
Abstract
Objective
We propose a formula as a means to estimate the number and incidence of snakebites treated per annum in KwaZulu Natal (KZN), South Africa.
Methods
Using an unvalidated formula that includes an antivenom ratio, we crudely estimated the total number of snakebite presentations in KZN. Using antivenom supply data from the central pharmacy, we stratified a sample of 6 hospitals that were surveyed to establish an antivenom ratio, that is, the total number of patients receiving antivenom to the total number of snakebite presentations at hospitals. The antivenom ratio and the average number of antivenom vials for treated snakebites were incorporated into a formula to crudely estimate the number of snakebite presentations. This was then applied to all public hospitals and districts in the region.
Results
Seventy-eight percent of public hospitals were included. The mean antivenom ratio derived from the sample hospitals indicated that 12% (95% CI, 10–14%) of snakebite presentations received antivenom. We estimated an annual total of 1680 (95% CI, 1193–2357) snakebite presentations to hospitals. Two thirds of cases (1109 of 1680) were in the low-lying subtropical coastal region. Few cases were in the higher, cooler regions of KZN (87 of 1680) or the metropolitan city of Durban (93 of 1680). The overall incidence for KZN was 16/100,000. The estimated cost of snakebite in KZN was between $1,156,930 and $2,827,848.
Conclusions
We propose an alternative method to estimate the annual number of snakebite presentations to hospitals.
Keywords
Introduction
Snakebite is an important disease that is difficult to quantify in terms of patient numbers and outcomes. The worldwide data on snakebite are limited, and region-specific data on snakebite numbers in Southern Africa are lacking. These data are critical to understand disease burden and to institute appropriate prevention and treatment strategies. Global information is sourced from various government departments and global organizations such as the World Bank, World Health Organization, and the United Nations. These reports are supported by scattered studies from hospital records and local surveys in communities affected by snakebite. 1 The current published data suggest that the greatest burden rests in Asia (approximately 15,400–57,600 deaths per annum) and sub-Saharan Africa (approximately 3500–32,100 deaths per annum). 2 Estimates put the number of snakebites in sub-Saharan Africa at 100,000 to 500,000 per year. 3 It is striking that the quoted snakebite numbers have a wide range and fall short of providing specific regions with accurate estimates. This is largely because of poor documentation of snakebites by healthcare practitioners and health facilities, lack of collation of cases by central health authorities, and healthcare practitioners such as traditional healers who have no formal documentation process.1,4 Snakebite is not a reportable disease, and as a result there is a noticeable paucity of good data from South Africa. In addition, there are no national standardized snakebite treatment guidelines, resulting in different prescribing habits from clinicians in the hospitals of South Africa.
One region in South Africa known to have a high number of snakebites is KwaZulu Natal (KZN). 5 –7 However, there are no accurate data on patient numbers and snakebite distribution. Various authors have noted that the mix of poverty, tropical climates, and a rural subsistence population creates a hotspot for snakebites. 8 –10 KZN has areas that have these 3 ingredients. We aim to use a different approach for estimating the number and incidence of snakebites presenting to public hospitals in KZN by using a formula. By combining antivenom supply figures in the province and extrapolating the data derived from the formula, we hope to quantify the distribution of snakebite presentations and the costs to healthcare in KZN.
Methods
Setting
Serving the health needs of KZN’s 10.8 million people are 11 districts with 72 public hospitals. Public hospitals are nonprivate institutions that are free-access hospitals serving the vast majority of South Africans. The majority of these are local district hospitals, 12 are regional hospitals, and 4 are tertiary referral centers. 11 –13 The starting point for estimating snakebite numbers is the KZN Department of Health central pharmacy antivenom supply data, based in Durban. The KZN central pharmacy is the only supplier of antivenom to public hospitals in KZN and keeps accurate records. All public hospitals that require antivenom are supplied according to need without constraints. Using these supply figures for a 2-year period, we identified the hospitals that treated snakebites.
