
Abstract
We discuss the case of an experienced diver who ran out of air during his final ascent while scuba diving. He lost consciousness rapidly after surfacing and despite immediate cardiopulmonary resuscitation, could not be revived. On arrival at the emergency department he was noted to have copious amounts of blood in his upper airway and had developed extensive subcutaneous emphysema. Large amounts of air were observed in the central circulation following a postmortem computerized tomography scan as well as pneumomediastinum, a small right-sided hemothorax, and extensive subcutaneous emphysema. We discuss several potential pathophysiological mechanisms that might explain these findings. Finally, we end with a recommendation for an expedient whole-body postmortem computerized tomography scan and autopsy by a suitably qualified pathologist in the investigation of all dive-related fatalities, where possible.
Introduction
Recreational diving is an ever-popular sport with an estimated 6 million active divers worldwide, 1 and although considered a safe activity, fatalities do happen. Historically, drowning was the autopsy diagnosis in 80% of cases, followed by air embolism secondary to pulmonary barotrauma (PBT) in 10%. 2 But errant reporting has skewed these figures. Many victims present to pathologists who are inexperienced in the investigation of diving fatalities and who may fail to appreciate that drowning is simply the final act in a series of events. In divers, drowning is more of a reflection of the medium in which the death happened rather than the cause of the death itself. 3 More recent data found that asphyxia (drowning and running out of air), arterial gas embolism (AGE), and acute cardiac events account for 85% of all diving-related fatalities. 4
The push to differentiate subjects dying of asphyctic syndrome secondary to drowning and subjects found dead in the water from other causes is important if we are to better understand the mechanisms of death behind such tragic events. In that regard, we present the case of a scuba diving victim who died suddenly upon surfacing and discuss the pathophysiology behind the most likely cause(s) of death.
Case history
A previously fit and healthy 59-year-old male Japanese tourist presented to the Emergency Department (ED) of Belau National Hospital, Palau via ambulance in cardiopulmonary arrest. He was an experienced diver, achieving rescue diver status, with more than 2300 logged dives. The victim had no known past medical history and was not taking any regular medication. He presented to the ED having just completed his third dive of the day, the previous 2 being uneventful. All 3 dives were no-decompression profiles, using open-circuit scuba on air. Both the diver and the dive instructor wore dive computers, which they used to monitor their decompression obligations. The victim’s computer was interrogated subsequently and no alarms/warnings were noted. For each of the 3 days before the accident the deceased had conducted 4 dives, each lasting approximately 30 minutes to a maximum depth of 30 m. On the day he presented to the ED, he had completed the following dives: the first dive lasted 30 minutes to a maximum depth of 38 m. The surface interval to the second dive was 1 hour and this dive was also for 30 minutes to a maximum depth of 35 m. The surface interval to the third dive was also 1 hour. The third dive was uneventful until the end. The maximum depth was 30 m and total dive time of around 25 minutes. At the beginning of the final ascent, some 20 minutes into the dive, the dive instructor recalled that there were no problems. At 17 m (24 minutes dive time) the instructor noticed that the victim was using a fellow customer’s primary gas supply via his second stage mouthpiece (octopus). Immediately, she confirmed normal respirations and, using hand signals, that he was “OK.” He chose to ascend using the same regulator (belonging to his buddy) at a safe rate.
Two minutes after commencing the safety stop at 5 m, the patient became progressively agitated and tachypneic. After the dive instructor had been unsuccessful in her attempts to calm him down, she switched him onto her octopus and brought him to the surface. Once above water, she found him to be uncontrollably agitated, tachypneic, and producing incoherent speech. He was moving all 4 limbs equally. He rapidly lost consciousness and stopped breathing. Cardiopulmonary resuscitation (CPR) was commenced immediately while still in the water and continued once back on the boat.
An automated external defibrillator was immediately attached and the patient was shocked twice but without a return of spontaneous circulation. He arrived in the ED around 90 minutes after he lost consciousness, having continued to receive CPR in the meantime. Initial assessment revealed no signs of life. The airway was filled with copious amounts of fresh blood, which was hard to clear with suctioning. Endotracheal intubation was not attempted. Rhythm analysis demonstrated asystole and CPR was terminated soon thereafter. No external injuries were noted. A widespread, grossly bloated appearance was observed that affected most of the skin surface (including the face, neck, trunk, arms, hands, legs, and feet) with underlying crepitus commensurate with significant subcutaneous emphysema. This had become obvious to the dive instructor about 20 minutes after she had commenced CPR. After the victim had died, the dive instructor had inspected the victim’s diving equipment for faults. She found that the regulator was working properly. She noted that the victim had started his last dive with a full tank (11 L, 200 bar) but, when she examined it, found it was empty. The authors acknowledge that, ideally, the equipment should be examined by a neutral third-party specialist. Of note, no other individuals on the dive, including the dive instructor, suffered any ill effects after the third dive.
