
Abstract
A 48-year-old man developed general fatigue, dyspnea, and fever at an altitude of 1562 m from the morning of the first day of a 3-day hike. Despite pharyngeal discomfort and mild general fatigue, he felt that the symptoms were not sufficient to abandon his plan. He usually required 1.5 hours to reach Tokusawa (6.4 km from the starting point at an altitude of 1500 m), but this time he required 2.5 hours and slept briefly upon arrival at Tokusawa due to extreme fatigue and respiratory discomfort. His symptoms became aggravated, so he presented at a mountain clinic with oxygen saturation at 80% and body temperature of 37.6°C. He was diagnosed with hypoxemia due to pneumonia and/or other disease(s) and was evacuated to a hospital where a chest computed tomography scan revealed ground glass opacity and infiltrative shadows. He was treated for pneumonia, but another doctor discovered during follow-up that the patient had sprayed 300 mL of a waterproofing aerosol on mountain equipment in a nonventilated, enclosed area of his home on the night before starting out on the hike. Therefore, waterproofing spray was considered to have caused pulmonary damage. Self-reporting or appropriate questionnaires are the only means of identifying this type of injury. The differential diagnosis of pulmonary problems in an outdoor setting should include toxic aerosol exposure from waterproofing spray.
Introduction
Protection against becoming wet is essential for safe and comfortable outdoor activities.1,2 Waterproofing or leather protector compounds containing fluoropolymers, silicone resins, petroleum hydrocarbons, or other solvents are sprayed onto surfaces to repel water and dirt. However, these products can cause acute lung injury when applied in poorly ventilated areas. 3 –5 The elapsed time to development of symptoms such as shortness of breath, chest tightness/pain, dry cough, throat pain, headache, nausea/vomiting, fever, lightheaded/dizziness, and general fatigue and fever varies from <15 minutes to 24 hours after inhaling an aerosol. 4 ,6–9 However, leisure activities in remote areas could proceed before symptoms of delayed onset appear or worsen.
We describe a patient presenting with pharyngeal discomfort, general fatigue, respiratory discomfort, and fever that developed while hiking at an altitude of 1562 m. He was initially diagnosed with hypoxemia due to pneumonia and/or other disease(s), but further information suggested that inhaling 300 mL of waterproofing spray caused the pulmonary damage.
Case Report
A 48-year-old Japanese man presented with pharyngeal discomfort, general fatigue, dyspnea, and fever at a mountain clinic located at an altitude of 1562 m in the Japanese Northern Alps on the first day of a 3-day hike.
He had felt pharyngeal discomfort and mild general fatigue from the morning of the day he left his Tokyo residence, which was essentially at sea level. He did not consider his consumption of 360 mL of Japanese sake on the previous evening to be a factor because he habitually consumed that amount. He felt that something was wrong, but the symptoms were not sufficient to abandon his plan to climb Mt. Yari (altitude 3180 m). He travelled with a friend by public transport to Kamikochi (altitude 1500 m), a starting point for the Japanese Northern Alps. He became unable to walk at normal speed soon after starting the hike. He usually walked faster than this friend, but he was slower than his friend on that day and needed 2.5 hours to reach Tokusawa (altitude 1562 m; distance 6.4 km from Kamikochi) instead of the usual 1.5 hours. After walking for about 1 hour, he found that he could not continue without brief stops due to worsening fatigue and respiratory discomfort. Therefore, they changed their destination for the first day to Tokusawa instead of Yarisawa (altitude 1820 m; another 2.5 hours from Tokusawa). The patient’s symptoms became aggravated after sleeping briefly at Tokusawa, and he felt very hot. He assessed himself as having a cold and asked his friend to borrow a thermometer at the front desk of a mountain lodge. The manager of the mountain lodge then referred him to medical care.