Sample Population
Patients who presented to a public hospital in KZN with snakebite were included in the study. Within this group, all patients who were treated with antivenom were admitted for a period of observation. A stratified sample of 6 hospitals spread across the province were selected on the basis of having treated a reasonable number of snakebites with antivenom (Figure 1). Such a selection was made by including those hospitals that prescribed at least 40 antivenom vials during a 2-year period. We made the assumption that these sites had treated enough snakebites to provide an adequate patient sample size for analysis. Unpublished data from a retrospective analysis of snakebite for 5 years at the sixth hospital (a snakebite referral center) in the northeast of KZN were also included. Patient demographic details were stored on a password-protected Excel (Microsoft Corp, Redmond, WA) spreadsheet and anonymously analyzed using a simple numbering system.
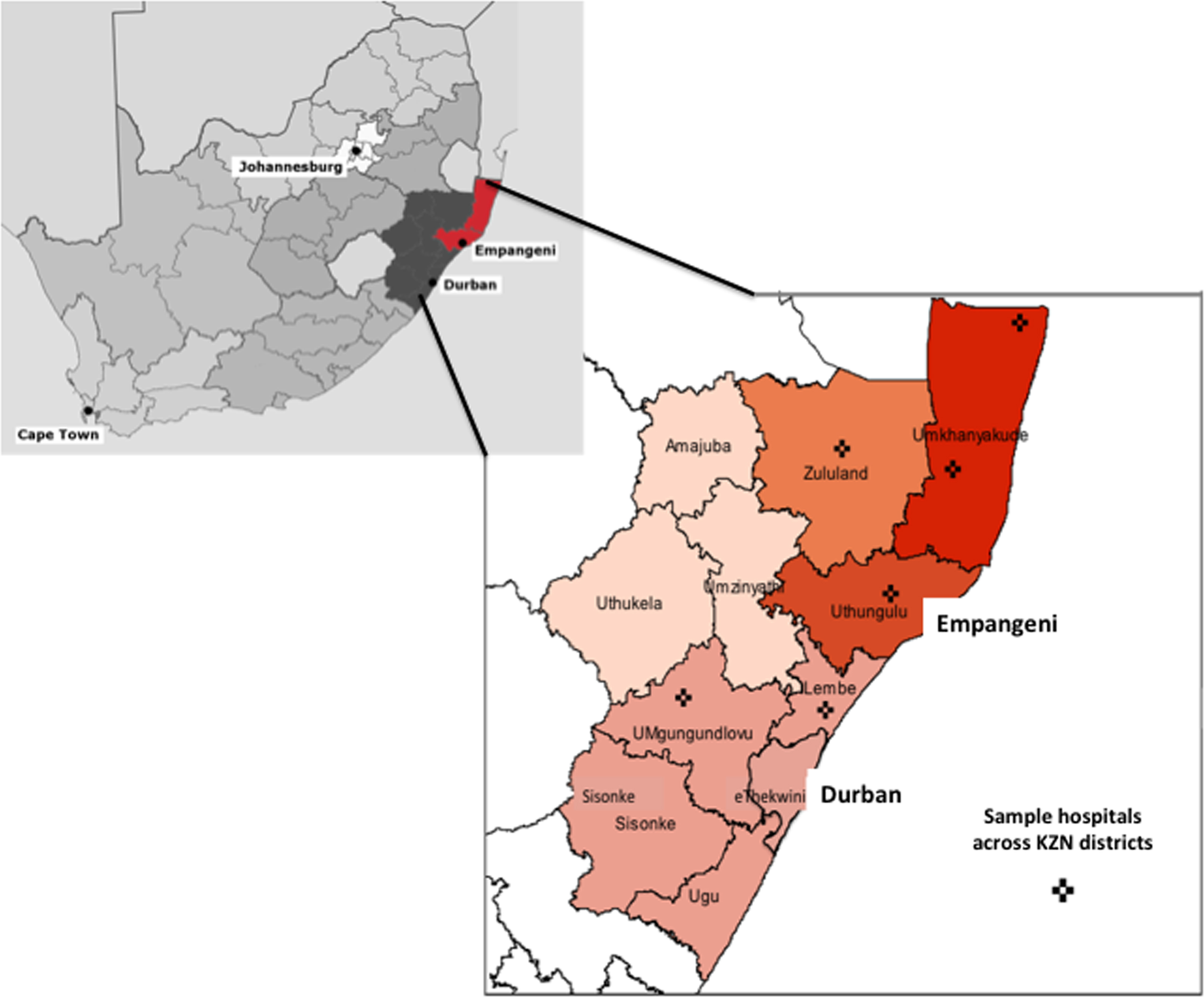
Map of KwaZulu Natal (KZN) province in the context of South Africa and expanded to show the distribution of the 6 sampled hospitals per district.
