
Abstract
Acute injuries in rock climbing either come from a fall onto the lower leg or from performing a hard move and injuring the upper extremity. Further evaluations of lower leg injuries in rock climbing athletes have been performed recently finding sport characteristics such as peroneal tendon dislocations or chronic deformations of the feet. One injury mechanism described in case reports is the so-called heel hook position, which is used more frequently today compared with the beginngs of rock climbing. In addition, the number of these injuries is expected to rise with the increase in popularity of climbing and bouldering. Therefore, it is important to further analyze this pathology. We investigated 17 patients with injuries of the lower extremities after performing a heel hook.
Introduction
Most acute injuries in climbing either come from a fall onto the lower leg or from performing a hard move and injuring the upper extremity.1,2 Because these injuries on the upper extremity are very sport specific, such as flexor tendon pulley injuries or epiphyseal fractures in the finger joints, most climbing-related scientific studies focus on them. Only recently further evaluations of lower leg injuries have been performed.3,4 Most injuries to the lower leg are acute trauma, such as those that result from falls (eg, fractures and sprains). These happen more often in alpine or traditional climbing than in sport climbing.1,2 Some of these lower extremity injuries exhibit sport characteristics such as peroneal tendon dislocations. 5 One injury mechanism described only in case reports thus far is the so-called heel hook position (Figure 1). 6 -8 These injuries occur mostly in bouldering. Because the number of these injuries is expected to rise with the increase in popularity of climbing and bouldering, it is important to further analyze this pathology.

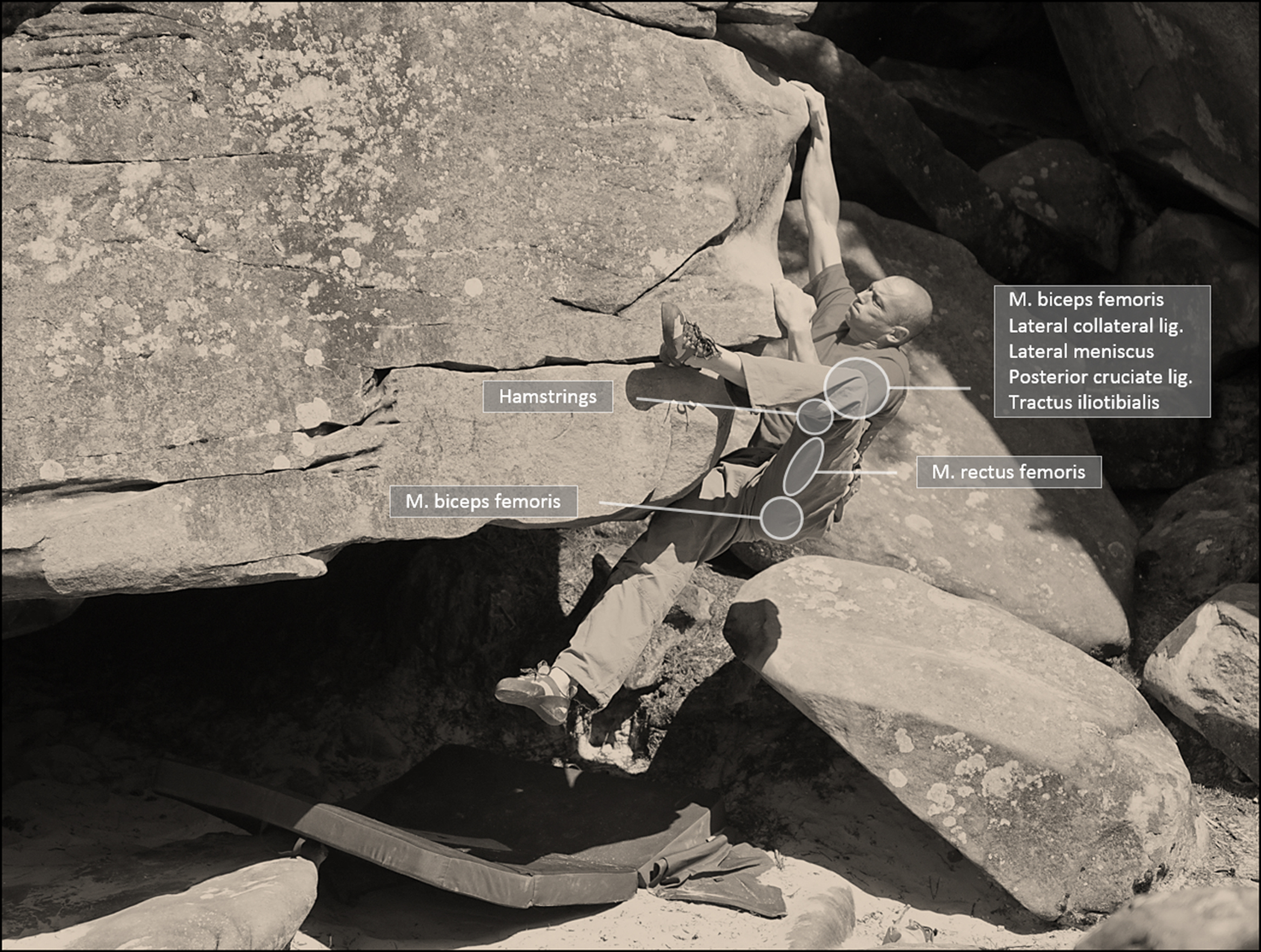
A heel hook performed in outdoor bouldering.
The Heel Hook
With the increasing popularity of bouldering, ropeless climbing in minor height, the complexity of the climbing moves performed has increased. Whereas climbing in the 1970s and 1980s used to be mostly vertical face climbing, the rock features climbed nowadays are more 3 dimensional. This especially applies to the very complex forms of artificial bouldering walls that are also used regularly in competitions. These steep walls require the use of the legs and feet in a more complex form than just standing on them. The legs are used in a similar way as the arms, to hook with the toe or heel, pull and jam (Figure 1).
