
Abstract
Objective
The purpose of this study was to evaluate 2 ruggedized field intravenous (IV) systems currently in use by US military medics and to determine their effect on fluid bolus administration rates.
Methods
A series of 500 mL fluid boluses consisting of either Lactated Ringer’s solution or Hextend were delivered to 2 artificial intravenous training arms using a standard 18G catheter (control) and 2 separate ruggedized field IV systems. Fluid boluses were delivered under both gravity force and pressure infusion (constant 300 mm Hg), and total bolus times were recorded.
Results
Using Lactated Ringer’s solution, the standard IV system took a mean time of 9:33 minutes (95% CI: 9:13–9:54) to deliver a 500 mL fluid bolus whereas the 2 ruggedized field systems took mean times of 14:50 minutes (95% CI: 14:00–15:40) and 12:20 minutes (95% CI: 11:54–12:45). Using Hextend, the mean bolus time for the control system was 24:39 minutes (95% CI: 22:47–26:32). The 2 ruggedized field systems required an average of 49:32 minutes (95% CI: 48:07–50:58) and 39:46 minutes (95% CI: 37:30–42:01) to deliver an equivalent bolus. Pressure infusion significantly increased flow rate in all systems.
Conclusions
Ruggedized field IV systems can significantly delay fluid bolus rates. In instances where ruggedized field systems are deemed necessary, pressure infusion devices should be considered to overcome the constrictive effects of the ruggedized system.
Keywords
Introduction
Under current tactical combat casualty care (TCCC) guidelines, the rapid delivery of fluid bolus challenges is a cornerstone of resuscitation for the hypovolemic trauma patient in the tactical and austere environment. Recommendations for the treatment of casualties who have massive hemorrhage and are displaying signs of shock include a 500 mL bolus of Hextend (6% hetastarch in lactated electrolyte injection) delivered as quickly as possible.1,2 Moreover, rapid fluid bolus administration within the tactical and austere medical arena is not simply limited to instances of massive hemorrhage. Entrapped