Data Collection And Measurement
We collected data on the number of antivenom vials distributed to hospitals in KZN using supply records from the provincial central pharmacy, which is the sole supplier to public hospitals. In addition, a survey using hospital admission records was conducted at each sample site. Any person bitten by a snake who presented to the hospital was entered into the admissions book. Details on whether the patient was envenomated or not were not captured. Those patients who received antivenom were documented. Because not all snakebites presenting at a given facility require antivenom treatment, we crudely estimated the number of snakebites using a formula created by the authors that has not been validated previously. The formula includes the antivenom ratio, which is the proportion of patients receiving antivenom to the total number of patients presenting with snakebite at each sample facility. The formula was then applied to all hospitals that were not in our sample and extrapolated to each district. The total number of snakebite presentations to public hospitals can be calculated using this formula:

Data Analysis
We used the data from the sample hospitals to calculate the weighted average (scaled by caseload) of the pooled effect size for the average number of vials used per patient as well as the antivenom ratio. We also used the 95% CIs from these estimates to obtain worst versus best case projections of snakebites. The formula, derived from the 6 sample hospitals, was applied to all hospitals treating snakebite to estimate the total number and distribution of snakebite presentations in KZN. Population statistics were retrieved from the KZN Provincial Census data, and hospital admission figures were obtained from the KZN provincial District Health Information Systems database. 11 –13 Population for 2013 is estimated using a growth rate of 1.018% applied annually. Ethics approval was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu Natal (Ref. BE 034/01). Informed consent from patients was not obtained because all patient data were analyzed anonymously and numbered (patient names and file numbers were excluded) sequentially. Permission for accessing case files was obtained from the KwaZulu Natal Department of Health. All data were collated using Excel (Microsoft 2010; version 14.4.7) and analyzed using Stata (version 13; StataCorp LP, College Station, TX) in consultation with a statistician. Risk maps were constructed using MapInfo Professional (Pitney Bowes Software, Stamford, CT).
Results
The KZN central pharmacy supplied antivenom to 56 hospitals (78% of all public hospitals) during 2012 and 2013. The number of SAIMR polyvalent antivenom vials (South African Vaccine Producers, Johannesburg, South Africa) that were distributed to these institutions during 2012 and 2013 was 1680. The annual average number of vials used in KZN during this period was 840.
Antivenom Ratio (Stratified Sample Hospital Data)
The average antivenom ratio (number of snakebites treated with antivenom to number of snakebite presentations) calculated from the 6 sample sites was 0.12 (95% CI, 0.10–0.14). The total number of snakebite presentations from this data set is 8 times the number of cases that received antivenom. The average number of vials used per patient receiving antivenom is 4.9 (Table). The annual mean number of snakebite presentations to the sampled hospitals was 72. Figure 2 graphically represents these data (sampled hospitals numbered 1 to 5 and referral hospital numbered 6) with their associated weighting and calculated weighting estimates for the antivenom ratio.
Results of the survey from the stratified sample hospitals in KwaZulu Natal
Total number averaged for 5 years.
Antivenom ratio derived from weighted estimates (WE) for the patients receiving antivenom to the total number of snakebite presentations. The larger the number of patients per hospital, the greater the allocated weighting. The antivenom ratio can be reflected as a percentage by multiplying by 100.
