
Abstract
Objective
The objective of this study was to describe the pediatric emergencies encountered by the Christophorus-1 helicopter emergency medical service (HEMS) during a period of 2 years.
Methods
Emergency treatment of pediatric casualties by HEMS was evaluated at a helicopter base. Children up to 14 years who were treated by HEMS emergency physicians from Christophorus-1 during primary missions in the alpine region were retrospectively enrolled.
Results
Of the 1314 HEMS operations conducted during a 2-year investigation period, pediatric emergencies accounted for 114 (8.7%). Trauma was the most common emergency indication (91.3%) in alpine areas, and 77.5% of the indications were related to skiing and snowboarding; 11.3% of the prehospital pediatric emergencies were classified as life-threatening. Interventions on site were rendered in 46.3% of cases. Mean and SD intervals for approach were 11.0 ± 3.0 minutes; for treatment, 14.0 ± 6.0 minutes; and for transport, 8.0 ± 4.0 minutes. Intervals on site were significantly longer whenever it was necessary to search for an interim landing place (P < .001) or perform rope extrication (P < .001). Aggravating environmental conditions such as low temperature (78.8%), rocky terrain (18.8%), or precipitation (12.5%) were common.
Conclusions
Rapid procedures are preferred to sustained on-scene treatment, particularly when surrounding conditions are hostile. HEMS emergency physicians attempt to keep on-site intervals short and treatment and monitoring to the essential to minimize delay in rescue.
Introduction
With more and more locations for leisure time events, the number of pediatric emergencies occurring during leisure activities is increasing. 1 In remote alpine regions helicopter-based emergency medical services (HEMS) hold a special position in providing access to rapid high-quality health care. Expert emergency care and direct referral to the trauma center are associated with reduced 2-week mortality in severe trauma2,3 and may eliminate the need for secondary transfer of patients. 4 Furthermore, nondelayed extrication of patients from wilderness regions gains special importance as even mild-to-moderate trauma can become life-threatening under extreme atmospheric conditions. 5
Pediatric emergencies frequently represent a challenge for emergency physicians, with high expectations and pressure to succeed in an atmosphere of strong emotions. 6 At the same time, sufficient experience with pediatric emergencies is difficult to obtain as the average rate of emergency treatment in routine duties is low. 7 In remote areas and at high altitude, further difficulties may arise from topographic and weather conditions, calling for individual and pragmatic solutions. This does not substitute for regular training of pediatric algorithms. Emergency techniques adjusted to the specific requirements of HEMS in the mountainous regions are important. 8
The objective of this study was to describe the pediatric emergencies encountered by the Christophorus-1 HEMS during a period of 2 years.
Patients and Methods
Rescue System
Christophorus-1 in Innsbruck, Austria, has provided HEMS since July 1983. The operation area is around 10,000 km 2 within a maximum diameter of 150 km. Of the 450-km 2 core catchment area, 16% is less than 800 m altitude and is where most of the population lives. Within 15 minutes, the double-engine Eurocopter EC 135 can reach 9 different hospitals: 5 in Austria, 1 in Italy, and 3 in Germany. The crew consists of a pilot, a rescue technician, and an emergency physician. 9 Rope extrications are performed with a specially developed double-hook system located centrally on the helicopter to avoid additional weight for a winch and a winch operator. The emergency physician and rescue technician are transported as near as possible to the patient. In steep and rocky terrain, they either get off the hovering helicopter or are transported to the scene by rope. In this case, the pilot searches for a small area suitable as an interim landing place for the helicopter so the rope can be attached to the double-hook system. Duty hours differ day by day between dawn and nightfall. 8 With 15 emergency helicopter bases during the winter season, Tyrol offers the highest density of HEMS in Europe. 9
Study Design
Between January 2012 and December 2013, children up to 14 years who were treated by HEMS emergency physicians from Christophorus-1 during primary missions in the alpine region were retrospectively enrolled. Secondary missions, eg, interhospital transport of neonates from a peripheral hospital to the center, were not included. Data were collected from record charts filed at the HEMS base in Innsbruck, Austria. The retrospective study was approved by the ethics committee of Innsbruck Medical University (AN 2014-0069 334/4.25). Alpine region was defined as being at an altitude exceeding 800 m above sea level. 8 Rescue intervals comprise approach interval (time from alarm to arrival on scene), treatment interval (time on site), and transport interval (time from departure to arrival in the hospital). For the sake of comparability of pediatric emergencies in the catchment area, the definitions of age groups follow the categories used by Nagele and Kroesen. 10 Five age groups include neonate (<1 month), baby (1–12 months), toddler (1–4 years), preschool (4–6 years), and school age (6–14 years). 10 Neurologic status was assessed using the Glasgow Coma Scale (GCS). In infants and young children the pediatric version of the GCS was applied. 11 Scores were evaluated in 3 groups (15, 9–14, and ≤8).
