
Abstract
High altitude pulmonary edema (HAPE) is a potentially life-threatening form of noncardiogenic pulmonary edema that may develop in otherwise healthy individuals upon ascent to high altitude. A constitutional susceptibility has been noted in some individuals, whereas others appear not to be susceptible at all. In our report, we present a case of HAPE triggered by concurrent respiratory tract infection and strenuous exercise in a mining worker with an abnormal rise in pulmonary artery pressure in response to acute hypoxia, without a prior history of HAPE during almost a year of commuting between high altitude and lowland areas.
Keywords
Introduction
High altitude pulmonary edema (HAPE) is a potentially life-threatening form of noncardiogenic pulmonary edema that may develop in otherwise healthy individuals in the 2 to 5 days after rapid ascent to altitudes above 2400 m. 1 The incidence of HAPE varies from 0.01 to 0.1% at ski resorts in the Rocky Mountains (Colorado, 3000–3600 m) 2 to 15% in Indian soldiers at 5500 m. 3 However, the incidence of HAPE in nonacclimatized lowlanders depends not only on the altitude of sojourning, but also on the speed of ascent and the individual predisposition. 4 Numerous studies have revealed that individuals under the same conditions show different levels of susceptibility to HAPE. 5 A constitutional susceptibility has been noted, as the condition tends to recur in the same individuals when ascending rapidly to high altitudes between 3000 and 4500 m. 6 Indeed, a prior history of HAPE is an important predisposing factor that renders an individual prone to HAPE. Risk factors for HAPE also include the rate of ascent, male sex, preexisting lung or cardiac disorders, and an exaggerated rise in pulmonary artery pressure in response to acute hypoxia.7,8 Furthermore, intense physical exercise 9 and concurrent respiratory tract infection can provoke HAPE.10,11 This case report describes a mining worker with an abnormal rise in pulmonary artery pressure in response to acute hypoxia, but who had no prior history of HAPE during 10 months of commuting between high altitude and lowland areas, and who developed HAPE after concurrent respiratory tract infection and strenuous exercise.
Case Report
A 28-year-old Kyrgyzstan male worker at the gold mining company was referred to our department for evaluation of shortness of breath and hypoxemia that developed during his shift while working at high altitude. All high altitude workers of the mining company undergo a preemployment health screen and an annual checkup at a single specially-designated clinic in Bishkek (760 m). Apart from clinical examination and specialist counseling, clinical lab work (blood cell count, urine analysis, and biochemistry), electrocardiogram (ECG), echocardiography, chest X-ray, sonography, and spirometry are usually conducted. Mine employees are transported to the mine site by bus. The overall ascent lasts 7 hours. The living quarters at the mine are located at an altitude of 3700 m, and the open-pit mine operates at altitudes between 3800 and 4500 m (Tian Shan mountain range, Kyrgyzstan). The workers commute between high altitude and lowland (760–1600 m) on a 2-week shift rotation. The patient had been working as a mechanic (moderate to heavy workload) at the high altitude gold mine for 10 months without any health or acclimatization problems. According to the rules of the company, on arrival (the first day of ascent), all employees should have a respite with the working shift that begins on the next day. However, during this rotation, the patient had to start working on the first day because of an urgent situation.
In the evening of the second day at high altitude, the patient complained of a sore throat, dry cough, and headache. He attributed these symptoms to cold exposure, as he had worked outside in rainy and windy weather. The next morning, he experienced chills, weakness, and increased cough. As the worker was unwilling to visit a doctor, he took paracetamol and continued working throughout the day. On the fourth day, his condition became worse: he experienced a productive cough with clear white sputum, increased fatigue, and headache. At the doctor’s office, the patient’s vital signs were as follows: blood pressure 120/78 mm Hg, heart rate 98 bpm, respiratory rate 24 breaths/min, temperature 37.5°C, and SpO2 89%. He was diagnosed as having “acute pharyngitis” and he received paracetamol and was given a day off. However, the patient was brought back to the doctor 7 hours later because of further deterioration, which included the following symptoms: severe fatigue, dyspnea at rest, productive cough with mucous sputum, and persistent headache. Vital signs included the following: blood pressure 120/80 mm Hg, heart rate 140 beats/min, respiratory rate 32 breaths/min, temperature 37.7°C, and SpO2 70% while breathing ambient air. On chest auscultation, crackles were heard over both lungs. Administration of 5 L/min of supplemental oxygen via a face mask at an FIO2 of 100% for 15 minutes slightly diminished the dyspnea and fatigue, decreased the heart rate to 125 beats/min, and increased the SpO2 up to 80%. ECG showed sinus tachycardia with a right axis deviation and a late precordial R/S transition (Figure 1A). Because the chest radiograph showed signs of interstitial pulmonary edema (Figure 2), the patient was immediately evacuated by vehicle to Bishkek (approximately 7 hours).