Local municipalities from which patients attend the sample hospitals.11–13
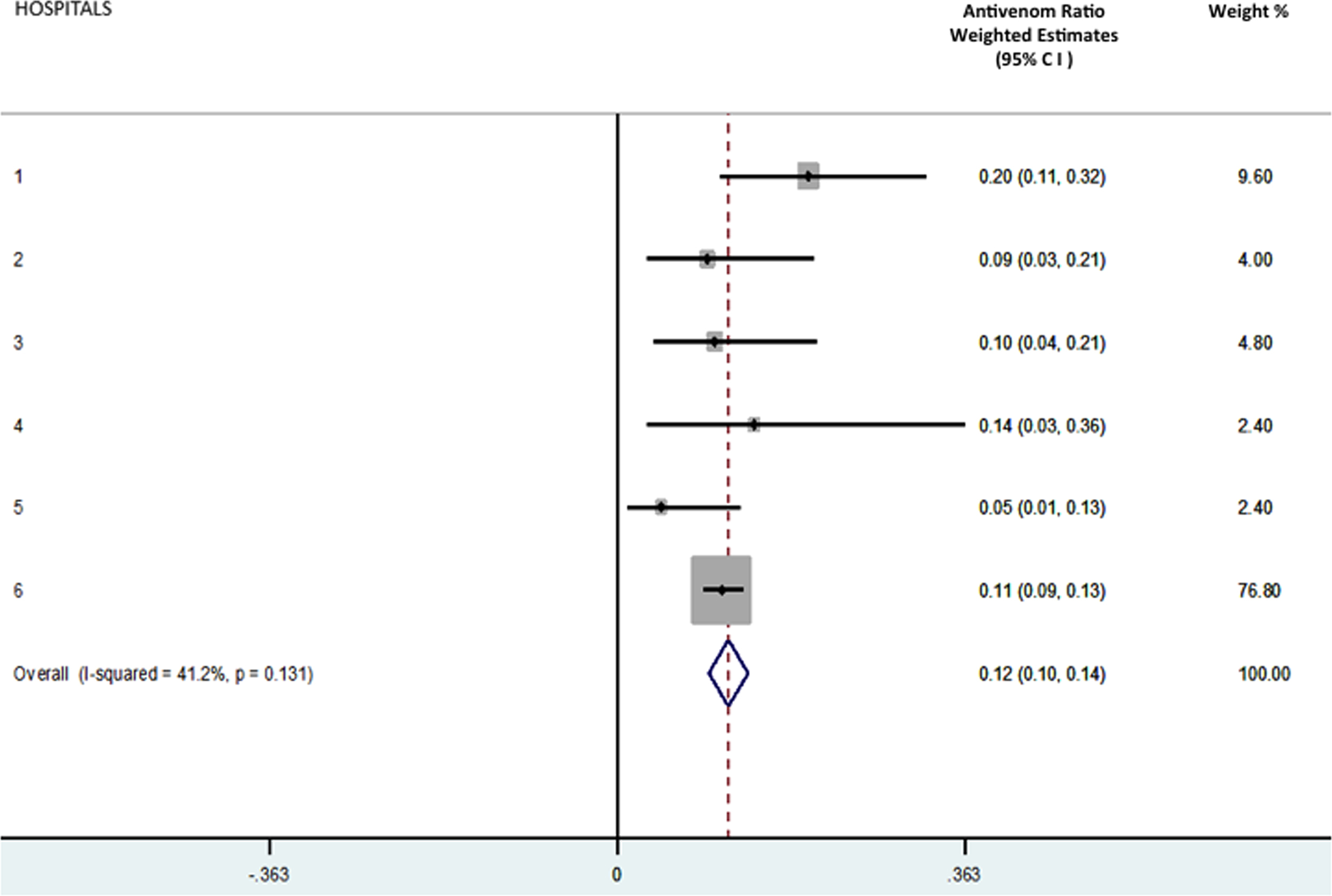
The weighted estimates of each hospital’s antivenom ratio (hospitals 1 to 6) plus the overall ratio for the stratified sample.
Number and Distribution of Snakebites In Kwazulu Natal Using The Antivenom Ratio
All hospitals (56 in total) that treated snakebites with antivenom had the formula applied to their data, and the results were extrapolated to each district (for distribution) and KZN as a whole. The estimated total number of snakebite (treated and untreated) admissions per annum in KZN is 1680 (95% CI, 1193–2357). The projected number of snakebite patients treated with antivenom in KZN is 202 (12% of snakebite presentations). The majority of projected case presentations were in the subtropical northeast coast of KZN (Figure 3, region 4) and accounted for 67% (1109 of 1680) of all hospital presentations. As expected, this region treated the greatest number of cases with antivenom (133). Of note was the densely populated Durban metropolitan area, which treated only 93 cases (Figure 3, region 1). The higher, cooler inland areas of region 2 saw very few cases and collectively represented only 5% (87 of 1680) of the total.