A postmortem computed tomography scan (PMCT) of the thorax and abdomen, taken at 100 minutes after he lost consciousness, demonstrated significant subcutaneous emphysema and pneumomediastinum, a small right-sided hemothorax, bilateral pulmonary infiltrates, a small pneumopericardium and extensive pneumocardium (Figure 1), complete filling of the pulmonary artery and ascending aorta (Figure 2), and complete pneumatization of the supra-aortic vessels (Figure 3). Air was also noted in the portomesenteric venous system. No air was noted in the coronary arteries. Due to a lack of suitably qualified personnel, an autopsy was not undertaken. At the time, death was attributed to obstruction of the central circulation with air secondary to PBT.
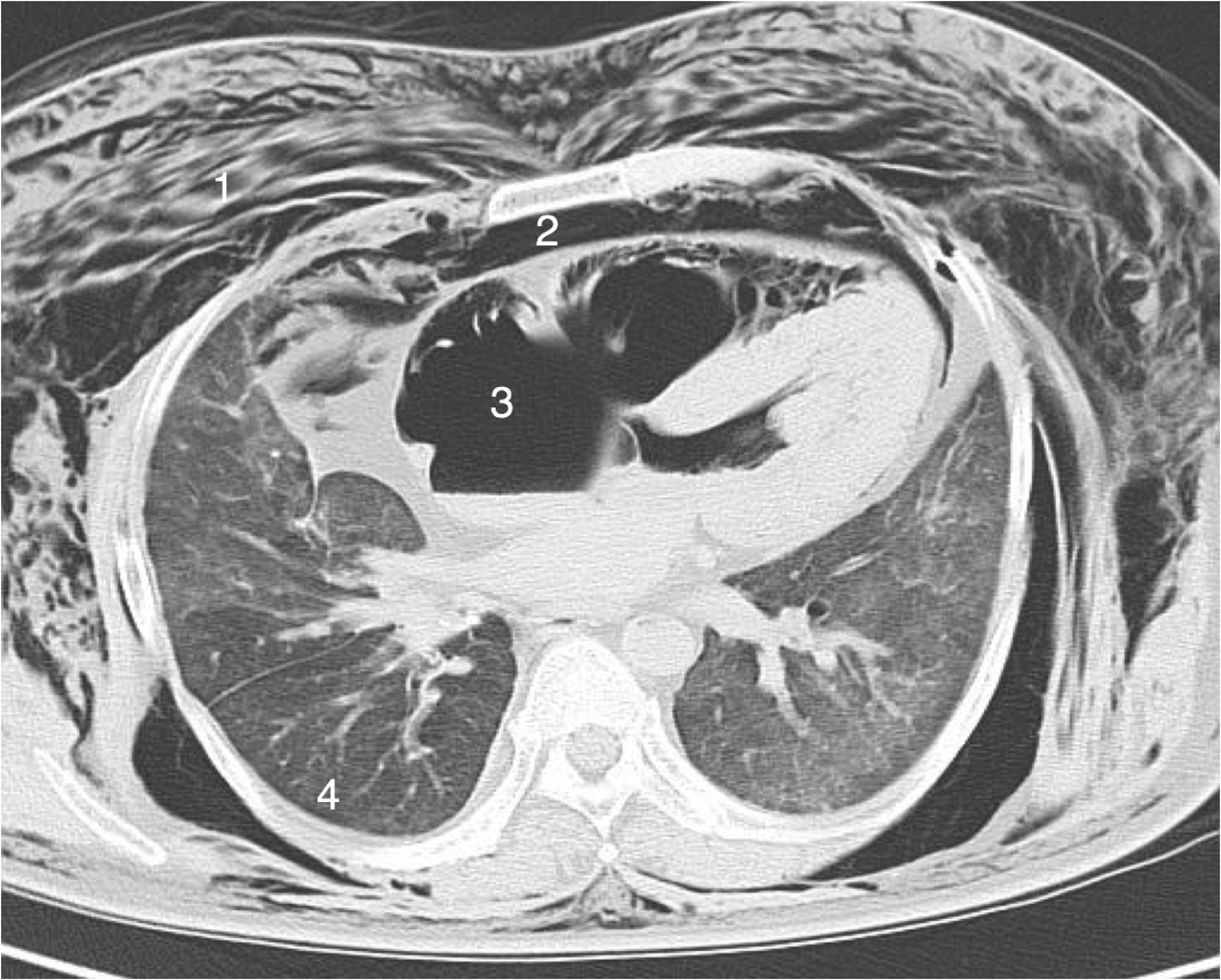
Axial CT scan showing extensive subcutaneous emphysema (1), pneumomediastinum (2), pneumocardium (with a fluid level in the left atrium) (3), and a small right-sided hemothorax (4).
