recreationists and travelers encounter leeches and develop leech attachments. The consequences of these attachments range from inconvenient to severe complications, such as bleeding, infection, and even death. This present work seeks to review the prevention, removal, and wound care of hirudiniasis while exploring historic, folk, and contemporary remedies.
Background
Leeches are a subclass (Hirudinea) of segmented worms (phylum Annelida). Although there are over 600 species, only a minority of these are sanguinivores (ie, blood drinking) and the cause of human morbidity. 2 Hirudo are freshwater leeches that can range from very small to up to 10 cm long. They have 2 suckers, anterior and posterior, with 3 jaws on the anterior sucker. They can ingest almost 10 times their weight in blood (approximately 5–15 mL) in a single feeding, which typically takes place over 20 to 30 minutes. One feeding can satiate the leech for a year or more. 3 –5 Although most attachments are short and external, attachment to internal surfaces such as the eye, ear, nose, naso/oropharynx, urethra, bladder, rectum, or vagina, can last for days or weeks. 6 The medicinal leech, Hirudo medicinalis, is the most studied variety. Figure 1 provides a photograph of Hirudo medicinalis.

Hirudo medicinalis attached to a human hand. Photograph credit/rights: Shamleen/Shutterstock.
Leech attachments can cause significant bleeding secondary to biologically active anticoagulation factors intrinsic in their saliva. The most potent of these factors is hirudin. This molecule inhibits thrombin-catalyzed conversion of fibrinogen into fibrin clots 7 and remains active for 15 to 20 minutes.8,9 Figure 2 depicts the interruption of clotting components by hirudin. The mean duration of bleeding is approximately 10 hours, with an upper limit of 7 days.2,10 Although formal data do not appear to be available, authors have estimated the rate of blood loss at the wound to be 1 mL per minute (or 60 mL per hour). 11 Although leeches will detach themselves and fall off after they are full, bleeding at the site of the attachment may continue for hours due to the continued presence of anticoagulation factors at the wound site.