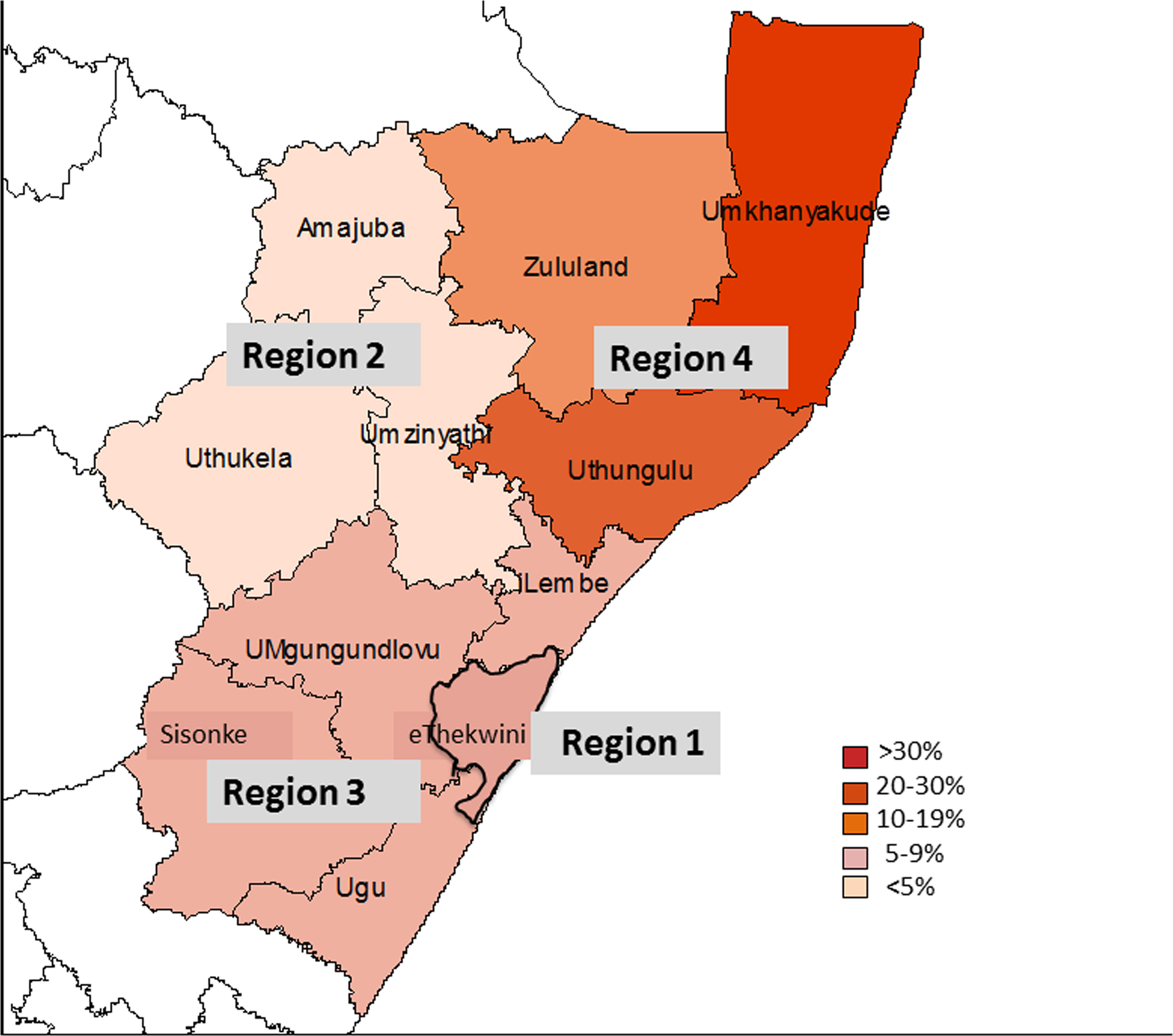
The percentage of snakebite presentations to public hospitals per district in KwaZulu Natal extrapolated from the derived formula.