crush-injured patients can require large volumes of crystalloid fluid over short periods, often before extrication.2,3 In instances when rapid fluid administration is required, a significant rate-limiting factor is often the junction between patient and the administration line: the catheter. Although civilian recommendations typically involve the initiation of 1 or more 14G to 16G catheters for trauma resuscitation, smaller 18G catheters are favored in the tactical and field settings because of their higher rate of successful placement.
To prevent accidental dislodgement of intravenous catheters during transport, 2 variants of ruggedized field IV systems, or “Ranger IVs” (so called because of their development by the US Army Rangers), have become increasingly common in the past several years (Figures 1 and 2). Whereas traditional IV systems involve connecting the fluid administration line directly to the peripheral catheter hub, these ruggedized field systems involve first connecting a pro re nata (PRN) adapter to the catheter and then covering the catheter and PRN adapter with a transparent dressing, creating a saline lock. The next step is what differentiates the 2 variants of ruggedized field systems. Variant 1, currently taught to US military Special Operations combat medics, requires that the IV administration line be connected to an 18G hard needle and that the needle be inserted into the saline lock (Figure 1). 4 Variant 2, the type more commonly found in medical references, requires that a second 18G catheter be inserted into the saline lock and that the IV administration line be connected to this secondary catheter (Figure 2).1,5
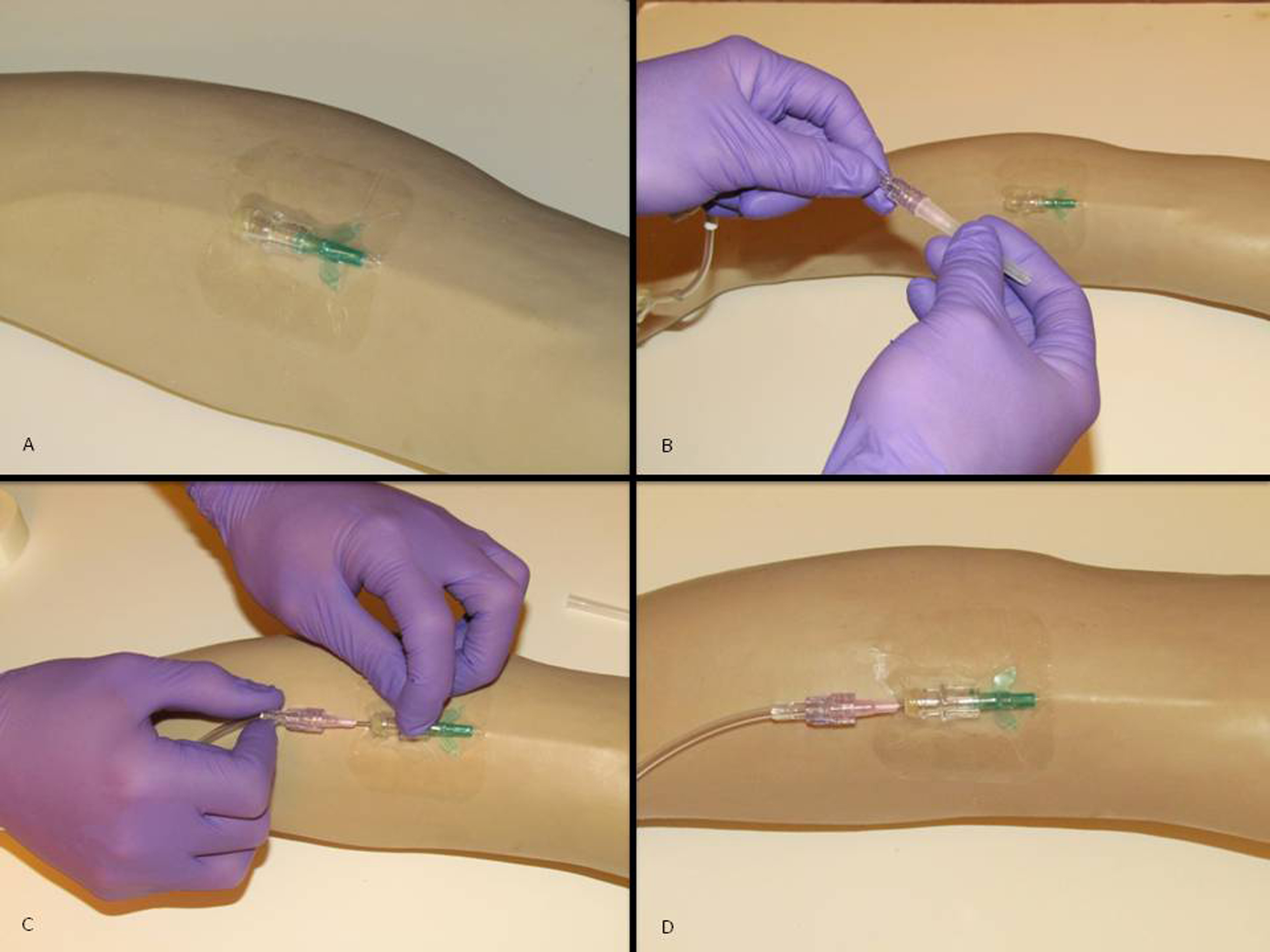
Steps for initiating a ruggedized field IV variant 1: (A) A peripheral 18G IV catheter and saline lock are established and covered with a transparent dressing; (B) an 18G hard needle is connected to the administration line; (C) the hard needle is inserted through the transparent dressing into the saline lock; and (D) the completed system.
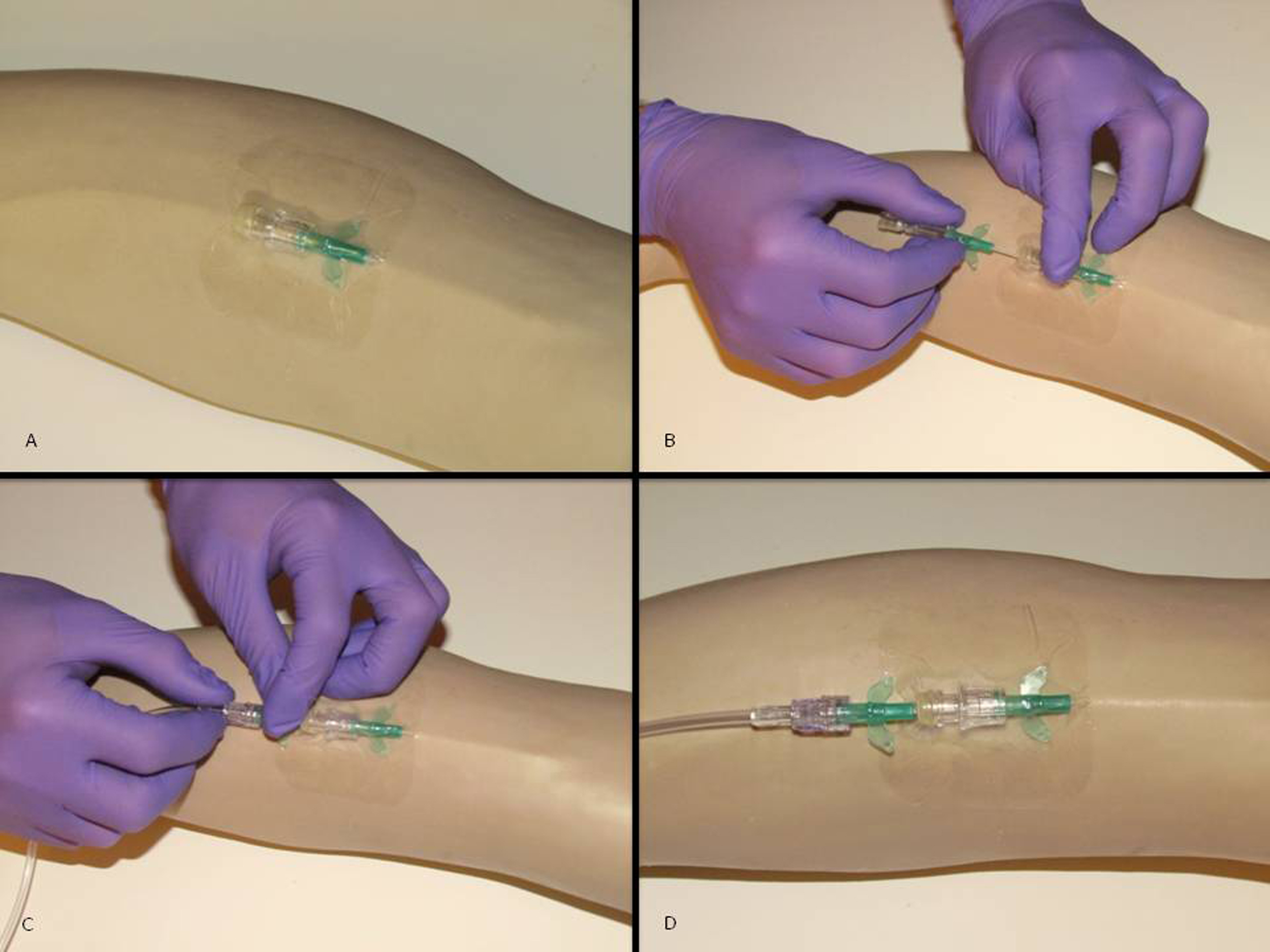
