
Abstract
Acute kidney injury (AKI) is an unusual complication of wasp stings. Treatment of established AKI is largely supportive but the preventive strategies are not well documented. This is a report of 2 human cases that developed AKI after multiple wasp stings (Vespa magnifica). Each patient reached the hospital early in their clinical course and was treated with intravenous hydration and urine alkalization. In both the cases the severity of AKI, morbidity, and duration of hospitalization were reduced. The requirement of dialysis therapy was avoided. We propose early treatment with intravenous hydration, diuretic administration, and urine alkalization in such cases to prevent systemic and renal complications.
Introduction
Insects that sting are members of the order Hymenoptera of the class Insecta. Medically important insects belong to families of Vespidae (yellow jacket, hornet, and wasp) and Apidae (honeybee and bumblebee).1,2 Stinging events involving honeybees and wasps are not rare. Clinical manifestations depend on the victim’s sensitivity to the venom and the number of stings; most deaths or clinically important incidents involve very few stings (<10) and anaphylactic shock. However, mass stinging events involving tens to hundreds of wasp stings can prove life threatening via toxic action of the venom when injected in large amount. 2 Acute kidney injury (AKI) after multiple hymenoptera stings is a rare phenomenon. Victims of multiple wasp or bee stings can experience a triad of intravascular hemolysis, rhabdomyolysis, and AKI. Usual causes of AKI are intravascular hemolysis, rhabdomyolysis, shock, and the direct toxic effects of the venom. 3 More than half of the victims who experience multiple wasp or bee stings develop AKI, and most of these patients require intermittent hemodialysis or peritoneal dialysis. 4 –7 The mortality rate of patients who experience AKI has been reported to be as high as 25%. 3 This is a report of 2 cases of AKI following multiple wasp stings in which severity of illness was reduced and recovery time was shortened due to early institution of aggressive treatment. Informed consent for publication was obtained from both the patients and the hospital ethics committee.
Case 1
A 72-year-old man was stung by a swarm of wasps (Vespa magnifica) at multiple sites all over the body while he was grazing cattle in the forest. Immediately he developed severe pain at the site of stings and nausea followed by repeated episodes of vomiting. There was no history of symptoms of breathlessness or wheeze, abdominal pain, diarrhea, hematuria or cola-colored urine, or syncopal attacks. He was transported in a motor vehicle and reached our medical center within 1 hour of the incident. On arrival in the emergency department, he was hemodynamically stable, with a pulse of 88 beats/min, blood pressure of 140/70 mm Hg, and respiratory rate of 20 breaths/min. There was periorbital swelling and multiple sting marks (∼100) over the head, trunk, and extremities. His skin was infiltrated by edema and stung areas were edematous and erythematous. No other abnormalities were found on systemic examination. The blood investigation results are shown in the Table. Examination of urine showed trace albumin, no glucose, 10-12/high power field white blood count, occasional red cells, and the culture was sterile.
Results of the blood investigations
WBC, white blood cell; AST, aspartate aminotransferase; ALT, alanine amintransferase; CPK, creatine phosphokinase; LDH, lactate dehydrogenase.
The investigation revealed evidence of intravascular hemolysis, rhabdomyolysis, hepatic dysfunction, and acute kidney injury. The patient was treated with an injection of hydrocortisone, antihistamines, intravenous fluids (2.5–3 L), and forced alkaline diuresis (100 mmol bicarbonate and furosemide injection 80 mg). He received steroids, antibiotics, and other supportive therapy for a week. Patient improved with this treatment, remained nonoliguric, did not require dialysis, and the renal functions normalized on day 7 (Figure 1).