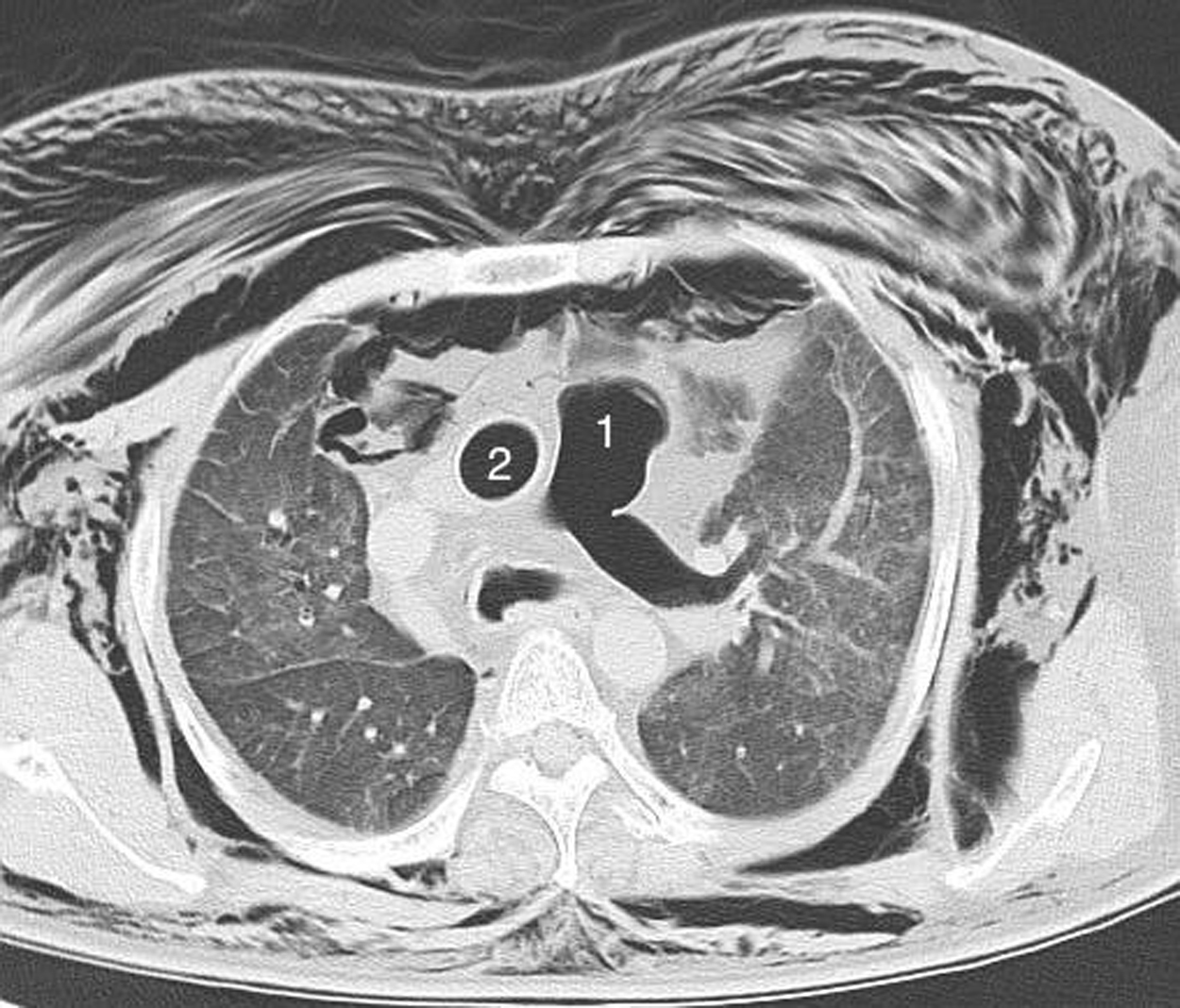
Axial CT scan showing extensive air in the pulmonary arteries (1) and ascending aorta (2).