Steps for initiating a ruggedized field IV variant 2: (A) A peripheral 18G IV catheter and saline lock are established and covered with a transparent dressing; (B) a second 18G catheter is inserted through the transparent dressing and the needle is removed; (C) the administration line is connected to the second 18G catheter; and (D) the completed system.
Both of these field ruggedized systems allow for 2 advantages over a standard IV system. First, they provide for the most efficient use of supplies in low resource environments. The initial saline lock provides critical vascular access without committing limited fluids to a patient who may not require volume resuscitation. Second, when used to deliver IV fluid, they prevent accidental catheter dislodgment and the loss of IV access. If the IV line were to become snagged or placed under sudden tension, the secondary catheter or hard needle inserted into the PRN adapter would simply be pulled out, leaving the original saline lock in place and thus preserving IV access. Although these ruggedized field systems have the obvious benefit of preventing accidental loss of IV access and minimizing waste in resource-critical environments, they also limit fluid flow rate under circumstances in which rapid administration is the goal. This paper attempts to determine what impact the use of ruggedized field IV systems has on the rate of fluid bolus administration.
Methods
A series of 500 mL fluid boluses were administered to 2 IV catheterization training arms (Life-form Injectable Training Arm LF00698, Nasco, Fort Atkinson, WI) using the systems described in the following text. Both training arms were set up identically.
Standard IV, Control
The arms were cannulated in identical locations with 18G 1.25-inch (Introcan safety winged-FEP, B Braun, Melsungen, Germany) peripheral venous catheters. Fluid administration sets (IV administration set with universal spike and spin-lock connector, B-Series set, 15 drops per mL, B Braun Medical, Bethlehem, PA) were connected directly to the catheters.