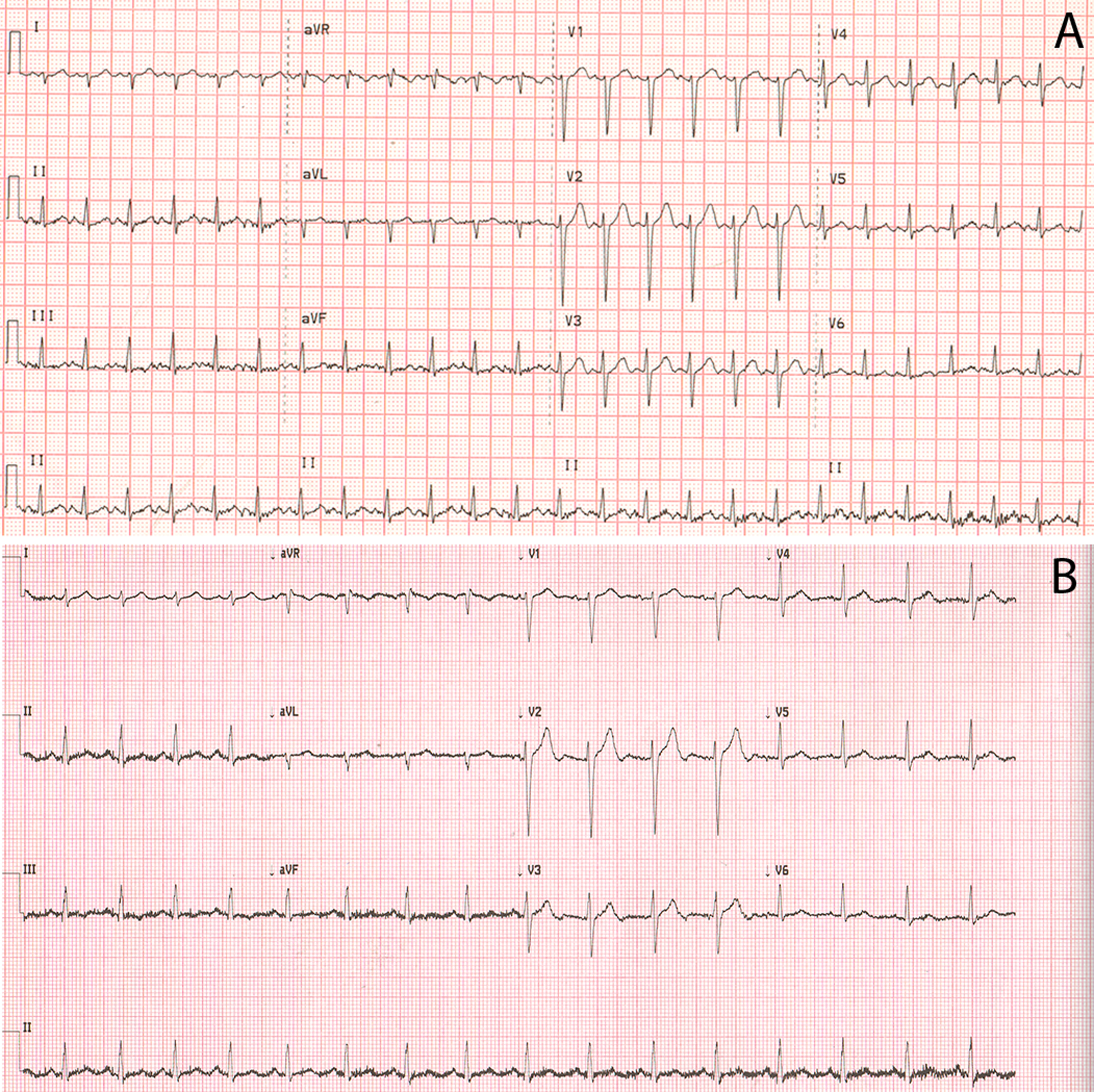
Electrocardiograms (ECG) taken at high altitude during HAPE (A) and at low altitude after recovery from HAPE (B).