Pain status was estimated and documented in 3 categories as slight, moderate, or severe in consideration of overall condition and signs and symptoms observed (Figure 1). Whenever practicable, HEMS physicians asked for character and intensity of pain according to a numerical rating scale (none to slight, 0–2; moderate, 3–6; and severe, 7–10). 11
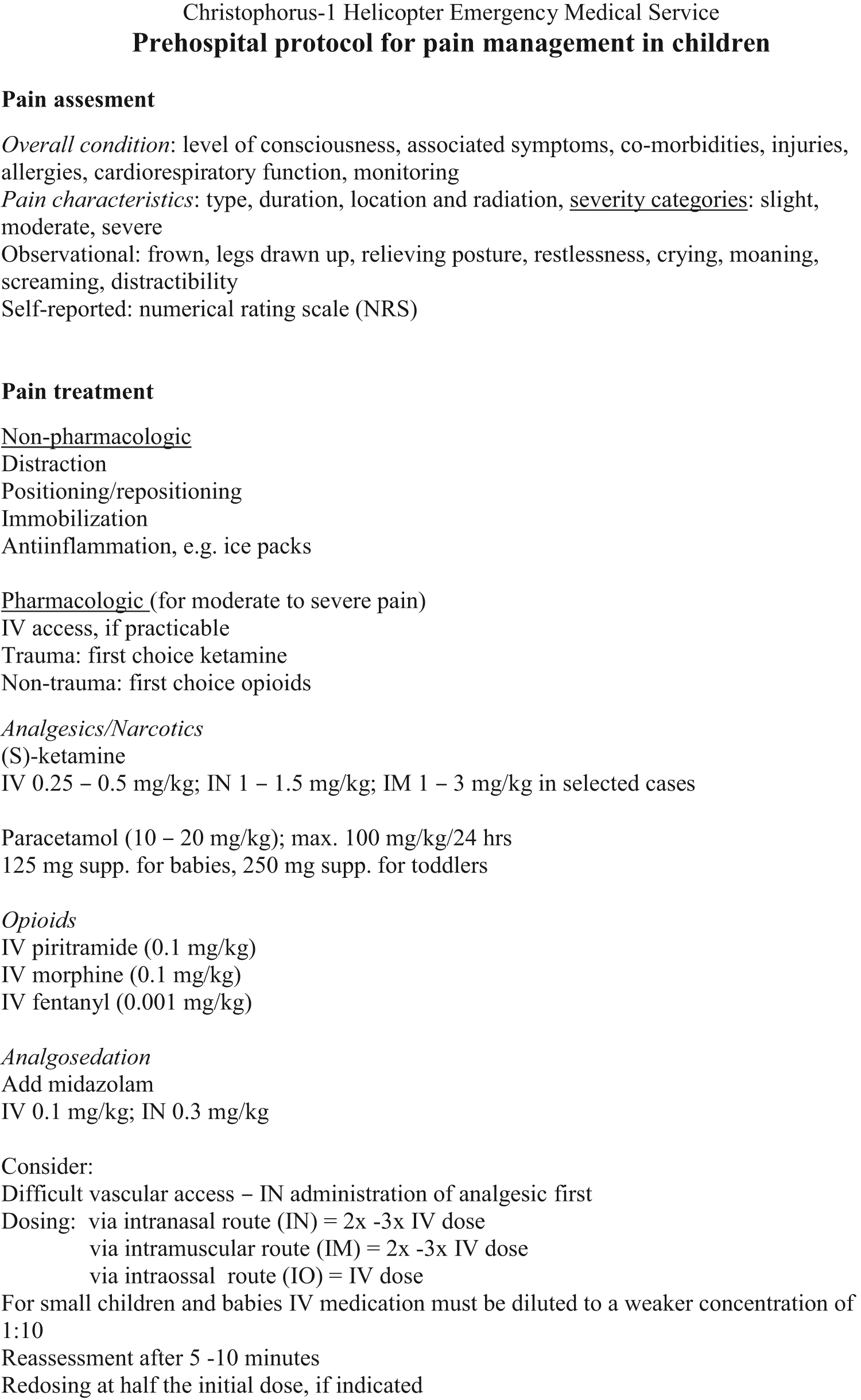
Prehospital protocol for pain management in children. IM, intramuscular; IN, intranasal; IO, intraossal.