Ruggedized Field (Ranger) IV, Variant 1
The administration set was removed from the existing peripheral catheter and a PRN adapter was connected (Baxter interlink injection site 2N3379, Baxter Healthcare Corp, Deerfield, IL) (Figure 1). An 18G hard needle (PrecisionGlide needle, Becton Dickinson, Franklin Lakes, NJ) was inserted into the saline lock, and the administration set was then connected to the hard needle.
Ruggedized Field (Ranger) IV, Variant 2
The 18G hard needle was removed from the saline lock and replaced with an 18G catheter (Introcan safety winged-FEP, B Braun, Melsungen, Germany) (Figure 2). The administration line was connected to this secondary 18G catheter.
All 3 systems were evaluated using both gravity-fed and pressure-infused fluid delivery. For the gravity-fed system, the fluid was hung from a standard collapsible IV pole designed for use with a military folding litter (adjustable IV pole, North American Rescue), creating a vertical distance of 46 cm from the bottom of the fluid bag to the catheter insertion site. Pressure infusion was accomplished using a disposable commercial pressure-infusion device (Infu-Surg disposable pressure infuser bag, Ethox International, Buffalo, NY) inflated at a constant pressure of 300 mm Hg. The pressure infusion bag was also hung from the collapsible IV pole, creating a vertical distance of 46 cm from the bottom of the bag to the catheter insertion site. Each system was evaluated using 10 500-mL bags of Lactated Ringer’s solution (Baxter Healthcare, Deerfield, IL) and 5 500-mL bags of Hextend (6% hetastarch in lactated electrolyte injection, Hospira, Lake Forest, IL). Fewer Hextend boluses were used because of the colloid’s increased cost and because of the narrow range of observed bolus times. In all Lactated Ringer’s trials, 5 fluid boluses were delivered through each arm, whereas in the Hextend trials, 2 boluses were delivered through the one arm and 3 were delivered through the other.
Analysis of variance testing was used to compare bolus times between both Ranger variants and control IV systems. Student’s t test was used to compare pressurized and gravity force for each system with both Lactated Ringer’s solution and Hextend. All calculations were performed using Microsoft Excel (Microsoft Corporation, Redmond, WA).
Results
Bolus times for all 3 systems are shown in the Table. Analysis of variance testing demonstrated significant differences in the bolus times of IV systems within all 4 groups (Lactated Ringer’s gravity fed, Lactated Ringer’s pressure infused, Hextend gravity fed, and Hextend pressure infused). A Bonferroni correction showed that both Ranger IV variants had significantly longer bolus times than the control groups, and that variant 1 was associated with longer bolus times than variant 2 (P < .001 in all instances). On average, Lactated Ringer’s solution flowing under gravity pressure through the variant 1 and variant 2 ruggedized field systems took 55% and 29% longer than the control, respectively, to deliver a 500 mL bolus. Using the more viscous colloid fluid, the flow restrictive characteristic of the ruggedized field systems was even further magnified.
Bolus times for all 3 systems
All times listed as minutes:seconds.
Student’s t test for comparison of pressure infused vs gravity fed, P < .001 in all instances.
Analysis of variance with Bonferroni correction for systems within each group, P < .001 in all instances.
Student’s t test was used to compare pressure infusion and gravity force in all 3 IV systems and with both Lactated Ringer’s and Hextend. In each instance, gravity-fed systems were paired with their pressure-infused counterpart. In this analysis, pressure infusion was universally shown to produce significantly shorter bolus times (P < .001). Under pressure infusion, all 3 IV systems were able to deliver a bolus of Ringer’s Lactate in less than 5 minutes and a bolus of Hextend in less than 10 minutes (Table).
No differences were observed in bolus times between the 2 training arms.
Discussion
The data collected demonstrate that using a ruggedized field IV system can have a significant impact on the overall time required to administer a fluid bolus challenge. The rate-limiting effects of these IV systems are most profound when using Hextend and, theoretically, other equally viscous colloid fluids (Hetastarch solutions have a viscosity of approximately 7 times that of water 6 ). This finding is troubling because Hextend, in the tactical and austere environment, is typically reserved for the hypovolemic trauma patient who is most in need of rapid fluid resuscitation. 1 ,2, 7 Under gravity pressure alone, the mean times required to deliver a 500 mL bolus of Hextend using the 2 varieties of ruggedized field systems were 49:32 minutes and 39:46 minutes. This is arguably too slow to effectively resuscitate, or determine fluid responsiveness, in a patient showing signs of shock secondary to massive hemorrhage. When faced with critically ill trauma patients requiring rapid boluses of colloid solutions, and in the absence of pressure infusion devices, providers in the field might be best advised to utilize traditional IV systems and maintain a high level of vigilance to prevent accidental dislodgment.