Estimation of The District and Provincial Snakebite Incidence
The sample hospitals had an incidence that ranged from 5.7 to 90 per 100,000 population (Table). 11 –13 The calculated and extrapolated overall KZN provincial incidence was 16/100,000 population (Figure 4). Two districts in region 4 (uMkhanyakude and uThungulu) had a high incidence, 82/100,000 and 47/100,000 population, respectively. Figure 4 depicts the relative incidences per district in KZN, highlighting the high incidence of snakebite in the low-lying, humid coastal regions compared with the low incidences in the higher, drier inland regions.
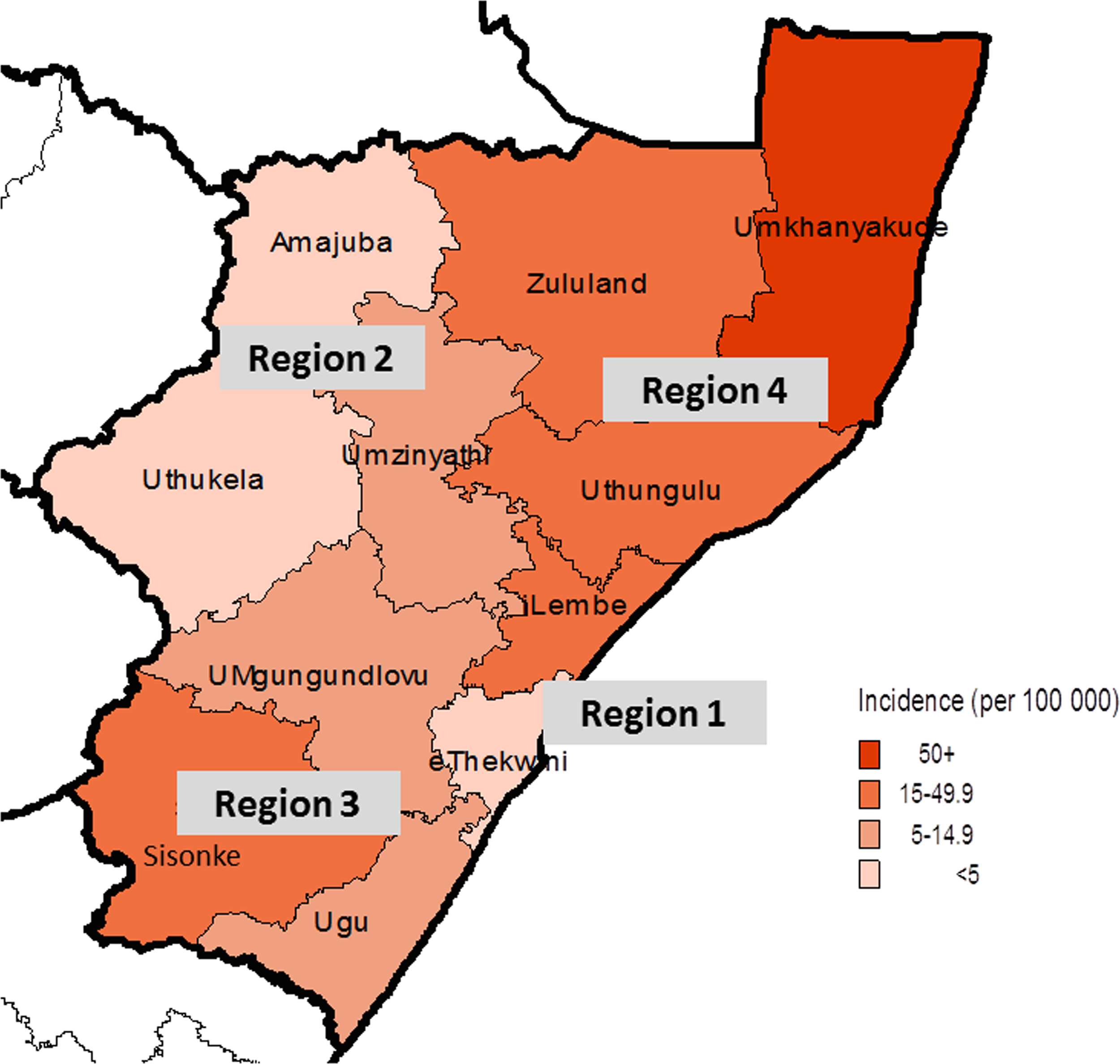
The relative incidence of snakebite presentations to public hospitals per district in KwaZulu Natal.