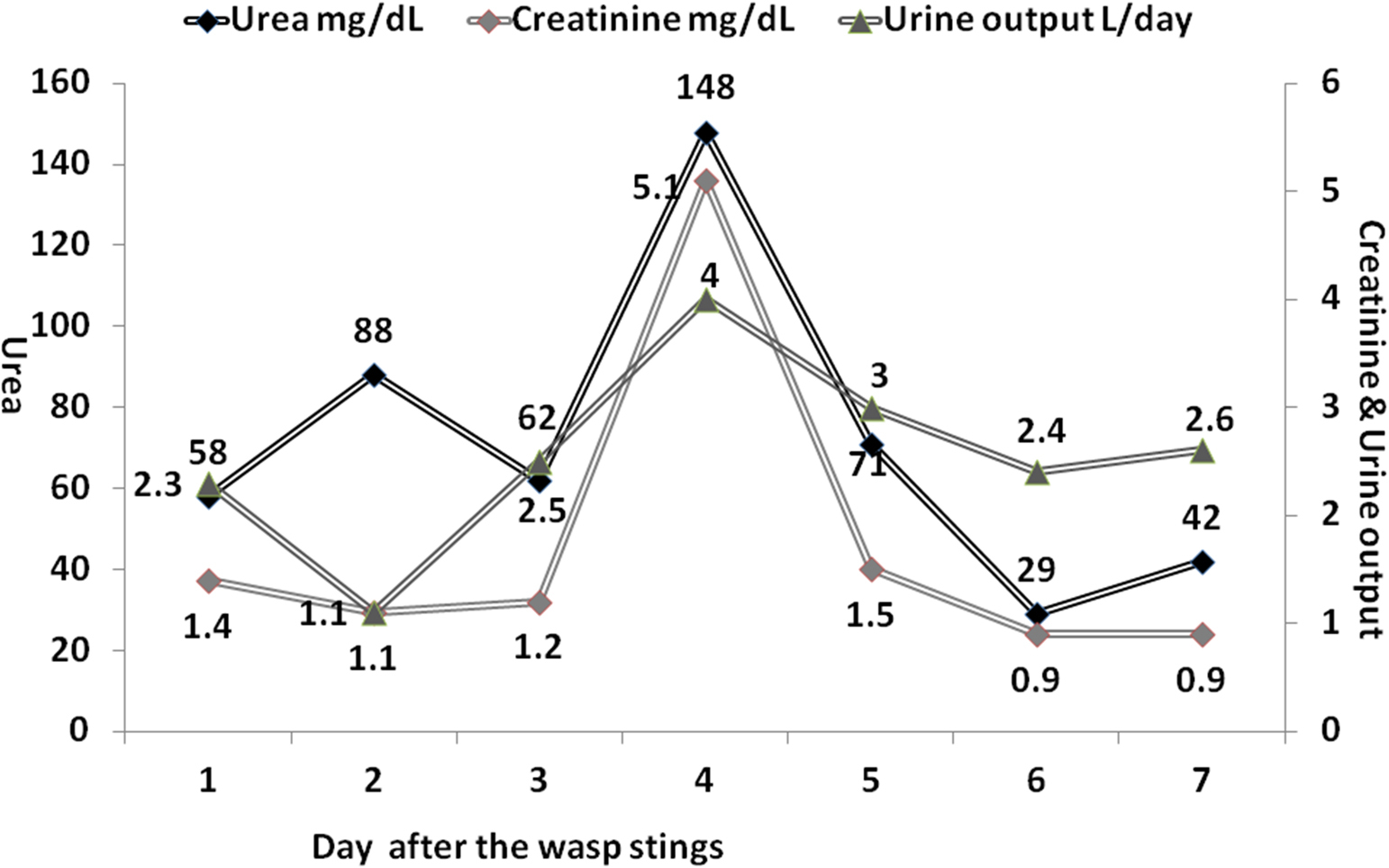
Course of renal function tests and urine output.
Case 2
A 40-year-old man was stung by a swarm of wasps (Vespa magnifica) at multiple sites (head, face, trunk, and both upper extremities) while he was working in the fields. He developed pain and itching at the site of stings. He was treated at a local hospital with injections of hydrocortisone and antihistamines. He developed difficulty in breathing, periorbital swelling, and decreased urine output and was referred to this hospital. There was no history of symptoms of nausea, vomiting, abdominal pain, diarrhea, hematuria or cola-colored urine, or syncopal attacks. On arrival at our medical center 9 hours after the incident, he had a pulse of 90 beats/min, blood pressure of 180/130 mm Hg, and respiratory rate of 18 breaths/min. He had periorbital swelling and multiple sting marks (∼100) over the head, trunk, and upper extremities. His skin was infiltrated by edema and stung areas were edematous and erythematous. No other abnormalities were on systemic examination.
The blood investigation results are shown in the Table. Urine examination found albumin 2+, glucose 0, and plenty of red cells were present. The patient was known hypertensive and the blood pressure was controlled with oral amlodipine 10 mg daily.