Severity of impairment by disease or injury was rated using the scale of the National Advisory Committee for Aeronautics (NACA: 1, minor, no transport; 2, moderate, outpatient management; 3, serious, hospital admission; 4, severe, potentially life-threatening; 5, severe, immediately life-threatening; 6, critical, survival uncertain; 7, death).
Supplementary information and mission details on location (temperature, altitude), obstacles (eg, rocky terrain requiring rope extrication and a search for a landing place), and weather conditions (precipitation, strong wind, fog) were evaluated.
Statistical Analysis
For descriptive analysis of frequencies we used SPSS version 22.0 (IBM SPSS Statistics, IBM Corp, Armonk, NY). Data are presented as frequencies (number and percentage) and mean±SD as appropriate. Student’s t test was used for comparison of means in independent samples when data were normally distributed. Nonparametric analysis was made with Mann-Whitney U test. A probability value of less than .05 was deemed significant.
Results
Of 1314 primary missions, 114 (8.7%) were pediatric cases, 80 (70.2%) of which occurred in the alpine region. Most children (90.0%) were of school age; the male-to-female ratio was 1.3:1 (Table 1). There was a seasonal peak in frequency between December and March, when 73.8% of pediatric emergencies occurred (Figure 2). Diurnal frequency of emergencies accumulated before noon (1100–1200) and in late afternoon (1500–1700). Trauma was the underlying reason for HEMS treatment in the majority (91.3%) of pediatric cases. The majority of injuries occurred when skiing or snowboarding (Table 2). Life-threatening conditions on site were diagnosed in 11.3% of emergencies (Table 2). Mean GCS score and SD were 14.7 ± 0.8. Interventions were performed in 46.3% of cases; in 45.0% an IV access was established (Table 3). One third (28.8%) of the children received analgesic treatment, most commonly ketamine (69.6%) administered IV or via the nasal mucosa, and piritramide (52.2%) given IV. Monitoring was established in 56.3% of cases, most frequently by pulse oximetry (86.7%). Oxygen by mask was given in 6.2% of cases; tracheal intubation on site was not reported during the investigation period.
Demographic and patient characteristics in 80 pediatric emergency cases
