
Abstract
Objective
Hypobaric hypoxia decreases exercise capacity and causes hypoxic pulmonary vasoconstriction and pulmonary hypertension. The phosphodiesterase-5 inhibitor sildenafil is a pulmonary vasodilator that may improve exercise capacity at altitude. We aimed to determine whether sildenafil improves exercise capacity, measured as maximal oxygen consumption (peak V̇
Methods
The design was a randomized, double-blind, placebo-controlled, crossover study. After baseline cardiopulmonary exercise testing at 1400 m, 12 healthy participants (4 women) aged 60 years or older, who reside permanently at approximately 1400 m and are regularly active in self-propelled mountain recreation above 2000 m, performed maximal cardiopulmonary cycle exercise tests in a hypobaric chamber at a simulated altitude of 2750 m after ingesting sildenafil and after ingesting a placebo.
Results
After placebo, mean peak V̇
Conclusions
Sildenafil (50 mg) did not improve exercise capacity in adults 60 years or older at moderate altitude in our study. This might be explained by a “dosing effect” or insufficiently high altitude.
Introduction
In unacclimatized individuals, ascent to high altitude decreases maximal exercise capacity (maximal oxygen consumption, or peak V̇
The phosphodiesterase-5 inhibitor sildenafil has been shown to be an effective pulmonary vasodilator for treatment of both hypoxia- and nonhypoxia-associated pulmonary hypertension. 8 ,10,11 There is also evidence that, in normal subjects, altitude-induced hypoxemia is attenuated with sildenafil. Previous studies show that sildenafil improves exercise capacity in healthy men and women at high altitudes (4350 m to 5245 m). 5 ,9,12 One possible reason for this exercise limitation is increased right ventricular afterload as a result of hypoxic pulmonary vasoconstriction. However, improvement in gas exchange provides the most likely potential mechanism by which sildenafil improves exercise performance at altitude. 5 ,6,9
Previous studies by Ghofrani et al, 5 Richalet et al, 9 Faoro et al, 12 and Ricart et al 13 show that sildenafil improves exercise capacity, decreases pulmonary vascular resistance, and improves arterial oxygenation. However, these studies examined relatively young (mean ages, 29 to 36 years) healthy subjects under hypoxic circumstances at high altitudes of 4350 m to 5245 m. A question remains about the implications of these studies for older adults who participate in mountain recreation at moderate altitude (approximately 2000 to 3000 m).
The population older than 65 years is increasing worldwide, and this age group is expected to make up 19% of the US population by 2030. 14 Although older individuals may, at times, have greater difficulty in acclimatizing to the rigors of travel, persons older than 60 years comprise an increasing proportion of international travelers. 15 Some references suggest between 15% and 30% of international travelers are now older than 60 years.15,16 In addition, a study as far back as 1997, which examined 1416 US travelers attending a pretravel clinic, found that a full one third of subjects were older than 60 years. 17 Even healthy, athletic older individuals whose lungs undergo the normal aging process face deterioration in pulmonary function and exercise capacity. 18 –23 The potential exercise benefits of sildenafil for this older demographic at a moderate altitude has yet to be elucidated.
The objective of the present study was to investigate whether a 50-mg dose of sildenafil (with dosing based on criteria mentioned in the study design) would increase maximal exercise capacity in persons 60 years or older who reside permanently at approximately 1400 m during acute exposure to a simulated moderate altitude of 2750 m in a hypobaric chamber. We hypothesized that sildenafil would increase peak oxygen consumption at 2750 m in persons 60 years or older.
Methods
Participants
Twelve healthy male (n = 8) and female (n = 4) volunteers 60 years or older (mean age, 66.5 years) were enrolled and gave written informed consent to this study. Subjects were recruited from the local Salt Lake City, UT, mountain club (Wasatch Mountain Club) and from the Salt Lake City area (average elevation, 1400 m). All subjects reported being regularly active in self-propelled mountain recreation at moderate altitudes higher than the altitude at which they live. Subject characteristics are shown in Table 1. No subjects had a history of severe chronic obstructive pulmonary disease as defined by American Thoracic Society criteria, left ventricular ejection fraction of less than 45%, severe pulmonary hypertension with New York Heart Association functional class III or IV symptoms, or a requirement for chronic supplemental oxygen.24,25 No subjects used sildenafil chronically and none were currently using any drugs known to interact with sildenafil (erythromycin, itraconazole, or ketoconazole CYP34A inhibitors). The study was approved by the Intermountain Healthcare institutional review board.