The investigation revealed evidence of intravascular hemolysis, rhabdomyolysis, hepatic dysfunction, and acute kidney injury. The patient received aggressive intravenous fluid therapy (2.5–3 L) along with forced alkaline diuresis (100 mmol bicarbonate and furosemide injection 80 mg). He was treated with steroids, antihistamines, antibiotics, and other supportive therapy for a week. The patient improved with this treatment, remained nonoliguric, did not require dialysis, and renal functions normalized at discharge on day 6 (Figure 2).
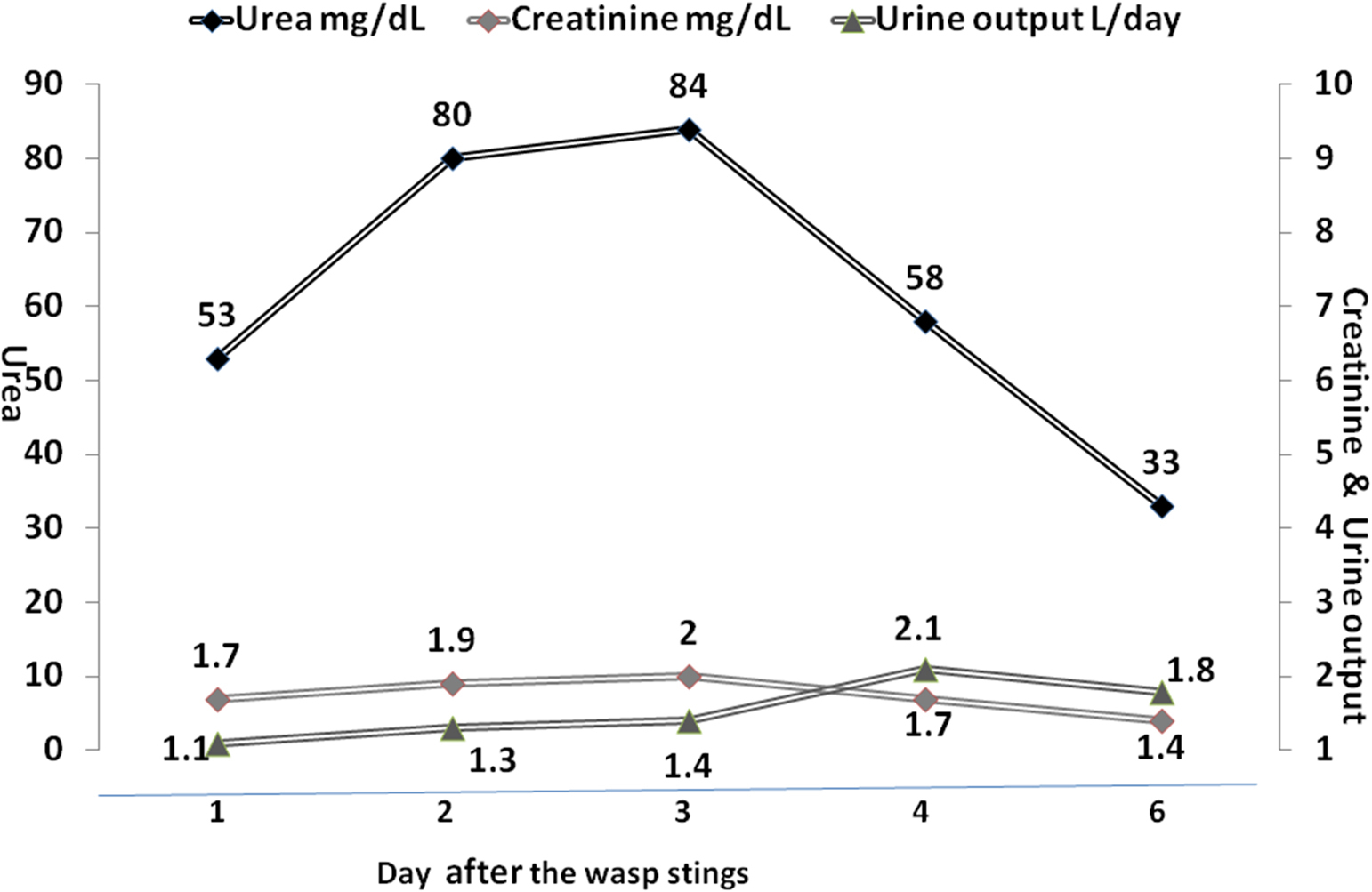
Course of renal function tests and urine output.