To perform a heel hook, the back of the foot, the heel, is used to apply pressure onto the hold, while pulling on the foot by flexing the hamstrings (Figure 2). In addition, during this motion the knee is often rotated outwardly, applying a high force onto the back and lateral structures of the knee and leg (lateral collateral ligament, lateral meniscus, posterior cruciate ligament, popliteus tendon, dorsal joint capsule, tractus ileotibialis, hamstring tendons). Climbers often report a snapping or popping sound at the time of injury. Even though lower leg and knee injuries only account for 5.9% to 12.7% of climbing injuries we see, these heel hook injuries can present many different clinical features and thus should be further analyzed. 9 During the last 5 years (2010−2014) we saw 17 climbers with injuries due to this specific technique. The outcome was evaluated at a minimum of 6 months after the injury and classified in an analogous sport-specific score to a score that was used for finger pulley injuries in rock climbers.10,11
Injury distribution.
Patients and Diagnostics
All patients were seen in our sports medical outpatient clinic, which is part of our orthopedic, traumatology, and sports medical department. The sports medical outpatient clinic serves as primary care for sports orthopedics as well as a referral center specialized in outdoor sports medicine. Within the time frame of 5 years (2010−2014) we saw 17 patients complaining about an injury while performing a heel hook (see Table 1). In 6 patients we served as the primary medical consult; 11 patients came to seek a second opinion. Because some climbing injuries are very sport specific (eg, pulley ruptures, heel hook injuries), we are regularily seeing patients seeking a second opinion because initial diagnosis may be missed, because not all medical centers are familiar with these types and mechanism of injuries.
Heel hook injuries from 2010 to 2014
UIAA = Union International des Associations d’Alpinisme; F = female; MRI = magnetic resonance imaging; M = male; PCL = posterior cruciate ligament; PRP = platelet rich plasma.