He presented at a mountain clinic during the evening, about 2 hours after arriving in Tokusawa. He had a history of infectious mononucleosis and a pyrine allergy. He had smoked 20 cigarettes/day for 20 years but had stopped 2 years previously. He had 30 years of mountaineering/hiking experience. The initial findings were as follows: blood pressure 114/68 mm Hg; pulse 106 beats/min; body temperature 37.6°C; oxygen saturation (SpO2) 80–83% in room air; no cyanosis; clear respiratory sounds; and no obvious dry or moist rales, heart murmur, or edema of the extremities. Portable electrocardiography confirmed normal sinus rhythm. The doctors diagnosed hypoxemia due to pneumonia and/or other disease(s) and suggested an emergency descent. He was given 3 L/min of oxygen, and SpO2 immediately increased to 92%. While waiting 1 hour for evacuation, SpO2 further increased to 96–98%, his pulse decreased to 90 beats/min, and his general fatigue improved.
Examination upon admission to a suburban hospital (altitude 690 m) revealed a pulse of 80 beats/min and SpO2 of 100% upon administration of 3 L/min oxygen. Laboratory findings showed elevated white blood cells and C-reactive protein and decreased arterial partial pressure of oxygen without decreased partial pressure of carbon dioxide (Table). Chest computed tomography images revealed diffuse ground glass opacities in bilateral lung fields and infiltrative shadows in bilateral lower lung fields, indicating atypical pneumonia (Figure). Procalcitonin was also increased, and bacterial pneumonia was suspected (Table). Urinary antigen tests for Legionella pneumophila and Streptococcus pneumoniae and the pharyngeal influenza virus antigen rapid test were all negative.
Laboratory data at suburban hospital on day of symptom manifestation
WBC, white blood cells; Neut, neutrophils; Lym, lymphocytes; Mon, monocytes; Eos, eosinophils; Bas, basophils; RBC, red blood cells; Hb, hemoglobin; Hct, hematocrit; PLT, platelets; CRP, C-reactive protein; pCO2, partial pressure of carbon dioxide; pO2, partial pressure of oxygen; HCO3–, bicarbonate; BE, base excess.
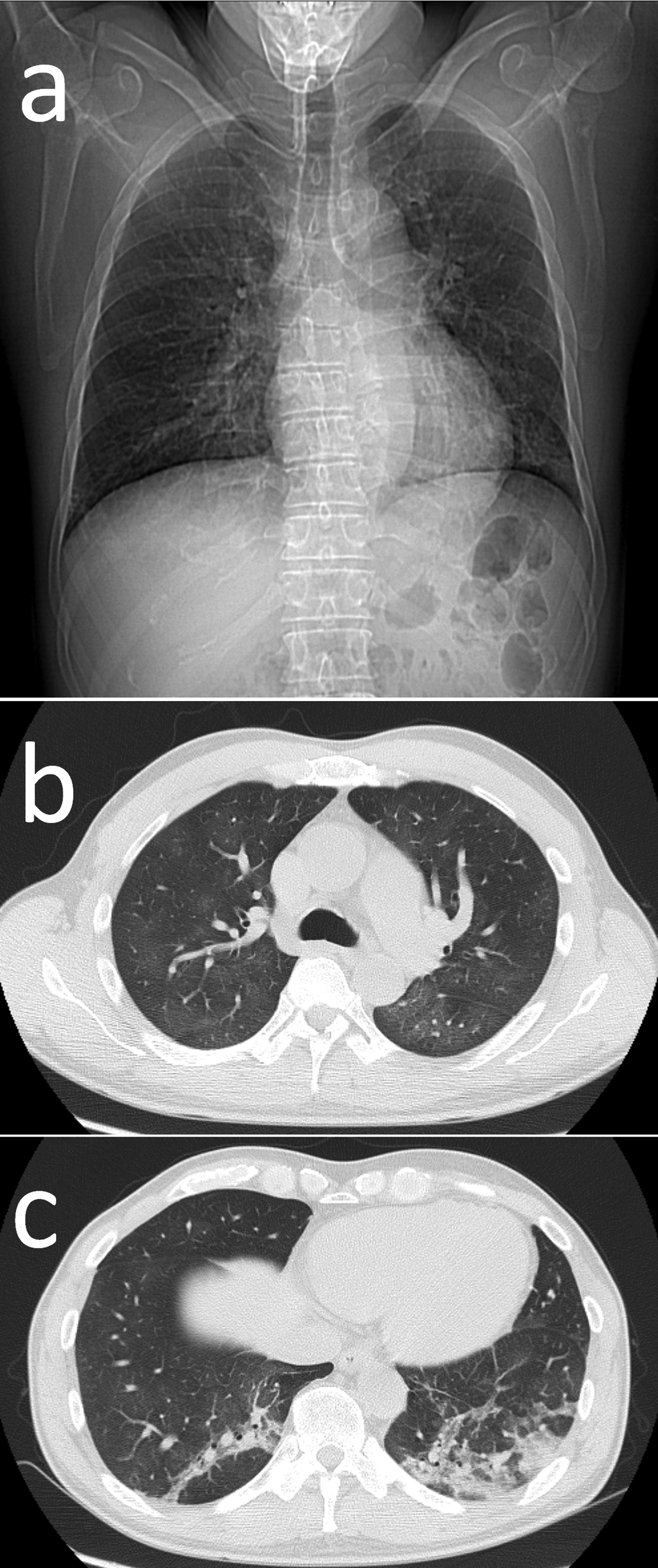
Chest computed tomography findings. A, Positioning image. B, Ground glass opacity. C, Infiltrative shadow.