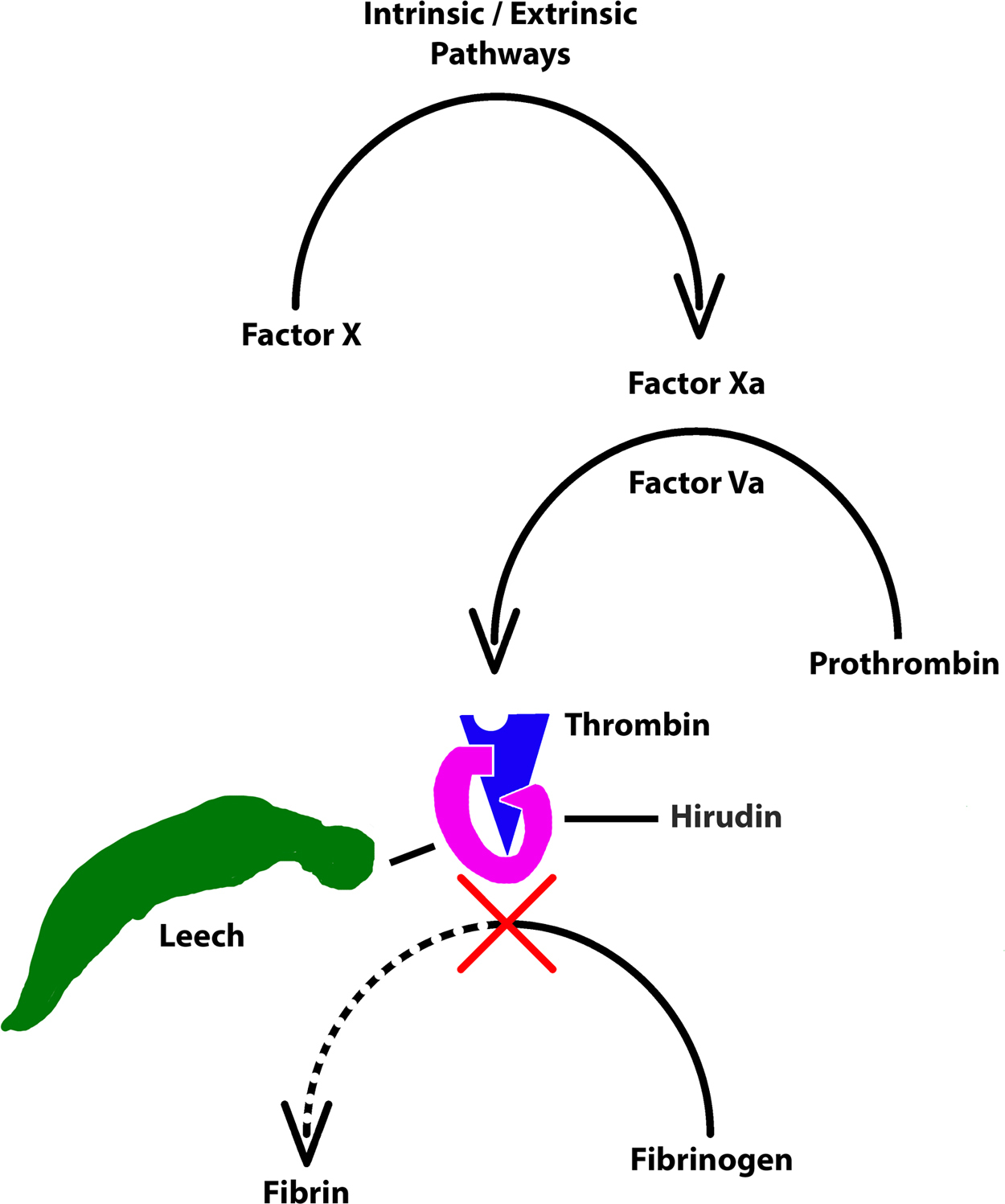
Coagulation interruption by hirudin found in leech saliva (adapted from Hildebrandt and Lemke 4 ).
Historic context
Leeches have been used throughout history for a variety of medicinal purposes. The earliest recorded use of leeches was in 1500 BCE, as depicted in an Egyptian tomb. 1 They were used to reduce inflammation, which was thought to be the source of all subsequent disease. 1
Leeches are mentioned both in the Bible and the Koran. 2 Europeans were so enamored with the use of medicinal leeches in the 17th and 18th centuries that they depleted the supply.1,12 Use of leeches then declined in the 19th century, coinciding with the rise of germ theory, but a renaissance in the use of medicinal leeches occurred in the 20th century in the field of reconstructive surgery.1,12 In 2004, the US Food and Drug Administration approved leeches for use in micro- and plastic surgery. 1 Outside of the hospital, contemporary folk remedies have involved the use of leeches to treat black eyes and varicose veins. 3
Prevention
Methods to avoid and prevent leech attachment are largely intuitive; the easiest and most effective way is to avoid leech-infested regions. Indeed, leeches can be encountered in more than aquatic environments. Some land species simply perch on vegetation awaiting the opportunity to attach to a host and obtain a blood meal. Other prevention methods that have been suggested, but remain mostly speculative, include wearing tall, light-colored socks pulled over pants13,14; inserting tobacco between the toes 15 ; placing dried, powdered Neem leaves under clothing 16 ; or applying body oil because leeches have a difficult time attaching to slippery surfaces. 16 Strategies borne from formal study include application of N,N-diethyl-meta-toluamide17,18 or N,N-diethyl phenylacetamide 17 as chemical repellents. Based on this literature, the authors’ recommendations are to wear clothing that covers the lower extremities (tucked, long socks) and to apply insect repellents such as N,N-diethyl-meta-toluamide or N,N-diethyl phenylacetamide.