Cost of Antivenom Treatment In Snakebite
The cost per vial of polyvalent antivenom (data from KZN central pharmacy) in the public sector is approximately $80. The total cost per annum for an average of 840 vials used equals $67,200. The antivenom cost per patient receiving antivenom (average, 5 vials) is $400. The total cost to KZN for snakebite admissions can be estimated using published data on trauma admissions for which a daily fee has been estimated at an average cost of $243 per patient per day (KZN Department of Health, cost for a ward bed in 2014; unpublished data). In KZN, snakebite is classified under trauma because it is regarded as an injury. Currently, specific costs for admitted snakebite patients have not been quantified in our setting, and the use of trauma figures acts as a crude surrogate for an estimate. Patients who are hospitalized with snakebite spend on average 3 to 7.6 days in the hospital before being discharged.14,15 Using these values (range, 3–7.6 days), a crude estimate of a single snakebite admission ranges from $703 to $1780. The total cost of snakebite admissions in KZN, based on the low and high hospital stay and the estimated 1680 cases, equals a low estimate of $1,156,930 (95% CI, $821,558–$1,623,145) and a high estimate $2,827,848 (95% CI, $2,008,090–$3,967,404). Added to this cost is the total cost of antivenom per year ($67,200).
Discussion
Strategies to obtain data on snakebites in southern Africa presented in the literature are not accurate and poorly describe case numbers within a specific region. Studies that are community-based using household surveys are challenging because these are labor-intensive and it is difficult to cover large areas. 14 Initial community research should begin within the identified hotspots and possibly be extrapolated to the immediate district. The majority of research in hospitals describes envenomations only, although published data on all snakebite presentations is scarce (envenomation plus non-envenomation bites). 1 Snakebite in South Africa is not a reportable disease, making accurate record keeping unreliable. In response to these difficulties, we have proposed using a formula that incorporates antivenom distribution data and a formula derived from a sample of hospitals to quantify the number of snakebites presenting to public hospitals in KZN as a whole. The basis of this model relies on the accurate antivenom distribution data from the sole provincial central pharmacy. Almost 80% of hospitals in KZN received antivenom during this period, which provided investigators with good provincial coverage for the framework of the proposed model.
Our survey of sample hospitals produced an average antivenom ratio of 0.12, ie, 12% of snakebite presentations were prescribed antivenom. This ratio is supported by previously published research within the province that on analysis yielded an average ratio of 0.1. 5 –7,15 These prescribing ratios are lower than those reported by studies conducted in West and East Africa, which report ratios upward of 0.33. 4 Our data are consistent with reported prescribing habits of clinicians treating snakebites in our region during the past few decades.
One vial of South African Vaccine Producers polyvalent antivenom contains 10 mL of concentrated antibodies to the venoms of 10 dangerous snake species. These include the puff adder (Bitis arietans) Gaboon adder (Bitis gabonica), cobra species (Naja nivea, Naja mossambica, Naja melanoleuca, Naja annalifera), mamba species (Dendroaspis polylepis, Dendroaspis augusticeps, Dendroaspis jamasoni), and the rinkhals (Haematochus haematochus). Our local guidelines suggest an initial loading dose of 5 vials polyvalent antivenom followed by further doses according to clinical response.16,17 Dosing is stopped when an adequate response is seen, such as cessation of swelling progression, reversal of muscle weakness, or bleeding that has stopped. Patients are further monitored for 48 hours after antivenom treatment. The average number of vials per patient receiving antivenom in this study was approximately 5, which is lower than expected, and in our experience 10 or more vials are usually required to neutralize the effects of envenomation. The significant risk of antivenom anaphylaxis (range, 19%–39%) reported from some studies in the region may explain this trend, causing doctors to stop antivenom infusions before they have been completed. 3 ,5,7,15
Our results show that there is significant variation of snakebite numbers across KZN. The subtropical low-lying northeast of KZN accounted for the majority of snakebites, in keeping with other studies showing hot, humid climates in low-lying rural areas to be hotspots for snakebite. 9 The 3 districts representing this region (uMkhayakude, Zululand, and uThungulu) are all underdeveloped and have primarily rural subsistence populations. These observations are further supported by snake distribution data presented by Bates et al, 18 which supports the presence of a numerous varieties of venomous snake species (eg, puff adder and Mozambique spitting cobra) in the eastern coastal region of KZN. Very few snakebites occur in the cooler, higher altitude regions of the north and northwest of KZN, which border on the Drakensberg mountain range, suggesting that altitude and temperature are significant factors in snakebite incidence. Geographical variations within a region clearly affect the number of snakebites. Global estimates and health organization statistics do not bear relevance to this and are often not practical for planning management strategies at the regional and district levels.