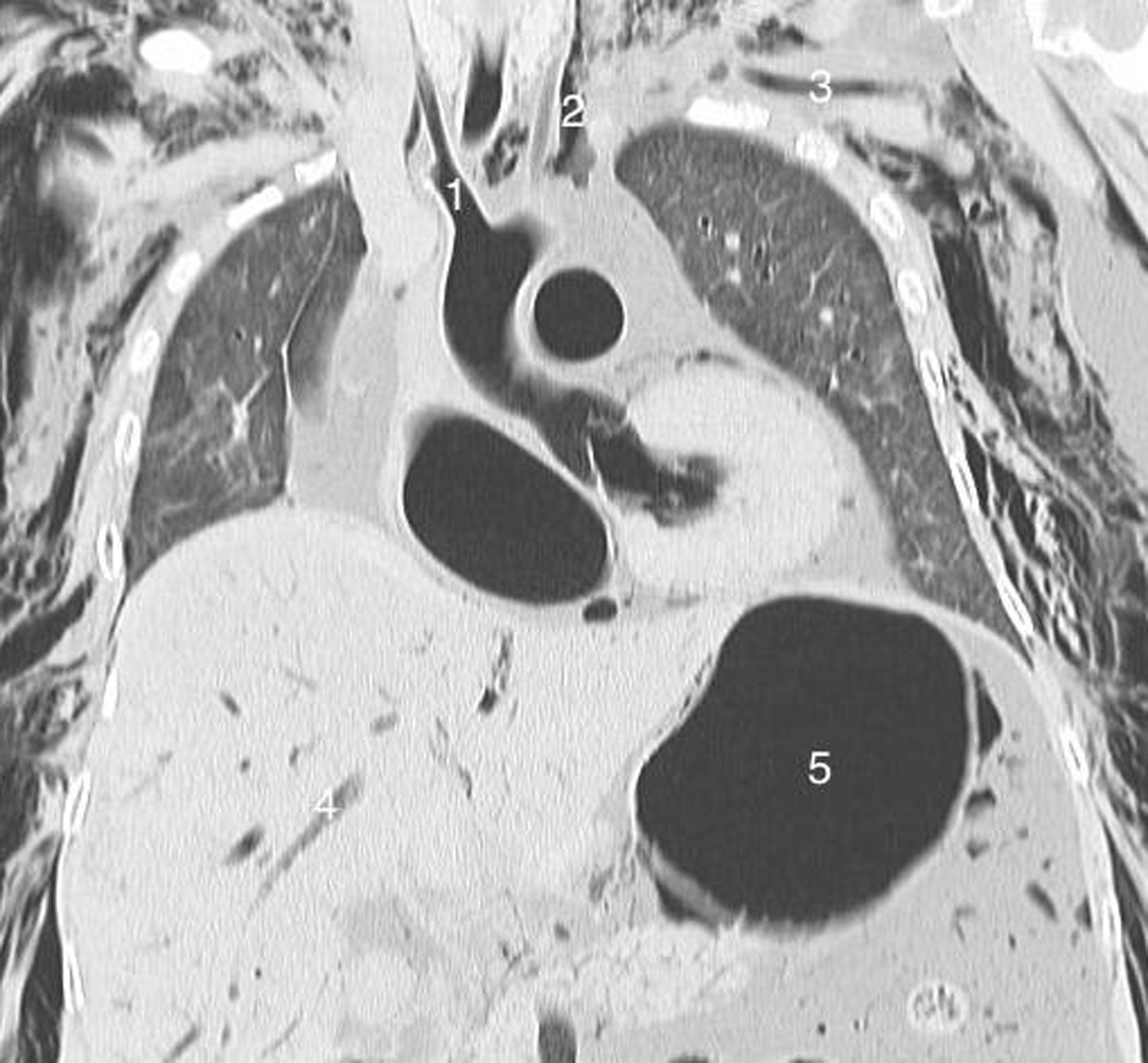
Coronal CT scan showing complete pneumatization of the supra-aortic vessels, namely the brachiocephalic artery (1), right and left common carotid arteries (2), and the left subclavian artery (3). Air is also noted in the portomesenteric venous system (4) and stomach (5).