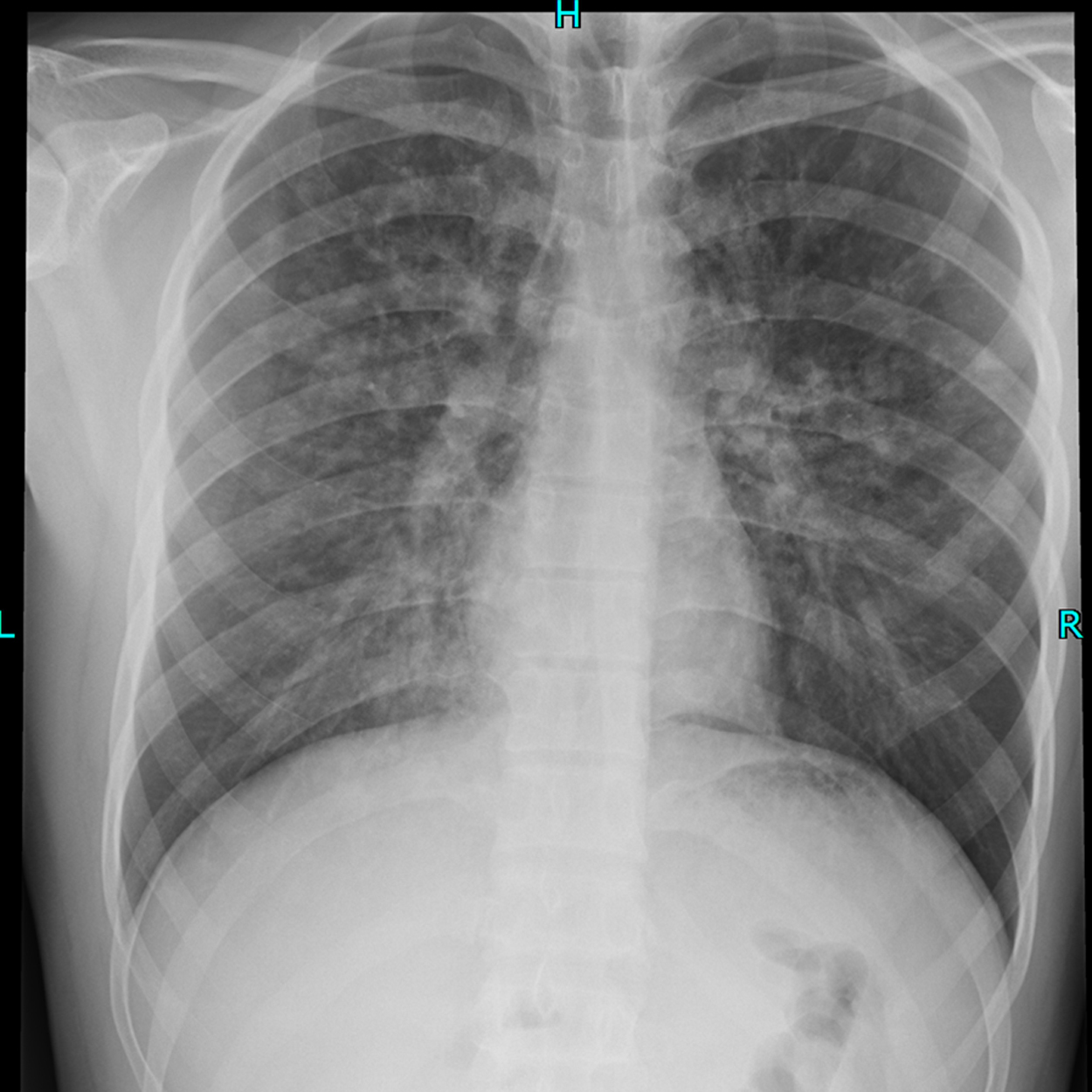
Posterior-anterior X-ray view of the chest showing pulmonary edema.
On admission, the patient’s vital signs were taken again: blood pressure 110/70 mm Hg, heart rate 120 beats/min, respiratory rate 28 breaths/min, temperature 37.1°C, and SpO2 90% while breathing ambient air. On auscultation, crackles over both lungs persisted. Complete blood count was normal, sputum was nonpurulent, and biochemical blood tests were within normal ranges. The patient was diagnosed as having resolving HAPE and acute pharyngitis, and was treated with bed rest, supplemental oxygen, and expectorants. On the second day, the patient felt significant improvement in his condition. The shortness of breath and fatigue had disappeared; however, the productive cough with sputum persisted. On the third day at the clinic, the patient noticed relief of the cough. His temperature and oxygen saturation while breathing ambient air normalized, and no crackles were heard on chest auscultation. Repeat chest X-ray showed full resolution of the pulmonary edema. A pulmonary function test, abdominal ultrasound, and ECG (Figure 1B) were performed after recovery and did not reveal any abnormalities. On resting echocardiography, right ventricular size and function were normal. This may be due to an echocardiography that was performed with delay and at low altitude. 12 Doppler echocardiography revealed a significant increase in the tricuspid pressure gradient from 24.9 mm Hg to 67.7 mm Hg after 1 hour of breathing a 12% oxygen mixture (Figure 3A and B). The patient resumed working at the mine, and has been working at high altitude for 9 more months without the recurrence of HAPE. Repeat Doppler echocardiography performed 9 months later showed a significant increase in the tricuspid pressure gradient from 25.8 mm Hg to 70.8 mm Hg after 1 hour of breathing a 12% oxygen mixture, and subsequently confirmed an exaggerated hypoxic pulmonary vasoconstrictive response in this person.