All 17 patients reported sudden dorsal-sided pain in the knee, thigh, or pelvis. Seven also reported hearing a snapping sound, similar to those reported in achilles tendon tears. Walking was difficult in all cases and all were limping. The time frame in between the injury and the consultation was 1 to 14 days. The clinical evaluation showed point tenderness (tuber ischiadicum, tractus ileotibialis, lateral collateral ligament, or biceps femoris muscle belly), and in few cases minor haematoma. Pain increased in stretching the respective muscle. A visible or palpable muscle gap was present in only 1. After clinical examination and exclusion of the minor injuries (strains) we performed ultrasound (11 patients) and/or magnetic resonance imaging (MRI) (11 patients) in accordance with the suspected injury based on the physical examination. Within our sample of 17 patients, we found 9 patients with injuries at the knee and 8 with injuries at the thigh or the pelvis (Figure 2).
Therapy
In 15 of 17 cases, we received “good” to “excellent” outcomes with a conservative approach, with initial partial immobilization (no weight bearing) and early functional therapy with physiotherapy and in some cases platelet rich plasma injections (Tables 1 and 2). The female patient with the partial meniscus tear obviously needed a surgical procedure. In complete tendon avulsions or partial avulsions over 50% we recommend and perform a surgical repair in climbers. This can be further discussed, as partial avulsion fractures in adolescents (eg, spina iliaca anterior inferior in soccer players) widely receive a conservative approach. 12 Nevertheless, our patients are adults and are likely to perform the exact injury-causing move (heel hook) again; thus, we think in complete tears a surgical repair is reasonable. Again, this is the personal preference of the authors and not evidence based, as there is no evidence here yet. Both options should be discussed with the patient to reach a decision together.