He was treated with 2 L/min of oxygen inhalation and intravenous sulbactam/ampicillin. The SpO2 improved to 95% in room air on hospital day 3, and he was discharged because of the demands of his job. He attended his general physician in Tokyo for follow-up as recommended by the doctor at the suburban hospital. His general physician then referred him to a respiratory disease specialist at a university hospital. A chest radiograph upon arrival at the university hospital confirmed that his lungs were clear of pneumonia, and he was advised to rest for 4 more days.
During follow-up, the specialist questioned the patient on his use of waterproofing spray and learned that he had used a spray on the day before the hike. He had applied 300 mL of waterproofing spray containing fluororesin and petroleum hydrocarbons to his pack and mountain gear in a closed, narrow, nonventilated entrance at his residence on the night before setting out on the hike. Therefore, he was finally diagnosed with acute pulmonary injury possibly caused by inhaling waterproofing spray with or without bacterial pneumonia.
Discussion
This report describes acute pulmonary damage attributed to inhalation of waterproofing spray that manifested after about 16 to 20 hours while the patient was mountaineering. The 3 primary components of waterproofing sprays are a propellant, a solvent, and a water-repelling agent. Due to the varied and complex composition of spray products, the toxicity of waterproofing aerosol spray remains unclear. 10 –12 However, aerosols that do not attach to target materials will become airborne particles that are considered toxic.11,13 On the other hand, aerosols will disperse and not usually cause chemical pneumonia when applied under the well-ventilated outdoor conditions indicated on the spray product. Aerosol particles with a diameter <10 μm are also established risk factors for chemical pneumonia. 13 Aerosol particles sprayed from hand-pump sprays are usually larger than those from aerosol sprays, but an instance of pulmonary damage caused by exposure to spraying cleaning agents for clothes has been reported. 14 Therefore, any type of spray should be applied with caution.