Discussion
PMCT has left an indelible albeit controversial mark on the assessment of fatal diving events. It is now utilized as an adjunct to, or even replacement for, a formal autopsy. It is particularly useful in defining the topography and volume of abnormal gases in divers who have died suddenly during, or shortly after, diving. 5 This view is controversial because these gases are not necessarily pathognomonic or specific for a particular mechanism of death related to diving, 2 and PMCT has limited usefulness in detecting nongaseous pathology compared with a conventional autopsy.
The potential causes of these abnormal gases are PBT, decompression sickness (DCS), postmortem decompression artefact (PMDA) or tissue off-gassing, resuscitation artefacts, and putrefaction gas, all of which we shall discuss in relation to our case.
Most diving-related complications can be explained by the behavior of gases in relation to changing ambient pressure. Boyle’s law states that at a constant temperature, the volume of a gas varies inversely with the ambient pressure (P1V1 = P2V2). Henry’s law states that the solubility of a gas in liquid is directly proportional to the partial pressure of that gas; in sport diving, this mostly concerns nitrogen. Both of these gas laws can help explain the possible cause(s) of death in our victim and PMCT findings.
Because our victim ran out of air at some point during ascent, PBT is a possibility. In accordance with Boyle’s law, intrapulmonary air will expand with ascent and cause alveolar wall stress and eventual rupture if it is not sufficiently exhaled. 6 Running out of air is a risk factor for PBT due to breath-holding and may have occurred in our victim while ascending. However, running out of air and breath-holding are both most commonly seen in inexperienced divers and it is noteworthy that our victim was highly experienced.
When the alveolar-capillary membrane is breached, air is free to track back along the perivascular sheaths and can result in pneumomediastinum, pneumopericardium, pneumoretroperitoneum, and subcutaneous emphysema. 7 Our PMCT demonstrates a large pneumomediastinum and small pneumopericardium. Moreover, focal lung pathology is evident with a small, right-sided hemothorax and may be secondary to a pneumothorax, which complicates 10% of PBT cases (although the effects of CPR cannot be excluded either). 8 Clinically, our patient was also noted to have copious amounts of blood in his upper airway and massive pulmonary hemorrhage is a recognized, albeit rare, complication of PBT 3 (again, the effects of CPR cannot be excluded). However, the extensive whole-body subcutaneous emphysema observed is unlikely to be related to PBT, which is usually limited to the head and neck (see below).
The most dangerous complication of PBT is AGE. This occurs within seconds to minutes after surfacing from a dive when alveolar air enters the pulmonary circulation. 3 Antegrade pneumatization of these vessels can result in left-sided pneumocardium and systemic air embolization (eg, cerebral arterial gas embolism), although there was no focal neurology to suggest this in our victim. Laurent et al found that the most specific marker for PBT was complete pneumatization of the supra-aortic vessels (if PMCT is performed within 24 hours), 5 features evident in our case. Retrograde pneumatization of the pulmonary capillaries may also occur, where alveolar air presumably tracks down the pulmonary artery and into the right heart. 7 Systemic gas emboli can also filter from the arterial system to the venous bed, right heart, and pulmonary artery.
The majority of victims of AGE survive but around 5% develop apnea, unconsciousness, and cardiac arrest on surfacing. 9 They are usually unresponsive to CPR, even when instituted immediately at the time of collapse, 10 as was the case with our victim.
Theories regarding the mechanism of death in such circumstances have previously centered around the effects of gas emboli on the brainstem or myocardium causing fatal arrhythmias 3 because 50% of fatal victims of AGE die on, or shortly after, surfacing. 11 However, animal studies, where air was injected directly into the cerebral circulation, demonstrate that cardiac arrest does not occur acutely and that lethal arrhythmias only occur after a period of prolonged cardiorespiratory collapse. 12 The same holds true for similar models investigating the effects of air emboli on the myocardium 13 and also in case reports detailing iatrogenic air embolization of the coronary arteries during coronary angiography. 14
The use of both chest radiographs and PMCT yield important clues that might better explain why PBT victims die suddenly upon surfacing. Several case reports and case series have previously demonstrated massive amounts of air in the central arterial and venous circulation,15,16 and these authors believed that obstruction of the central circulation was either causative or played a significant role in the mechanism of death.