Subject characteristics
Mean values are reported as mean (95% CI).
Values for predicted peak V̇
Study Design
This study used a randomized (block randomization in blocks of 4), double-blind, placebo-controlled, crossover design to examine the effects of 50 mg of sildenafil vs placebo on parameters of pulmonary circulation, arterial oxygenation, and cardiopulmonary exercise capacity. All subjects performed 3 cardiopulmonary exercise tests: 1 baseline test at 1400 m and 2 study tests at simulated altitude (2750 m). This simulated altitude was the maximum for which our institutional review board would give permission under these study conditions. For the 2 exercise tests at simulated altitude, subjects received initial random assignment to either the placebo group (n = 6) or the sildenafil group (n = 6) in a double-blind, crossover fashion (Figure 1). All subjects underwent both placebo and sildenafil treatment at 2750 m. There was a minimum 24-hour washout period between study sessions (maximum elapsed time of 9 days between sessions in the case of 1 subject). Based on the study by Ghofrani et al, 5 12 subjects would be sufficient to detect a significant change (at 80% power with an alpha of 0.05) in cardiac output (CO) and cycle pedal load in watts of the placebo group exposed to 2750 m simulated altitude.
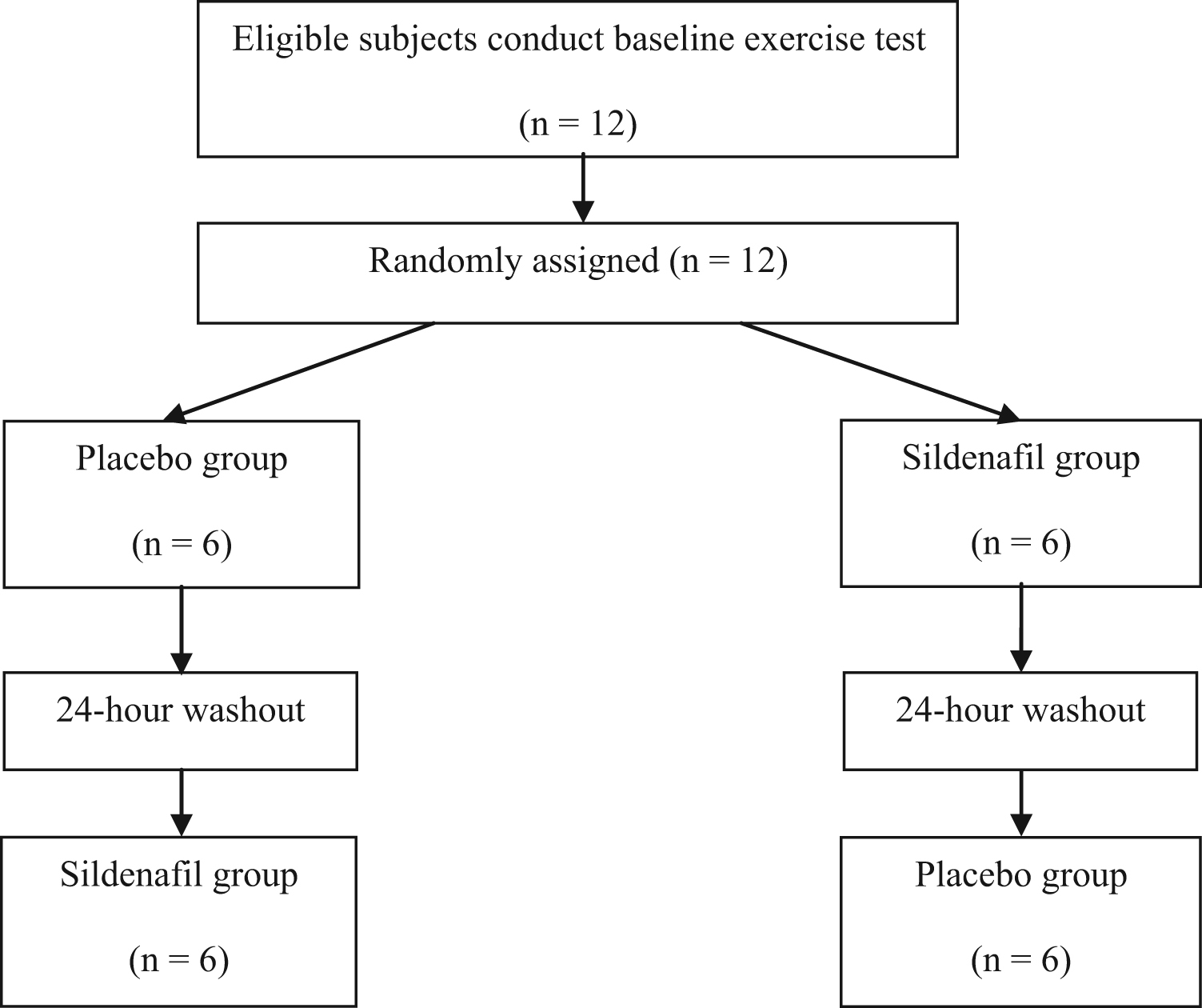
Experimental design. Assignment to placebo and sildenafil groups was by a randomized, double-blind, and crossover design.
The Intermountain Medical Center Research Pharmacy prepared the study drugs as 50-mg, single-dose, orally administered, colorless liquid solutions. We determined that liquid was a preferable form to reduce the likelihood that participants would distinguish between the sildenafil and placebo doses. The dose was selected based on previous studies that have examined the effect of sildenafil on exercise capacity, pulmonary vascular resistance, and arterial oxygenation in hypoxic conditions.5,12
Exercise Testing Protocol