Outcome Score (as used previously 10 )
Discussion
For analysis of the severity and numbers of heel hook injuries, one must understand that we serve as a primary service center for sports injuries but mostly as a referal center for outdoor sport injuries. Thus, most of the patients of this case series were referral cases, so the severity of the heel hook injuries may be biased. Patients experiencing minor cases would probably not see a doctor at all or just have received primary diagnostics elsewhere. Patients with more severe cases came to our clinic to discuss extent of injury, rehabilitation, and consult for surgical repair. For further discussion the 2 main injury locations are addressed independently.
The pelvic heel hook injury
Most of the pelvic injuries were complete or partial tendon avulsions (5 to the back [m. biceps] and 1 to the front [m. rectus]) (Figure 3). We did not find similar reports about these injuries in the climbing literature; nevertheless, these injuries are common in soccer players, mostly in adolescents. 12 Whether these injuries are predisposed through shortened muscle groups at the dorsal side of the leg cannot be answered yet, but it seems reasonable that stretching and proper warming up prevent against such injuries to some extent. We advise climbers to include the backsided muscle groups of the thigh (hamstrings, biceps) into their warm-up routine, especially before performing “extreme” hooks. As team doctors to various climbing teams, we perform functional muscle test also for the back muscles of the leg (hamstrings and biceps) in our yearly athletes examination and present certain stretching exercises in lectures and books (Figures 4A and 4B).6,13
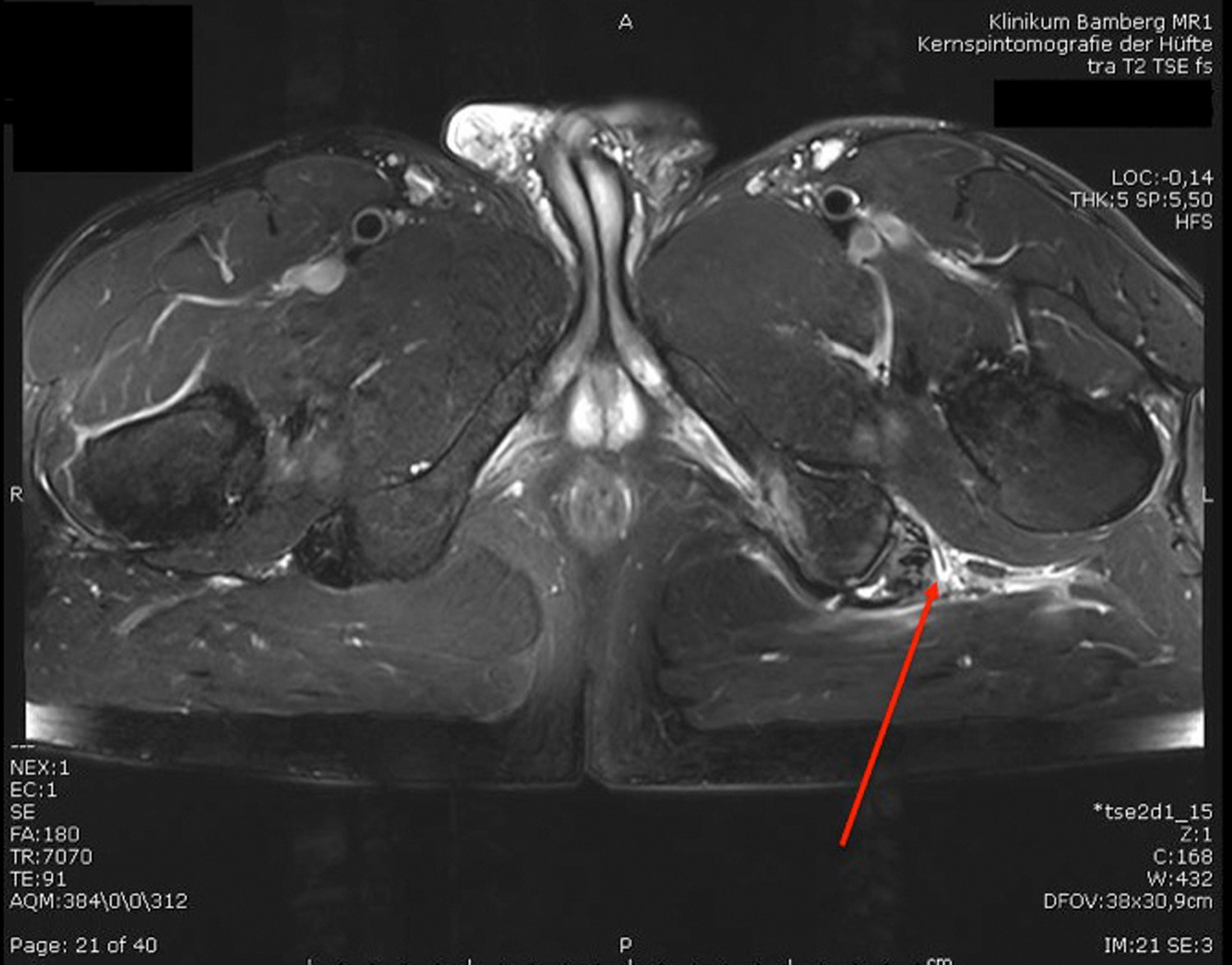
Proximal hamstring tendon tear. Note the seperated tendon insertion to the tuber ischiadicum (arrow) and the liquid around it.