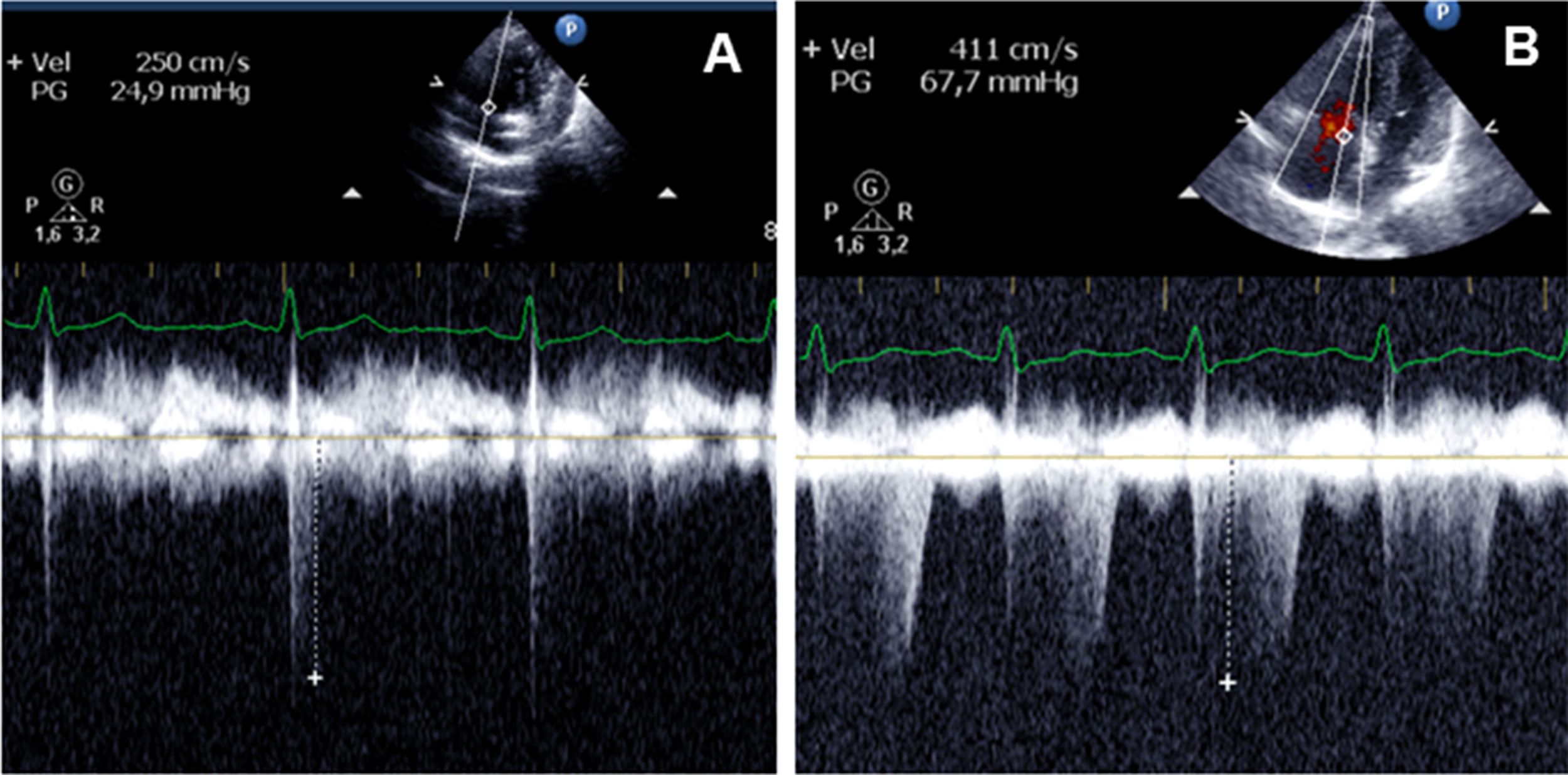
Peak tricuspid regurgitation jet velocity estimating right ventricular systolic pressure while breathing room air (A) and while breathing a 12% hypoxic gas mixture (B).