Each subject performed a baseline cardiopulmonary exercise test at 1400 m at The Fitness Institute at LDS Hospital in Salt Lake City, UT. The subsequent 2 exercise tests took place inside a hypobaric chamber (Hypobaric and Hyperbaric Chamber, DL-8, Fink Engineering, Warana, Queensland, Australia) at a simulated altitude of 2750 m (544 ± 1.3 mm Hg) at Intermountain Medical Center in Murray, UT. We selected 2750 m as an appropriate moderate altitude in accordance with previous research. 7 ,26,27 Echocardiography measurements were taken after the subject had spent approximately 30 minutes at rest in the chamber at 2750 m, and cardiopulmonary exercise testing was initiated immediately after echocardiography. In accordance with previous studies, exercise testing began 60 minutes after ingestion of placebo or sildenafil. 5 ,9,28–32
Exercise tests were completed on a non-breath-by-breath cardiopulmonary exercise testing system, the ParvoMedics TrueOne 2400, with an upright, electrically braked, cycle ergometer and a metabolic cart attached to a personal computer (ParvoMedics, Salt Lake City, UT). The TrueOne 2400 has been shown to be an accurate and reliable device for the measurement of inspiratory and expiratory gas exchange variables.
33
During exercise, a tight-fitting mask with a nonrebreathing valve connected to a mixing chamber recorded measurements of minute ventilation (V̇
Because flattening of the V̇
Echocardiography Measurements
A limited transthoracic echocardiographic examination was performed at simulated altitude of 2750 m inside the hypobaric chamber, initially at rest 60 minutes after ingestion of the study drug, and again immediately after exercise while still inside the hypobaric chamber, using a Philips CX50 ultrasound system (Philips, Bothell, WA). We recorded images of the right ventricle using a right ventricle-focused apical 4-chamber view, in accordance with published standards. 39 We measured 2 indices of right ventricular systolic function, the tricuspid annular plane systolic excursion (TAPSE) from m-mode, and the tricuspid annular plane systolic velocity (RV S′), in accordance with published standards. 39 Normal TAPSE is considered greater than 1.6 cm, and normal RV S′ is considered greater than 10 cm/s. The interpreting physician was blinded to the patient’s treatment arm.