GCS, Glasgow Coma Scale; VAS, Visual Analog Scale.
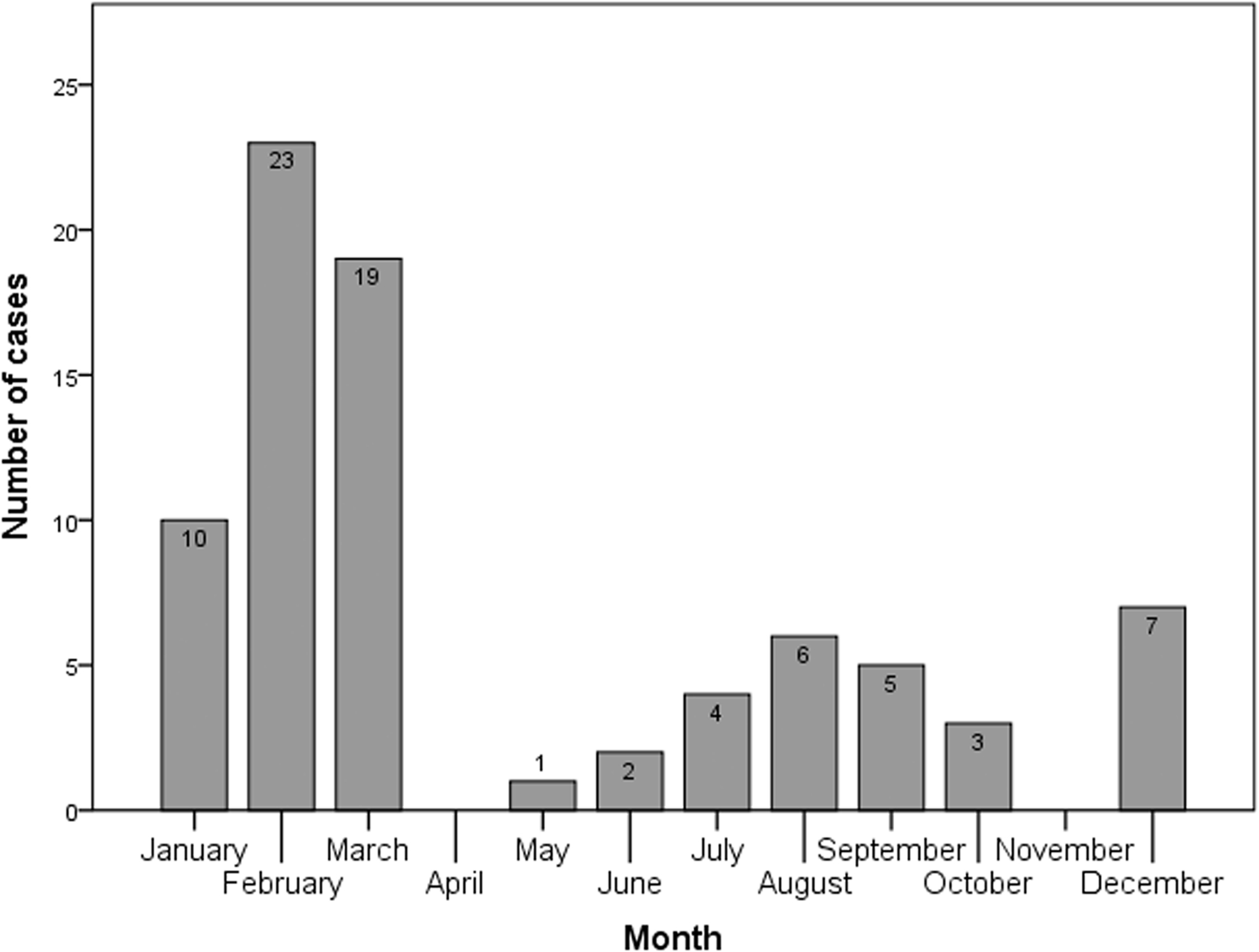
Seasonal distribution of pediatric emergencies treated by helicopter-based emergency medical services during a 2-year observation period.
Distribution of national advisory committee for aeronautics (NACA) scores in 80 pediatric emergency cases according to etiology and activities
Interventions during alpine rescue in 80 pediatric emergency cases
Most (68.8%) operations were performed at altitudes between 1500 and 2500 m at temperatures between 0°C and 10°C (60.0%). Mean approach interval was less than 14 minutes, mean treatment interval was less than 20 minutes, and mean transport interval was less than 12 minutes in the vast majority of missions (Table 4). Intervals were significantly longer in missions conducted under aggravated conditions such as having to search for a landing place (P < .001) or having to perform a rope extrication (P < .001). Of the treated children, 93.8% were admitted to hospital, half (54.7%) of whom were transported to Innsbruck Medical University Hospital.
Atmospheric and geographical conditions and mission intervals during alpine rescue in 80 pediatric emergency cases
Discussion
Pediatric emergencies encountered by the Christophorus-1 HEMS in a European alpine region during a period of 2 years were evaluated. We report for the first time that aggravating environmental conditions, including low temperature, rocky terrain, and precipitation, occur in the majority of cases and thus affect diagnostic and therapeutic maneuvers on site.
Low temperature, as encountered during most interventions, does not permit patients to be disrobed for a physical examination. Hence, the feasibility of on-site monitoring and diagnosis is severely limited. In addition, connection leads between patient and monitor complicate procedures. This particularly applies for rope extrications, although complete monitoring of ventilated patients is technically possible during this procedure. It is to be investigated whether real-time measurement of vital functions obtained from noninvasive sensors can provide better conditions for monitoring during alpine rescue. 12 However, this technology requires at least partial disrobing of warmly dressed patients to place sensors and a blood pressure cuff.