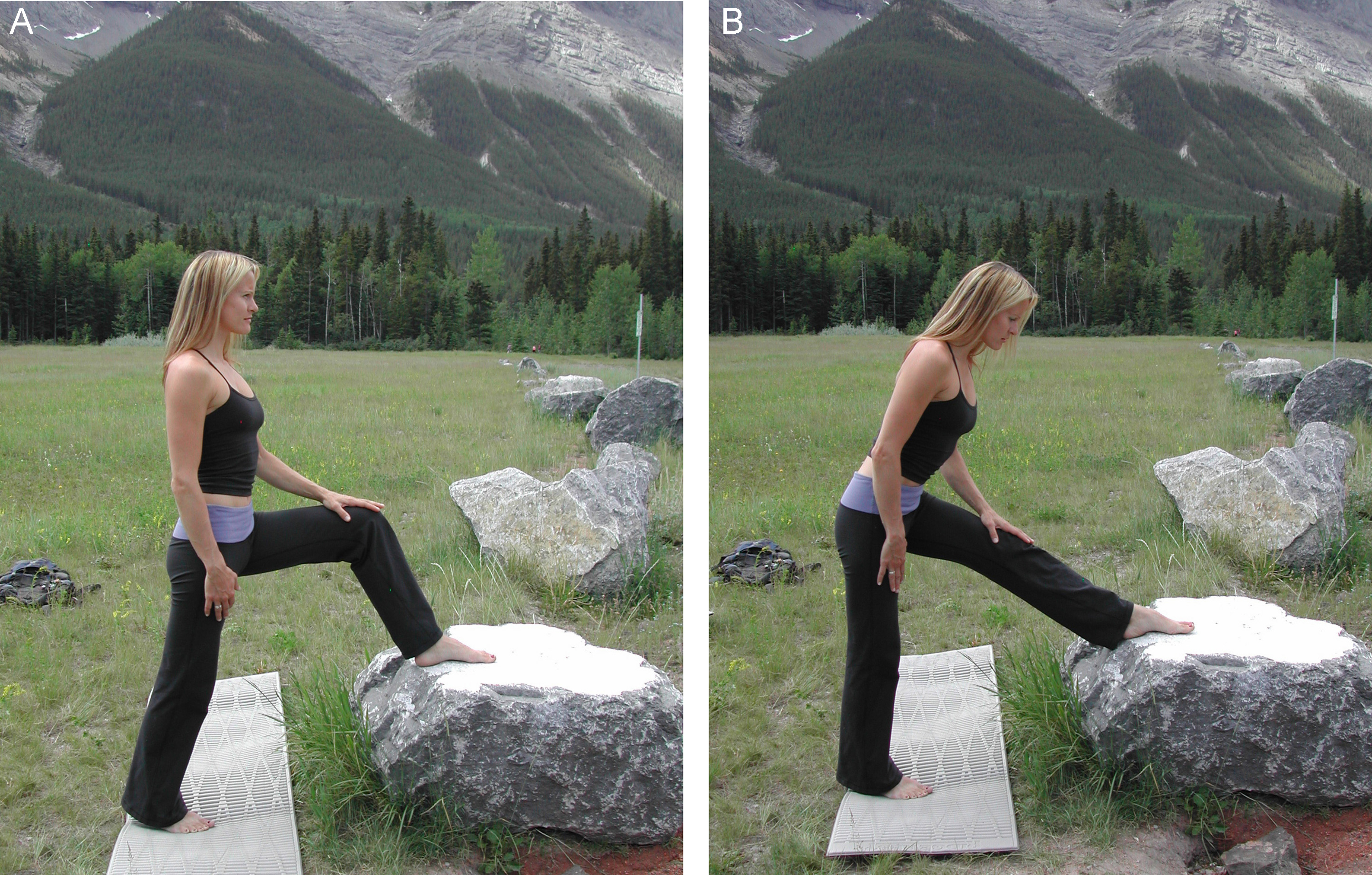
(A, B) Stretching of the hamstring muscles for injury prevention and warm up. A mobile hamstring is essential for the flexibility needed in rock climbing.