Removal and incapitation
Signs and symptoms of attachment
Most leech attachments are external. General symptoms of a leech attachment include painless bleeding, bruising, itching, burning, swelling, pain, irritation, redness, irritant contact dermatitis, follicular pseudolymphoma, and mucosal synechiae. 2 ,13,19–24 A single discovered leech should prompt an investigation for other attached leeches. 2
Internal leech attachment can be indicated by symptoms such as bleeding from the associated orifice(s), obstruction of the associated orifice(s), or a sensation of foreign body movement. Voice alteration or hoarseness, cough, stridor, and dyspnea are present when the leech attachment is associated with the larynx. Gross painless hematuria and dysuria, fever, pallor, and vomiting can also be found with internal leech attachment. 3 ,13,19–22,25–32
Removal
Due to severe local alterations in coagulation associated with leech attachment, initial treatment should focus on removing the leech(es), controlling blood loss, and preventing exposure to blood-borne pathogens. 2 Other factors to consider include infection and morbidity from mechanical obstruction or internal hemorrhage. 33
The medical literature is full of anecdotal and individual recommendations for leech removal. Unfortunately, few data are available to compare methodologies. Table 1 lists removal strategies that have been previously described but which are not necessarily recommended due to their anecdotal nature. They are presented to the reader for historic perspective and as a demonstration of human ingenuity. The authors’ recommendation is to attempt incapacitation if it can be done without stimulating leech regurgitation, followed by a combination of gentle traction and using a fingernail or other flat object to break the suction of the attached mouthparts. Just as with hematophagous arthropods, we recommend caution when detaching the leech to avoid causing reflux of potentially pathogenic blood previously consumed by the leech. Simple saltwater solutions have been reported to be effective in providing sufficient stimulation to cause the leech to relax and release. 45
Historic removal strategies described in the medical literature
Table 2 describes potentially effective chemical means that have been used to kill or incapacitate a leech for removal. Due to unique complications and considerations of various leech attachment sites, much has been written describing either anecdotes or advice for dealing with attached leeches. Table 3 lists these anecdotal methods with their considerations for removal of leeches related to the body part to which the leech was attached.
Chemical means reported to kill or incapacitate leeches for removal
Methods reportedly used for leech removal or special considerations needed with removal
Bleeding and wound care
After removal of the leech, 2 primary concerns are achieving hemostasis and initiating wound care. Once an attached leech is removed, the area should be cleaned with water and soap, consistent with general wound care. Various cultural and regional approaches to pain and subsequent itching differ considerably, with some using plant extracts, soap flakes, and oils. 14 It is likely that ice and antihistamine medications can be used to help control pain, itching, and inflammation, although these have not been specifically studied. Betadine or other topical antibiotic agents can be used for local wound treatment.20,33 The authors recommend a simple approach to external wound care, including cleaning the wound, assisting with coagulation via bandage or hemostatic agent, and monitoring the wound for signs of infection. Figure 3 provides a photograph of a man’s foot bleeding after leech removal.

Bleeding foot after removal of leeches. Photograph credit/rights: Mykola Ivashchenko/Shutterstock.
Multiple leech attachments and feeding can lead to significant blood loss, resulting in hypochromic microcytic anemia. In these cases, a complete blood count can reveal decreased red blood cells, decreased hemoglobin and hematocrit, decreased mean corpuscular volume, normal white blood cells and platelets, and increased eosinophils. Most attachments will not affect gross coagulation pathways; therefore, laboratory findings will show normal international normalized ratio and partial thromboplastin time. If there are multiple leech attachments and/or underlying coagulation disorders, an individual can experience severe anemia and even death. 3 ,6,10,27 In a case described by Kose et al, a patient with 130 leech attachments experienced systemic effects causing altered prothrombin time and partial thromboplastin time laboratory studies requiring transfusion of plasma and red blood cells. 33
Hemostasis
Although several methods for achieving hemostasis have been proposed, evidence supporting a best method is still lacking. Some of these methods that we include for context and which may have anecdotal value only include insertion of a tampon for orifice bleeding, 10 application of a sponge or gauze soaked in thrombin solution, 2 ,3,33,35 electrocoagulation cauterization to the bleeding site, 2 ,55–57 styptic pencil use,2,3 vein ligation of affected vessels, 36 localized application of tranexamic acid,30,58 cryotherapy with silver nitrate, 33 and oxidized regenerated cellulose absorbable hemostat with hemostatic dressing. 2 Some recommend against the suturing of wounds2,54 and some advocate for the suturing of bleeding wounds. 59
To highlight the painless bleeding that can occur, Ikizceli et al describe the case of an individual who used leeches for personal homeopathic therapy at night and sustained significant bleeding masked by the darkness and unnoticed during sleep. 35 In rare, severe cases of bleeding, clotting factor replacement has been used and recommended. 2
Complications
Viruses, bacteria, and protozoa infectious to humans have been found to survive inside leech digestive tracts, and there have been documented cases of transmission of these infectious agents. 50 Because leeches may regurgitate previously ingested blood if removed by salting or mechanical force, 50 it is important for the wilderness medical provider to be knowledgeable of the risk of pathogen transmission.