Mean approach intervals in our study are short and reflect the high density of HEMS in Tyrol during the winter season. 13 Treatment intervals are comparable with those reported in other studies dealing with HEMS in mountainous regions, 8 but are shorter than those reported for lowland bases. 14 In addition, Gries et al 14 observed that helicopter treatment times in lowland missions depended on the severity of injuries. Data from our investigation do not confirm this finding. We conclude that HEMS indications in mountainous regions have to be seen in a wider scope. HEMS missions in the mountains are especially challenging, and frequently encountered risk factors that expose flight crew and patients to risk must be outweighed by a tangible benefit for the patient.15,16
Rapid extrication of the patient takes on special importance as even mild-to-moderate trauma can become life-threatening under extreme atmospheric conditions. 5 Furthermore, keeping on-site intervals short helps reduce the potential for complications. It may even contribute to better outcome, especially in patients with multiple or spinal injuries.2,17
The frequency of HEMS missions for pediatric emergencies in our study is comparable with that of other studies in mountainous and lowland regions.8,18 Trauma related to sport and recreational activities is common in school age children.8,19 Trauma frequently occurs during alpine skiing and snowboarding, which are the most popular winter sports. 20 Most skiing resorts are at an altitude of 1500 m to 2500 m, where the majority of HEMS missions were performed. Diurnal accumulation of accidents between 15:00 and 17:00 is frequently related to exhaustion. 21 The double peak pattern of pediatric emergencies reflects the seasonal fluctuation of tourism.
The high number of HEMS missions performed during the winter season is associated with a decrease in estimated average severity of cases. 9 Compared with lowland HEMS bases, the proportion of children with estimated life-threatening conditions is low in our study. 8 ,22,23
Intravenous access was established in cases with severe impairment and whenever administration of analgesics was needed. (S)-ketamine, the nonracemic form of ketamine hydrochloride, is a potent analgesic drug, suitable especially for pediatric emergency patients. With moderate doses and slow administration, it usually does not impair spontaneous ventilation and can be administered noninvasively through the nose. 24
During the investigation period, no tracheal intubation was performed on site. Contrary to lowland missions, this maneuver is rarely performed on alpine missions.8,22 Size and weight of medical equipment is limited, especially during HEMS missions in high altitude.
Equipment must be light, portable (so as to be brought to the patient), and robust. 16 Preliminary assessment of cardiopulmonary function can be rapidly achieved by pulse oximetry. Its simple handling and noninvasive nature made this the most frequently used monitoring tool. 25
As a concept in alpine rescue, HEMS rapid procedures are preferred to sustained, on-scene treatment, in particular when the surrounding conditions are hostile. On-site treatment is minimized to the essentials primarily to facilitate rescue. In HEMS rescue strategy, the nearest suitable hospital is selected for referral. This explains the short transport intervals in our study and why only half of the children were brought to Innsbruck Medical University Hospital.
Limitations
Limitations on our results stem from the short investigation interval that reflects only 2-year seasonal variability in snow and weather conditions. Specific circumstances depending on topography, population, tourism, and regional health services in the catchment area vary among different HEMS centers, thus making generalizations difficult. Third, the number of pediatric cases is too small to allow generalization of mission concepts for HEMS missions in the alpine region. Pain assessment in 3 categories—mild, moderate or severe—depended on the physician’s observation and the feedback from the patient. We are aware that reliable scoring using numerical rating scales will be more accurate in older children. Finally, as data were collected retrospectively from emergency protocols, incomplete documentation of interventions on site cannot be excluded.
Conclusions
Trauma is the most frequent indication for pediatric rescue missions by HEMS in alpine areas. Aggravating environmental conditions are common during most missions. Unless it is necessary to search for an interim landing place or to perform a rope extrication, on-site intervals are kept short. In remote and potentially hostile areas in mountainous regions, HEMS emergency physicians minimize medical performance with only essential treatment and monitoring to not delay rescue.
Author Contributions: Study concept and design (ST, WL, MK, GK); acquisition of the data (ST, WL); analysis of the data (ST, WL); drafting of the manuscript (ST, WL, MK); critical revision of the manuscript (ST, WL, MK, GK); and approval of final manuscript (ST, WL, MK, GK).
Financial/Material Support: Support in the form of equipment for data evaluation, access to scientific literature and writing was provided from the Department of Anaesthesiology and Critical Care Medicine.
Disclosures: None.
Footnotes
Submitted for publication October 2015.
Accepted for publication March 2016.