The knee heel hook injury
Surprisingly, injuries to the knee while performing a heel hook are also described in martial arts. 14 -16 In these sports, the factor of velocity adds to the injury impact, which makes it more likely to tear an anterior cruciate than in the more static aspect of the heel hook pull in climbing. Davis et al 16 report 2 cases of high grade lateral collateral ligament injury, 2 in climbing and one in jiu jitsu. In jiu jitsu a valgus stress with knee inward rotation is reported, while in climbing an outward rotation of the knee is more important. 17 Thus, the pathology is more to the outside and backside stabilizers—the lateral collateral ligament, the tractus ileotibialis, the dorsal joint capsule, the m. popliteusm, and the m. biceps femoris. In climbing, 1 other case report shows a complete distal m.biceps femoris tendon tear. 8 The ganglion cyst in our patient 8 is probably also a consequence of a partial tendon tear (Figure 5). The patients also frequently reported a popping sound at the time of injury. This may correspond to a change of the pivot of the tractus ileotibialis that then “jumps” over the condyle. Similar to the “pivot shift” sign, as known in anterior cruciate injuries, the heel hook position causes high tension on the tractus. While the hook is performed, there is frequently an active knee flexion involved, which thus changes the pivot of the tractus.
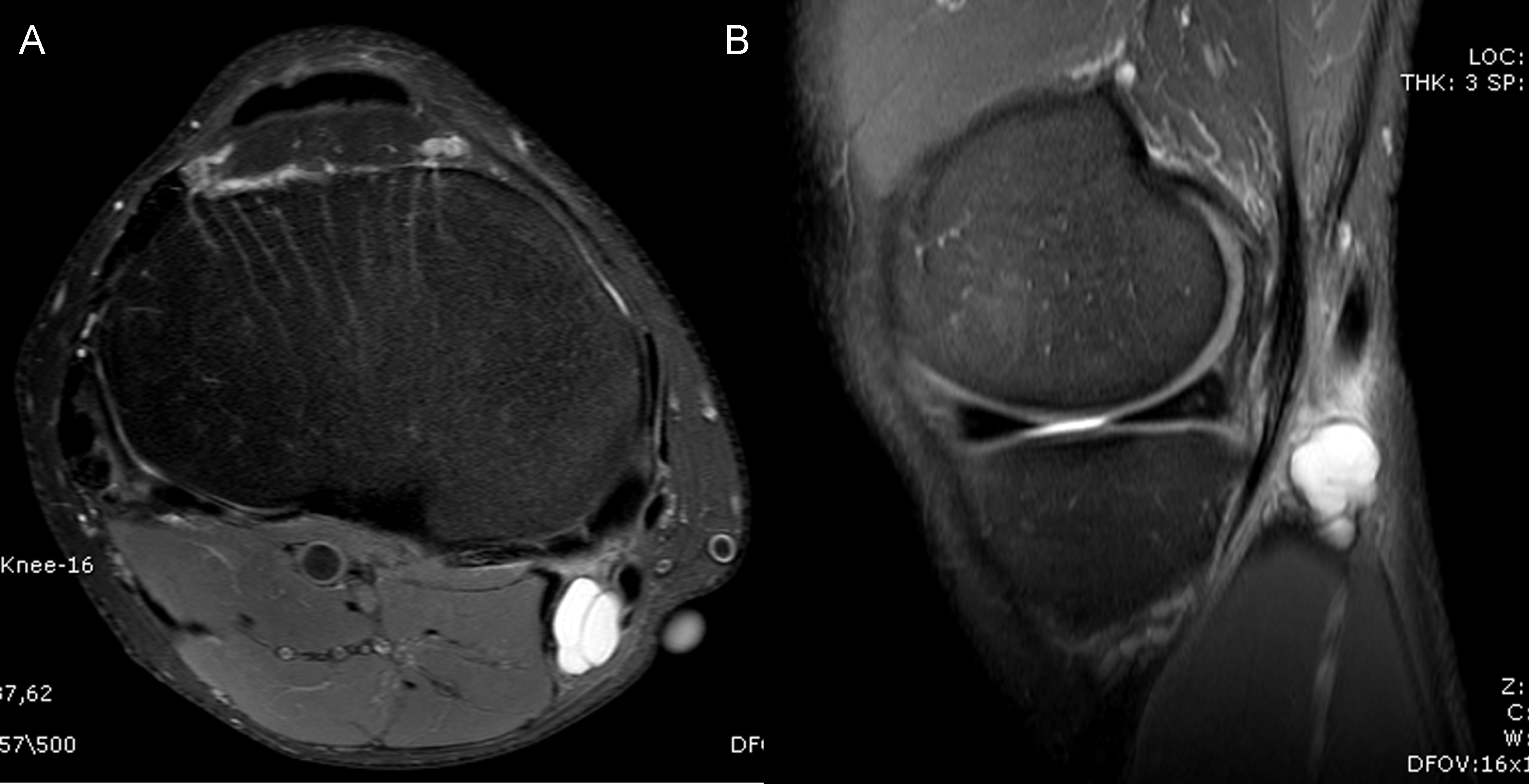
Ganglion cyst after hamstring tendon strain due to a heel hook. Note the white fluid cystic formation at the back of the knee, next to the hamstring tendons.