Discussion
In attacks involving multiple stings, AKI or death may result from 20 to 200 wasp stings or 150 to 1000 bee stings. 2 Multiple stings result in a unique syndrome of intravascular hemolysis, rhabdomyolysis, AKI, and hepatitis. 3 Accidents due to massive attack with hundreds or thousands of Africanized bees are well known. Because of their aggressive behavior and the number of accidents associated with them, the Africanized bees are also known as “killer bees.”6,7
Hymenoptera venoms are complex mixtures of biologically active peptides, enzymes, and amines. Bee venom contains melittin, phospholipase A2, mast cell–degranulating peptide (peptide 401), hyaluronidase, and apamin, among other constituents. 8 Melittin, which makes up approximately 50% of the entire bee venom mixture, powerfully disrupts cell membranes and has direct toxic effects on renal tubular cells of the host.9,10 Wasp venom lacks melittin; instead it contains antigen 5 as the main allergen. 8 These components have direct and indirect cytotoxic (hepatic, renal, and myocyte membrane), hemolytic, neurotoxic, and vasoactive properties, which can cause intravascular hemolysis and rhabdomyolysis. Phospholipase A2 is believed to trigger the release of arachidonic acid from lipids in the cell membrane, which initiates the production of inflammatory eicosanoids. Hyaluronidase in the venom causes breakdown of connective tissues, thereby facilitating the spread of the venom.9,11
Acute tubular necrosis, pigment nephropathy resulting from rhabdomyolysis (myoglobinuria) or intravascular hemolysis (hemoglobinuria), hypotension caused by anaphylactic reaction, direct nephrotoxicity, and acute interstitial nephritis are several mechanisms of AKI due to Hymenoptera venom. 3 Acute tubular necrosis secondary to intravascular hemolysis and or rhabdomyolysis is the primary cause of AKI after Hymenoptera envenomation. Hemolysis and rhabdomyolysis can induce AKI, particularly in hypovolemic or acidotic individuals. It has been postulated that hemoglobin and myoglobin cause AKI by toxic effects on tubule epithelial cells or by inducing intratubular cast formation. Hypovolemia or acidosis may contribute to the pathogenesis of AKI in this setting by promoting intratubular cast formation. In addition, both hemoglobin and myoglobin are potent inhibitors of nitric oxide bioactivity and may trigger intrarenal vasoconstriction and ischemia in patients with borderline renal hypoperfusion. 12
The major treatment strategy is to 1) correct the hypovolemia and attend to the renal ischemia; 2) enhance the clearance of hemproteins, toxins, or toxic wastes from the circulation and the kidney; and 3) alleviate the direct adverse consequences of venom toxins, toxic wastes, electrolyte imbalance, and hemproteins on kidneys and other organs. The early pharmacological intervention incorporates the volume replacement and alkaline diuresis in order to prevent the factors that lead to AKI, such as dehydration and renal hypoperfusion, intratubular cast formation and tubular obstruction, aciduria, and free radical release. 3 ,5–7,12 Indeed, some of the early-treated patients may not require dialysis as was seen in both the cases who were treated with alkaline diuresis as they arrived early (1–9 hours after being stung) and recovered without dialysis. However, in patients with established AKI the only reliable therapeutic intervention is extracorporeal blood purification such as intermittent hemodialysis, continuous renal replacement therapy, peritoneal dialysis, and plasmapheresis (whenever indicated). 3 ,4,9,11 Thus, the treatment of established AKI is largely supportive in nature, with renal replacement therapy being the cornerstone. 13
The novelty of this report lies in the fact that both the patients arrived in this hospital early after sustaining mass stinging by the wasps. The patients with multiple wasp stings are likely to develop the complications of intravascular hemolysis, rhabdomylysis, and AKI. In anticipation of these complication, an aggressive hydration and urine alkalization to a pH of >6.5 was instituted early to prevent AKI due to hemglobinuria and myglobinuria. In both the cases the severity of AKI, morbidity, and the duration of hospitalization were decreased and need for dialysis was avoided altogether.
Since there is no antivenom for wasp stings and treatment in all such cases is supportive, we propose that patients with multiple wasp stings be hospitalized for aggressive hydration and urine alkalinization to prevent the AKI secondary to hemolysis and rhabdomyolysis.
Author Contributions: SV: conceived the study, compiled and analyzed the data, and wrote the paper. AP: participated in writing the manuscript.
Financial/Material Support: None
Disclosures: None.