Using global studies, Kasturiratne et al 1 estimated the incidence for southern sub-Saharan Africa to be 8.87/100,000 population. The overall incidence of snakebite presentations to public hospitals in KZN was 16/100,000 population. The subtropical coastal districts in our study had higher incidences (81.6/100,000 population in the uMkhanyakude district). This was expected because earlier studies from these areas alluded to similar figures and range from 31/100,000 population to 97/100,000 population. 5 –7,15 The higher Amajuba and uThukela regions and the urban Durban metropolitan area saw few snakebites per population. This supports the observation that snakebite distribution is highly variable in KZN and is rare in the higher, cooler areas and in urban environments. 9
The overall cost of snakebite admissions is significant. The cost of antivenom is relatively low in comparison with the expense of admitting patients with severe presentations for prolonged periods.
When one considers that many snakebites occur during work activities such as farming, cultivating fields, and transiting to and from work, snakebite can be classified as an occupational disease in these settings. A study in South America by Otero-Patiño 10 in rural communities, where agriculture is the main industry, described 85% to 90% of snakebites to be occupational. Sugar cane farming is a major income generator in KZN, and it requires a labor force to manually cut the raw cane before it is processed. This activity makes cane cutters vulnerable to snake encounters. The loss of income to the industry and individual households from snakebite has yet to be estimated.
The proposed method and formula appears to support previous research on snakebites in KZN and our experience in this region. Such a method should be externally and prospectively validated in future research and could potentially be used to monitor the prescribing habits of doctors and the trends of snakebite presentations in KZN with time.
Limitations
We stratified sample hospitals from a group of hospitals that received antivenom vials for snakebite treatment on the assumption that hospitals treating snakebite would stock antivenom for severe cases. Our sample hospitals were selected as a stratified convenience sample, which reduces the accuracy of the estimates presented. A more comprehensive sampling strategy would provide a more accurate representation of the snakebite numbers and prescribing habits. In addition, some hospitals and primary healthcare clinics may have treated patients with snakebite and discharged them home without using antivenom during a 12-month period. We attempted to reduce this bias by using 24 months of antivenom distribution data in an attempt to include as many facilities as possible.
This model underestimates the true number of snakebites because it does not account for snakebite presentations that did not present to a hospital, such as those patients who exclusively attended primary health clinics, visited traditional healers, or received home-based care. In some parts of Africa this number far outweighs hospital admissions and can range from 60 to 80%.19,20 In our region there are no robust data on the number of snakebite patients who do not seek medical attention from hospitals. One local snakebite community survey yielded 39% of snakebite cases that did not present to the hospital. 14 The sample hospitals for this study did not include private hospitals, which do see a small number of snakebites but do not receive the supply of antivenom from the KZN central pharmacy. Private hospitals individually order antivenom directly on a needs basis and this is difficult to quantify. As a principle, any estimate of snakebite numbers will fall short of the true number. This method is reliant on accurate and reliable data on antivenom distribution and reflects public hospital attendees only. Such a method will not apply to countries where antivenom supply is not as well controlled.
Conclusions
Quantifying the number of snakebite presentations is challenging. We have proposed a formula that uses specific parameters as an alternative method to crudely estimate snakebite numbers. Our results from some of the districts are similar to those of previous observational studies done in these areas. More research is required to validate such a method. Of importance is the need for large community surveys that can reflect the proportion of patients who do not present to hospitals. Combining both these approaches would bring us closer to the true snakebite burden in KZN.
Footnotes
Acknowledgments
Support funding was by MEPI (Medical Education Partner Initiative); US Global Aids coordinator; US Department of Health and Human Services; and the National Institutes of Health (grant No. R24 W008863). The contents are solely the responsibility of the authors.
☆
Supported by a grant from MEPI (Medical Education Partnership Initiative).