Smoking cigarettes soon after spraying agents containing fluororesin results in characteristic flulike symptoms that are known as polymer fume fever. 15 The time of onset is usually within minutes to 1 hour, and heated fluorinated polymers exaggerate pulmonary damage. 5 Therefore, polymer fume fever differs somewhat from the pneumonitis associated with fluoropolymer waterproofing sprays. 12 Regardless of disease entities, fluorinated polymers heated by smoking are possible aggravating factors for chemical pneumonia. 5
Pulmonary damage caused by inhaling waterproofing spray manifests as interstitial pneumonia, 6 and rarely as pulmonary edema or alveolar hemorrhage,3,4 but specific symptoms for this pulmonary disease have not been defined. Appropriate medical tests can be delayed when patients self-assess bronchial asthma attacks 9 or when a general physician misdiagnoses patients as having a cold or bronchial asthma at the first consultation.4,8 Our patient had also assessed himself as having a cold and had briefly slept as a remedy, but he also underwent medical tests on the day of symptom manifestation.
A differential diagnosis of acute pulmonary damage due to waterproofing spray includes atypical, bacterial, hypersensitivity, drug-induced, and acute eosinophilic types of pneumonia, cardiogenic pulmonary edema, and collagen-disease lung. High-altitude pulmonary edema would be included in a differential diagnosis at a higher altitude and when pulmonary damage is caused by inhaling ski wax containing fluorocarbon resin at an altitude of 2500 m. 16
Laboratory findings revealed inflammatory reactions, as evidenced by leukocytosis and elevated C-reactive protein. 12 Elevated procalcitonin is a marker of sepsis that implies underlying infectious disease. According to the results, we could not exclude bacterial pneumonia despite a lack of sputum production except for the 2 types of bacteria identified using urinary kits. On the other hand, procalcitonin is elevated in drug-induced liver disease and other nonbacterial diseases.17,18 Thus, the elevated procalcitonin in our patient might have resulted from pulmonary damage caused by waterproofing spray. We could not exclude mycoplasma pneumonia, but his recovery within 1 week in the absence of antibiotics against Mycoplasma suggests that he did not have this type of pneumonia.
Most patients with this type of pulmonary damage recover within 24 hours when supplemented with oxygen or by being placed in fresh air, but severe and prolonged damage has also been described. 12 One patient with a 7-week history of worsening dyspnea recovered 8 weeks later without corticosteroids. 6 One patient with cough, sputum, and chest pain was treated with corticosteroids for 3 years. 4 Another patient treated with corticosteroids for severe pulmonary damage developed reactive airway dysfunction syndrome. 19 Desquamative interstitial pneumonia was confirmed in a patient with prolonged radiological abnormalities 1 month after undergoing about 10 days of steroid therapy. 20 Inhaled beta-2 agonists and corticosteroids are usually effective, 12 but follow-up is required.
Self-reporting or appropriate questionnaires are the only means of identifying the cause of lung injury. Hikers are meant to use waterproofing sprays as indicated on the container. Hikers, mountaineers, and other outdoor enthusiasts who develop pulmonary problems should be questioned about the use of waterproofing sprays.
Conclusions
When hikers present with dyspnea and other common illnesses in mountain areas, a doctor should determine the usage of waterproofing spray to differentiate acute pulmonary damage due to aerosols. Waterproofing aerosols must be applied as indicated on the container and not inside homes or buildings with poor ventilation to avoid inhalation.
Acknowledgments: We are grateful to Dr. Shigeru Masuyama, Tokyo Medical University; Drs. Masayuki Hanaoka and Nobumitsu Kobayashi, Shinshu University; and Dr. Norihiro Harada, Juntendo University for advice regarding interpreting the chest computed tomography findings.
Author Contributions: Study concept and design (TH, SA); acquisition of the data (TH, YH, YT-I, HS, MK, HH): analysis of the data (TH, YH, YT-I, HS, MK, HH, SA); drafting of the manuscript (TH); critical revision of the manuscript (TH, SA); approval of the final version of the manuscript (TH, YH, YT-I, HS, MK, HH, SA).
Financial/Material Support: None.
Disclosures: None.
Footnotes
☆
The content of this manuscript was formally presented at the 7th World Congress of Mountain and Wilderness Medicine, August 1, 2016, in Telluride, Colorado, USA.