Cardiac Output Measurements
We used a noninvasive CO monitor (NICOM) to take continuous measurements of stroke volume and cardiac output during all exercise tests at simulated altitude (Cheetah Medical Systems, Newton, MA). This technology, although typically used in a critical care setting, has been validated in 1 study in which results suggest the NICOM provides face validity for measuring cardiac performance during exercise in patients with heart failure. 40 The NICOM uses bioreactance, or phase shifts in pulsatile flow, to continuously capture hemodynamic signals. It then uses these data to calculate stroke volume index (SVI) and cardiac index.
Statistics
We used a paired Student’s t test to compare peak V̇
Results
A summary of peak exercise values and comparisons of peak V̇
Peak exercise means and comparisons
Values are reported as mean (95% CI).
Peak V̇
Alpha of statistical significance is 0.05.
Value represents Wilcoxon signed-rank test z score.
Cardiac index is calculated as follows: stroke volume × HR/body surface area.
Peak Exercise Values
All participants met criteria for maximal exercise tests in all 3 study sessions (median RER, 1.2, n = 12). Peak V̇
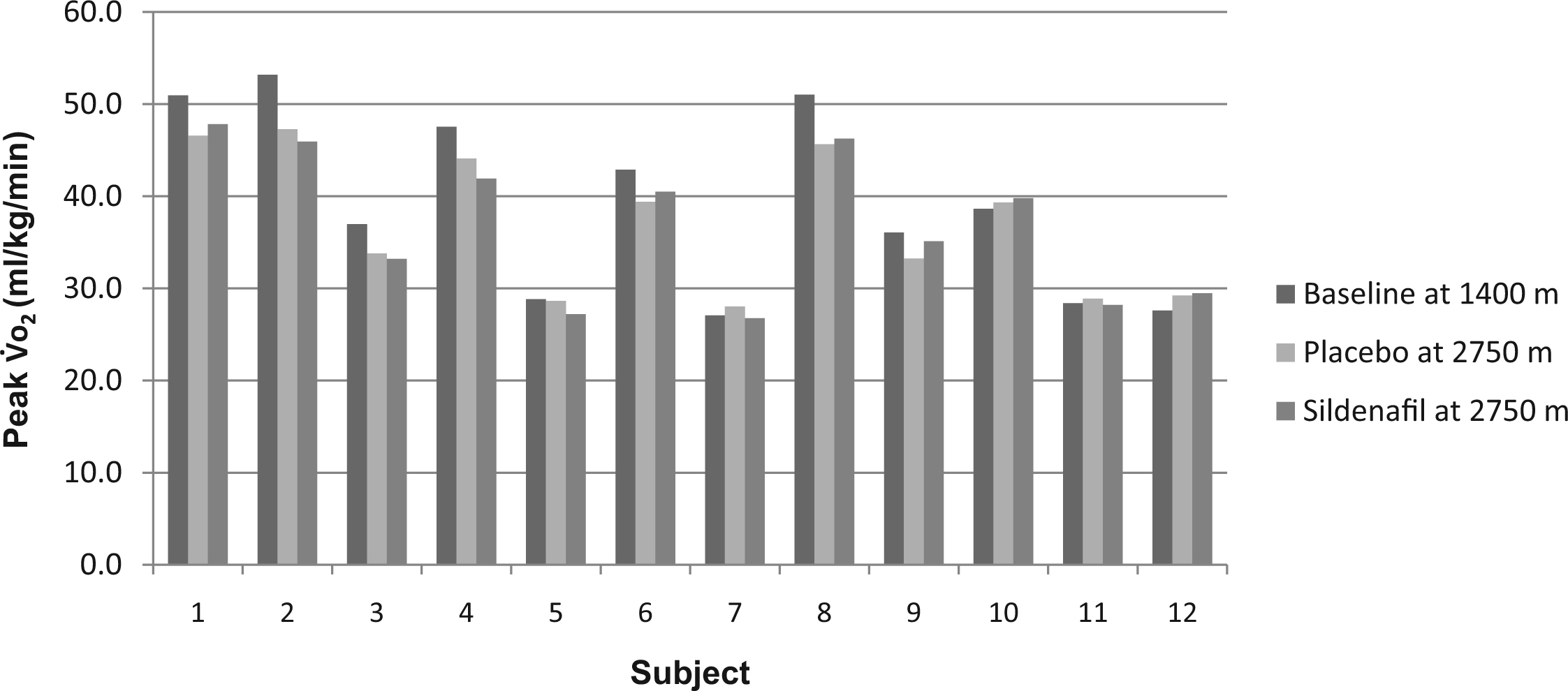
Peak oxygen consumption (V̇
Hemodynamic Measurements
Peak HR, O2 pulse, cardiac index, and SVI at 2750 m were not different after treatment with sildenafil as compared with placebo (P > .05), or between placebo at 2750 m and baseline at 1400 m (P > .05; Table 2).
Echocardiography
Echocardiography assessments conducted immediately after exercise in both 2750 m conditions showed no difference in TAPSE (P > .05). We observed significantly higher RV S′ (P < .05) at 2750 m in the sildenafil condition compared with the placebo condition.
Discussion
Altitude-induced hypoxia reduces peak V̇
At acute moderate altitude, ingesting sildenafil was not associated with an improvement in exercise capacity as compared with after ingesting a placebo. However, previous studies have shown that sildenafil may improve exercise performance in both acute and chronic hypoxia by indirectly improving gas exchange. Ghofrani et al 5 observed improved exercise performance after an approximately 1-week acclimatization trek to Everest base camp (5245 m), whereas Richalet et al 9 found an improvement in exercise capacity over the course of a 6-day stay at 4350 m. In such instances of multiple days of very high altitude exposure, acclimatization starts to become a factor. This may possibly compensate for the decrease in arterial oxygen saturation that occurs on initial ascent. 12