Leeches may also regurgitate digestive material during feeding, whether from an accidental or medicinal attachment. Infections that have been reported after repeated medicinal leech use include syphilis, puerperal fevers, erysipelas, and Aeromonas hydrophila. 3 Researchers have isolated HIV and hepatitis B viruses from live leeches pulled from fishermen in Africa. Other viruses, such as hog cholera and myxoma, for example, have been shown to remain present in leeches for as long as 5 months. 60 The model Plasmodium species for studying malaria (P berghei) was found to not only survive in the gut of medicinal leeches, but to be able to reproduce by using red blood cells the leech had consumed. 50
Although outside the scope of acute wilderness practice, we can glean important lessons from medicinal leech use. For example, just as medicinal leeches are not perfectly safe, leeches in pristine wilderness may carry risk by virtue of their lack of endogenous digestive enzymes that would otherwise provide a host defense against colonization of common water-borne bacteria. 61
Medicinal leeches are often imported from outside countries with no information available regarding their origins or exposure. 50 It is therefore not surprising that an estimated 2.4 to 20% of leech therapy results in infection. 7 Leeches have been demonstrated to be potential vectors for Trypanosoma sp, Plasmodium sp, viruses, 3 and chromoblastomycosis. 62 In one study of 227 patients whose postsurgical flaps were treated with leeches, there was an infection rate of 14.4%. Of these, 87.9% were A hydrophila. 63 A hydrophila is typically successfully treated with fluoroquinolones, although multidrug resistant strains have emerged. 61 ,63,64 Leech storage via refrigeration does not kill potential human pathogens. 50
With increased home use of leeches, as well as US Food and Drug Administration–approved medicinal usage, medical providers prescribing leech therapy commonly prescribe concurrent prophylactic antibiotics, such as a fluoroquinolone, to prevent Aeromonas infection. 1 ,65,66 Other commonly used antibiotics include third-generation cephalosporins, trimethoprim/sulfamethoxazole, 7 ,24,33,52,58,59 amoxicillin, 39 ampisid, 33 metronidazole, 23 and lomefloxacin. 32 Although it has not been studied, nonbacterial infections are also possible, and because the preferred antibiotic choice of a fluoroquinolone comes with disadvantages such as potential tendinopathy, the authors do not recommend routine antibiotic prophylaxis after attachment. Other known side effects after leech attachments include scarring, 3 local allergic reaction and anaphylaxis, 3 ,13,67 and the development of complex wounds prone to dehiscence and slow healing. 35
Given the extrapolated practice patterns observed from medicinal leech use, it may be reasonable to offer antibiotics to risk-averse patients with leech attachments in a wilderness setting, even though no data document this necessity. For those patients who develop signs of infection, treatment with antibiotics would be reasonable given the aforementioned limitations and suggestions.
Conclusions
Hirudiniasis is a common condition experienced by both humans and animals with much information, speculation, and anecdotal recommendations given regarding its medical management. The approach to the management of leech attachments must draw from case reports and series; evidence-based recommendations are unfortunately lacking. Basic principles can be adapted from what we currently know; these include prevention by avoidance or with long clothing, incapacitation and removal without unnecessary trauma to the leech, wound care that addresses hemostasis and the resulting risk of complications, and consideration of antibiotic coverage against Aeromonas species when suspicious of infection.
Novel agents have been used to control hemostasis and may be amenable to use in austere environments, although data are insufficient to make formal recommendations. Novel agents include topical tranexamic acid and hemostatic gauze and bandages that directly affect the coagulation cascade to reverse anticoagulation. There is a paucity of literature on outcomes or best practices regarding wilderness leech attachment management, and this review should serve as a call for research on this common problem.
Acknowledgments: The authors thank Derek Cooney, MD, for illustrating the figure of coagulation interruption by hirudin found in leech saliva. They also acknowledge Susan Wojcik, PhD, and Christine Podolak, MS, for their assistance in manuscript preparation.
Author Contributions: Study concept and design (JJ); acquisition of the data (NZ); drafting of the manuscript (NZ, AB, KW); critical revision of the manuscript (JJ); and approval of the final manuscript (JJ, AB, KW, NZ).
Financial/Material Support: None
Disclosures: None