Austere environments
If these injuries are happening in an easy accessible sport climbing area or even indoor climbing wall, primary care and patient transport may not be a problem. Nevertheless, climbing is mostly performed outdoors and often in remote places. Even if these injuries are not life threatening or severe in the Union International des Associations d’Alpinisme (UIAA) classification (UIAA grade 2), they may become a problem if occurring in austere environments and on expeditions. 18 All of our patients reported a great amount of pain and were limping; thus, long hikes or descends may be difficult. For in-place management we recommend elastic bandaging, splinting, partial weight bearing if possible (eg, with ski poles), and analgesia in accordance with the standard guidelines. 19 Diagnostics on site will be only clinical or, if available, through portable ultrasound.
MRI diagnostics: justified or overshot?
After clinical examination and conjecture, ultrasound and MRI help to specify the diagnosis. Although other climbing injuries (eg, pulley injuries) are predominantely examined through ultrasound, this is more difficult in heel hook injuries. Also most of the climbing patients are ambitious and want to resume climbing as soon as possible. Ultrasound diagnosis does not always lead to a definitive diagnosis here. Pelvic muscle avulsions are especially difficult to detect, and cruciate ligaments injuries are not seen in the ultrasound at all. We think this justifies the diagnostic cost of an MRI, which has the highest sensitivity and specificity. Especially in pelvic injuries, it is difficult to determine whether a tendon has a minor or major partial avulsion without the MRI.
Prevention
With respect to the literature in prevention of muscular injuries, a warm-up routine, an avoidance of muscular imbalances, and stretching and flexiblity training are recommended. A warm-up for the backsided thigh muscles (hamstrings and biceps) should especially be performed, which certain stretching exercises provide. 6 Also a general muscle warm-up such as easy jumps, a little run, or similar should be performed before the extreme stress. Muscular imbalances, as frequently seen in athletes (strong quadriceps and in contradiction shortened biceps femoris) need to be detected and avoided. 13 Thus, a yearly examination by a sports physician is important to all high class athletes. Prevention of the knee heel hook injuries are more difficult, because they do not originate from shortened muscle groups. They are due to performing the hook maneuver too ambitiously. Thus, the most effective prevention will be information to climbers and trainers about the injury pattern. The athletes need to understand that the structures of their knees have a limit that they need to keep in mind while climbing. To what extent physiotherapeutic tests and sports medical monitoring or testing (eg, functional movement screen) will help to prevent these injuries is under discussion among the physiotherapeutic and sports medical teams of various climbing national teams and the medical commission of the International Federation of Sport Climbing. Further studies are important to address these preventive measures and their implementation into training routines.
Conclusions
In rock climbing, injuries of the lower extremities will increase as the heel hook is used more frequently today with changing sport preferences. MRI shows the proper diagnosis and the proper therapeutic approach is conservative treatment with stress reduction. The outcome after heel hook injuries is good to excellent in most of the cases. Warm-up routine, an avoidance of muscular imbalances, and flexibility training can help to avoid injuries during heel hook.