If operational conditions pose a high risk of accidental dislodgement (eg, difficult extrication or movement over rough terrain) and a ruggedized field system is deemed absolutely necessary to avoid loss of vascular access, the above findings support the use of the second variant of ruggedized field IV (a second 18G catheter inserted into the saline lock rather than the hard needle as in variant 1). Although this variant of the ruggedized field IV system still causes a significant reduction in the total bolus delivery time as compared with the traditional IV system, it does offer an increased flow rate over the ruggedized field IV variant 1 (P < .001) (Table). Additionally, the second variant is potentially safer in the event of an accidental dislodgment of the IV in that it does not pose the threat of an unsecured sharp needle resulting in an accidental needlestick.
The results observed in this study can be quantified by the Hagen-Poiseulle equation, which states that small changes in the radius of a pipe can have a dramatic effect on resistance to flow (inversely proportional to the change in radius to the fourth power). That is demonstrated in the differences between the use of the 18G catheter and the hard needle, wherein the slightly smaller internal diameter of the hard needle (the average internal diameter of an 18G hard needle is 0.0330 inches, whereas the average internal diameter of an 18G catheter is 0.0370 inches8,9) caused a significant decrease in the overall flow rate. Continuing this line of reasoning, it would certainly appear that the use of larger (14G–16G) catheters in the second variant of the field ruggedized system would allow for even faster flow rates. Unfortunately, these larger catheters tend to collapse under the circumferential elastic pressure of the PRN adapter, resulting in unreliable and severely constricted flow.
Perhaps the most noteworthy feature of the data collected relates to the role of pressure infusion using both the traditional and ruggedized field IV systems. Although the relative differences in fluid bolus administration times remained fairly constant between the standard and the ruggedized field systems, the use of pressure infusion significantly increased overall flow rate. Under pressure infusion, all 3 IV systems were able to deliver a 500 mL bolus of Hextend in less than 10 minutes. By incorporating an inflatable pressure infuser with either variety of Ranger IV system, providers in the field are able to deliver rapid fluid bolus challenges while limiting the potential for accidental dislodgement of critical IV access sites. Providers should keep in mind that although there are field-expedient methods for pressurizing IV bags to increase flow rate (squeezing the bag, using blood pressure cuffs, and so forth), previous papers have shown these methods to be inferior to commercial inflatable devices.10,11 These inflatable pressure infusers are lightweight, inexpensive, simple to operate, and durable enough to survive field use. Given the significant advantage that these devices provide in administering rapid fluid resuscitation, they should most likely serve as standard equipment for anyone planning to treat trauma patients in the austere environment. Moreover, with the ever-increasing role of intraosseous devices in the treatment of both combat and prehospital patients, these pressure infusion systems should be nearly ubiquitous in the inventory of medics and remote medical providers. Considering the dramatic effect that pressure infusion is shown to have on both field ruggedized and standard IV systems, these devices should not be limited to use with intraosseous systems, but rather to all instances in which rapid fluid resuscitation is required.
Study LIMITATIONS
To maximize uniformity, artificial training arms were used to conduct this study rather than live patients. Owing to the variable flow rates encountered when obtaining IV access in humans, bolus times administered to patients could differ from those obtained during the conduct of this trial.
Conclusions
Ruggedized field IV systems, currently in use by US military medics, can offer significant advantages to tactical and remote medical providers by providing IV access without committing limited fluid resources and by reducing the potential of accidental catheter displacement. These advantages lend themselves particularly well to the arena of wilderness medicine, where supply is often limited to what can be carried by the provider, and difficult patient transport can wreak havoc on IV access sites. Unfortunately, these systems also have the drawback of limiting flow rate, especially when viscous colloid solutions are being used. If operational conditions require the use of a ruggedized field IV system, it is recommended that variant 2 (a second 18G catheter inserted into the saline lock, as shown in Figure 2) be used and that a commercial pressure infusion device be incorporated to maximize fluid delivery.
Footnotes
Acknowledgment
The author would like to thank the Joint Special Operations Medical Training Center for the use of its facilities and resources in the conduct of this trial.
☆
Disclaimer: The views expressed in this article are those of the author and do not reflect the views or opinions of the United States Army, the Department of Defense, or the United States Government.