Rapid accumulation of air within the central venous system will result in an “airlock” of the pulmonary arteries causing acute right ventricular outflow tract obstruction, increased pulmonary artery pressure, and right ventricular strain. 17 The increased resistance to right ventricular outflow results in diminished pulmonary venous return, which decreases left ventricular preload and cardiac output and is followed quickly by cardiogenic collapse. 18 However, although it is true that occasionally there can be retrograde transmission of intrapulmonary gas into the pulmonary arteries as a result of PBT, it is not usually in sufficient quantity to cause this scenario, which is more likely to occur after massive omitted decompression and cardiopulmonary DCS. The latter, however, is extremely rare in recreational diving and unlikely to have played a significant role here. The possibility that AGE caused gas in both the systemic and pulmonary arteries is also undermined by the fact that there appears to be no gas in the pulmonary veins in Figure 1. Also, although the deceased may have shown many clinical features of PBT, this diagnosis does not explain the extensive subcutaneous emphysema that was observed. Nor is the presence of large volumes of gas in the central circulation necessarily indicative of the cause of death and may simply be an artefact, such as PMDA.
It is also worth noting that the left ventricle appears to be hypertrophied and the lungs are congested. This may point to a potential cardiac event (eg, myocardial infarction or arrhythmia) as the root cause of the fatal sequence of events. It might also explain why he ran out of air, perhaps being tachypneic well before he started to ascend. Of course, other factors implicated with running out of air cannot be fully excluded (such as swimming against a tide or being out of condition) or other causes, such as immersion pulmonary edema (which may be more underdiagnosed than rare)—although these patients may become breathless while still at depth, which does not appear to have been the case here.
Divers who die soon after surfacing from deep and/or long dives are at risk of developing PMDA because their tissues and blood still contain substantial quantities of dissolved inert gases. Once circulatory collapse occurs these gases, which are usually exhaled in the living subject, accumulate in the vessels and tissues because they cannot escape. This occurs particularly within the venous system and can also result in extensive subcutaneous emphysema. 2
Experiments on animals exposed premortem to recreational diving conditions and then scanned after death demonstrate that PMDA begins gradually, initially intravenously from the first hour postmortem, which then spreads to the arterial system after 2 to 3 hours and is very obvious by 8 hours.19,20 Therefore, at 100 minutes postmortem, our PMCT is potentially liable to the effects of PMDA, largely on the venous side. Also, some authors advocate performing a whole-body PMCT as soon as possible after death in order to demonstrate gas in the intramuscular fascial layers, which is relatively specific for PMDA and not acute DCS, providing putrefaction gases are excluded. 2 Unfortunately, we only scanned the thorax and abdomen due to lack of awareness of this feature. Thus, in this case, given the victim’s recent dive history and circulatory collapse shortly after surfacing it is likely that much of the gas seen on PMCT will have been as a result of PMDA.
Putrefaction gases are unlikely to be a factor here as they usually appear from 3 to 6 hours postmortem. 20 Other sources of extraneous air, such as resuscitation artefacts—which usually affect the venous system or cause localized subcutaneous emphysema—do not normally replicate the large volumes and wide distribution of air seen in our victim. 2 However, it is possible that gaseous gastric distension (eg, from resuscitation) can cause gas to enter the portal venous system 21 (as evident in our case). This gas can then track to the systemic venous system and move to the systemic arterial system in the presence of an atrial septal defect, for example. Although there is no proof of an atrial septal defect in our patient, it is worth noting that in Figure 1 there appears to be no interatrial septum (which simply might be attributable to poor definition of a thin septum). In that situation, the gas seen in the central circulation would be entirely postarrest (and the cause of arrest would then be attributable to another problem, such as an acute cardiac event).
Conclusion
This case report highlights the potential challenges in determining the underlying mechanism of death in victims of fatal diving accidents. However, what is clear is that these individuals should have a whole-body CT scan followed by an autopsy by a suitably qualified pathologist, if available, and that both should be performed as soon as possible to minimize the effects of artefacts. On balance, the cause of death in our case is possibly due to an acute cardiac event, followed by PBT, and then DCS. Also, the effects of PMDA need to be considered, particularly with regard to the findings on the PMCT. Running out of air (without other mitigating circumstances) would be unusual in such an experienced diver, as would surfacing with a closed glottis. Ultimately, it will remain a mystery what precipitated the fatal spiral of events in this case.
Acknowledgments: The authors thank Ms Haruko Obara for her kind assistance communicating with the relevant parties in Japan.
Author Contributions: SD: data collection, project conception, manuscript drafting, critical revision, and approval of final version; MK: manuscript drafting, critical revision, and approval of final version; MA: manuscript drafting, critical revision, and approval of final version; VZ: manuscript drafting, critical revision, and approval of final version; JF: manuscript drafting, critical revision, and approval of final version.
Disclosures: None.
Financial/Material Support: None.
Footnotes
Submitted for publication September 2016.
Accepted for publication March 2017.