Discussion
HAPE is a form of high altitude illness characterized by cough and progressive dyspnea that may develop in otherwise healthy people ascending to high altitude. HAPE begins with a subtle nonproductive cough and shortness of breath, which progresses to a productive cough with pink, frothy sputum and a debilitating degree of dyspnea in severe cases. Subjects become tachypneic and tachycardic, and have crackles on chest auscultation. If the condition worsens, death may ensue. HAPE typically occurs at altitudes >3000 m, and is the leading cause of death from altitude illness.
The incidence of HAPE varies significantly depending on the altitude, rate of ascent, and genetic predisposition. For example, in otherwise healthy unselected subjects ascending rapidly to 4500 m, the incidence of HAPE is approximately 6%, whereas it is approximately 60% in HAPE-susceptible individuals. 6 A prior history of HAPE is an important predisposing factor that renders an individual to HAPE. Although high altitude hypoxia causes hypoxic pulmonary vasoconstriction with a moderate increase in pulmonary vascular resistance and pulmonary artery pressure in most people, 13 susceptible individuals have an abnormal rise in pulmonary artery pressure in response to acute hypoxia. 8 Our patient displayed an exaggerated pulmonary artery pressure in response to breathing a hypoxic gas mixture that rendered him prone to HAPE. Notably, the patient had numerous ascents to high altitude for more than 10 months without any significant health problems before this event. Furthermore, since his recovery from HAPE, the patient has been commuting between high altitude and lowland areas for 9 months without recurrence of HAPE. Although HAPE-susceptible subjects display abnormal pulmonary vascular responses to hypoxia,8,14 some studies have suggested that an exaggerated pulmonary hypertension is not sufficient to trigger HAPE.15,16 However, we believe that development of HAPE in persons with an exaggerated hypoxic pulmonary vasoconstrictive response can be provoked by the concurrent presence of several other HAPE risk factors, such as rapid ascent, individual susceptibility, preceding viral upper respiratory tract infection, and engagement in strenuous physical activity during the first days of acclimatization to high altitude.4,17 Indeed, gradual ascent to high altitude can prevent HAPE in most HAPE-susceptible persons. 4 Furthermore, the occurrence of HAPE is also dependent on home elevation (ie, the absolute altitude difference) and preacclimatization. 9
Although it is believed that inflammation is not an etiologic factor in the pathogenesis of HAPE,14,18 additional factors such as inflammatory mediators might favor increased vascular permeability.19,20 Elevated inflammatory mediators have been found in the bronchoalveolar lavage fluids and in the urine of patients with HAPE.21,22 Furthermore, a strong association between the presence of a preexisting inflammatory illness and the development of HAPE was reported in children visiting high altitude, 11 although this has not been studied in a controlled manner. Our patient had the typical signs and symptoms of the common cold, which included sore throat, cough with mucous sputum, headache, fatigue, chills, and low-grade fever. The development of signs and symptoms of the common cold associated with cold exposure, 23 adequate SpO2 (≥89%), and the absence of crackles early in the course of the disease are all suggestive of the presence of respiratory tract infection preceding the development of HAPE.
In our opinion, the subject did not develop HAPE in the past because no other precipitating risk factors were present. Although the individual has had numerous ascents to high altitude, the speed of ascent remained constant at all times. Moreover, he might have developed some degree of acclimatization as a result of commuting between high altitude and lowland areas.24,25 In addition, the company employees usually have a day of rest after ascent before beginning their shift at high altitude. Furthermore, home altitude (Bishkek) of the subject is located at 760 m; therefore, the absolute altitude difference between his place of residence and the mining site is smaller than the difference in cases of HAPE observed in sea-level residents. 14 However, when additional risk factors such as viral upper respiratory tract infection and engagement in increased physical activity during the first days of high altitude acclimatization were present, the patient developed HAPE. This case also illustrates that even individuals with an exaggerated pulmonary artery pressure response to acute hypoxia can successfully acclimatize to high altitude by controlling the rate of ascent, and avoiding unprotected exposure to extreme environmental cold and strenuous exercise during the first day at altitude.
Acknowledgment: The authors thank the patient for allowing us to present this case.
Financial/Material Support: None.
Disclosures: None.
Footnotes
Submitted for publication September, 2016.
Accepted for publication April, 2017.