Sildenafil has also been shown to improve peak V̇
Limitations
We believe that the primary limitation was that participants did not experience adequate altitude stress. It is possible that there was not enough hypoxia-induced physiologic response between 1400 m and 2750 m for the drug to have been of benefit in healthy subjects. In particular, for those participants in whom we did not see any significant changes in performance measurements, the altitude change may not have been pronounced enough to generate a normal physiologic response to hypoxia (Figure 2; Table 2). Previous research has shown an effect of sildenafil in a much larger altitude difference between baseline and treatment conditions. 5 ,9,12 Because subjects in the present study live at approximately 1400 m and exercise regularly at altitudes around 2750 m, they may have already been at least partially acclimatized to the study altitude. This could have contributed to the insignificant associations we observed.
Because our institutional review board required that we always perform the baseline exercise study at 1400 m under the direct supervision of a cardiologist as a first test (for screening and safety purposes), we cannot rule out the possibility that an order or learning effect influenced our results. Such an effect may have allowed some subjects to push themselves harder on subsequent V̇
Another possible limitation of this study is that peak V̇
Finally, we cannot rule out a type II statistical error in this study (accepting the null hypothesis when it is in fact false), given the small number of subjects studied. In addition, heterogeneity in fitness, health, and preacclimatization—owing to varying durations of visits to nearby high altitudes by the subjects—may have affected the results.
Conclusions
The main finding of this study was that, during exercise at simulated moderate altitude, we did not observe an association between sildenafil and changes in exercise capacity, as measured by peak V̇
Footnotes
Acknowledgments
This research was supported by a Wilderness Medical Society Hultgren Award.
Dr. Rodway is now with the University of California, Davis School of Nursing, Sacramento, CA.
☆
Presented in part at the Wilderness Medical Society annual summer meeting, July 2013, Breckenridge, CO.