
Abstract
Risk of injury in cold environments is related to a combination of athlete preparedness, preexisting medical conditions, and the body’s physiologic response to environmental factors, including ambient temperature, windchill, and wetness. The goal of this section is to decrease the risk of hypothermia, frostbite, and nonfreezing cold injuries as well as to prevent worsening of preexisting conditions in cold environments using a preparticipation screening history, examination, and counseling. Cold weather exercise can be done safely with education, proper preparation, and appropriate response to changing weather conditions.
Introduction
Cold exposure puts wilderness and outdoor athletes at risk for hypothermia, frostbite, and nonfreezing cold injuries. Cold weather exposure during outdoor activities does not cause adverse effects on health and physical performance in most people. However, individual tolerances to cold will vary based on the duration of exposure, ambient temperature, and preexisting risk factors unique to the individual.1,2 The incidence of hypothermia and frostbite in athletes during winter months is low. 3
Hypothermia is defined as a drop in core temperature below 35°C (<95°F).1,4 Symptoms of hypothermia correlate with core body temperature most of the time, but symptoms can be variable at a given core body temperature. Impaired thermoregulation can lead to hypothermia at warmer than expected temperatures1,2 [Zahren et al 2014 In Press (W&EM Dec 2014)]. Frostbite occurs when the skin and deeper tissue temperature drops below —0.5°C (31.1°F).4,5
It is most common on exposed skin, hands, and feet due to peripheral vasoconstriction and lower tissue temperatures. Contact frostbite can also occur when the skin is in contact with liquids, such as gasoline, alcohol, and stove fuel, that can cool well below the skin freezing temperature and evaporate rapidly increasing the rate of heat transfer. 4
Nonfreezing injuries include trench foot, chilblains, and cold urticaria. Trench foot typically occurs when feet are exposed to cold and wet environments in the temperature range of 0 to 15°C (59°F) for prolonged periods of time without the ability to warm and dry the skin. 4 –6 This medical condition is characterized by skin irritation, rash formation, and foot ulcerations. 4 –6 Chilblains is a superficial skin injury also occurring in cold wet environments. After 1 to 5 hours in cold conditions, susceptible patients develop tender erythematous papules that typically resolve in 2 to 3 weeks. 4 ,6,7 Cold urticaria is an allergic response to cold resulting in erythematous pruritic hives within minutes of exposure to cold. 4 ,6,8 Severe allergic reactions to cold can progress to anaphylaxis in rare cases. 4 ,6,9,10 In addition, exercising in cold weather conditions can worsen preexisting respiratory and cardiovascular conditions. 4 Nearly all cold-related injuries can be prevented with education, preparation, and appropriate response to changing weather conditions.
Methods
A PubMed search was initiated to identify articles with the key words wilderness preparticipation examination and cold injuries. Articles were assessed as to their relevance to cold injuries and outdoor experience.
Goals of the Preparticipation Physical Evaluation and Safe Participation
The goal of the preparticipation examination is to decrease the risk of hypothermia, frostbite, and nonfreezing cold injuries and to prevent worsening of preexisting conditions in cold environments. This section is designed to modify risk through athlete and medical provider education regarding behaviors, medical conditions, and environmental conditions that increase risk of cold-related injury. Wilderness adventurers and athletes have the responsibility to dress for the cold as well as recognize and respond quickly to a change in weather or personal condition that increases risk.
Physiologic Response to Cold
The human body attempts to maintain a core body temperature near 37°C (98.6°F). Heat exchange occurs through convection, radiation, conduction, and evaporation. 11 Heat exchange from the skin to the environment is influenced by a number of factors, including air temperature, humidity, wind speed; solar, sky, ground radiation; and insulation properties of clothing.
The body responds to acute cold exposure by increasing metabolic heat production and decreasing heat loss. 4 As the core temperature drops, heat production is increased through increased physical activity and involuntary shivering.4,12 Shivering intensity varies dependent on the level of cold stress. 4 Total body oxygen uptake is increased with shivering. 4 In addition, peripheral vasoconstriction minimizes heat loss by shunting peripheral blood away from the skin and subcutaneous tissue to decrease heat transfer to the environment.4,13 Peripheral vasoconstriction begins when skin temperatures drop below 34 to 35°C (95°F).4,14 This heat-saving mechanism occurs at the expense of a decline in skin and muscle temperatures, increasing the risk of frostbite injuries and decreasing muscle performance and coordination.4,5
The combination of cold, wet, and windy conditions poses the greatest hypothermia risk to the wilderness athlete. Therefore, temperature alone cannot be used to determine risk of cold injury. This is demonstrated in the windchill temperature index below, which reflects convective heat loss rates (Figure 1).15,16
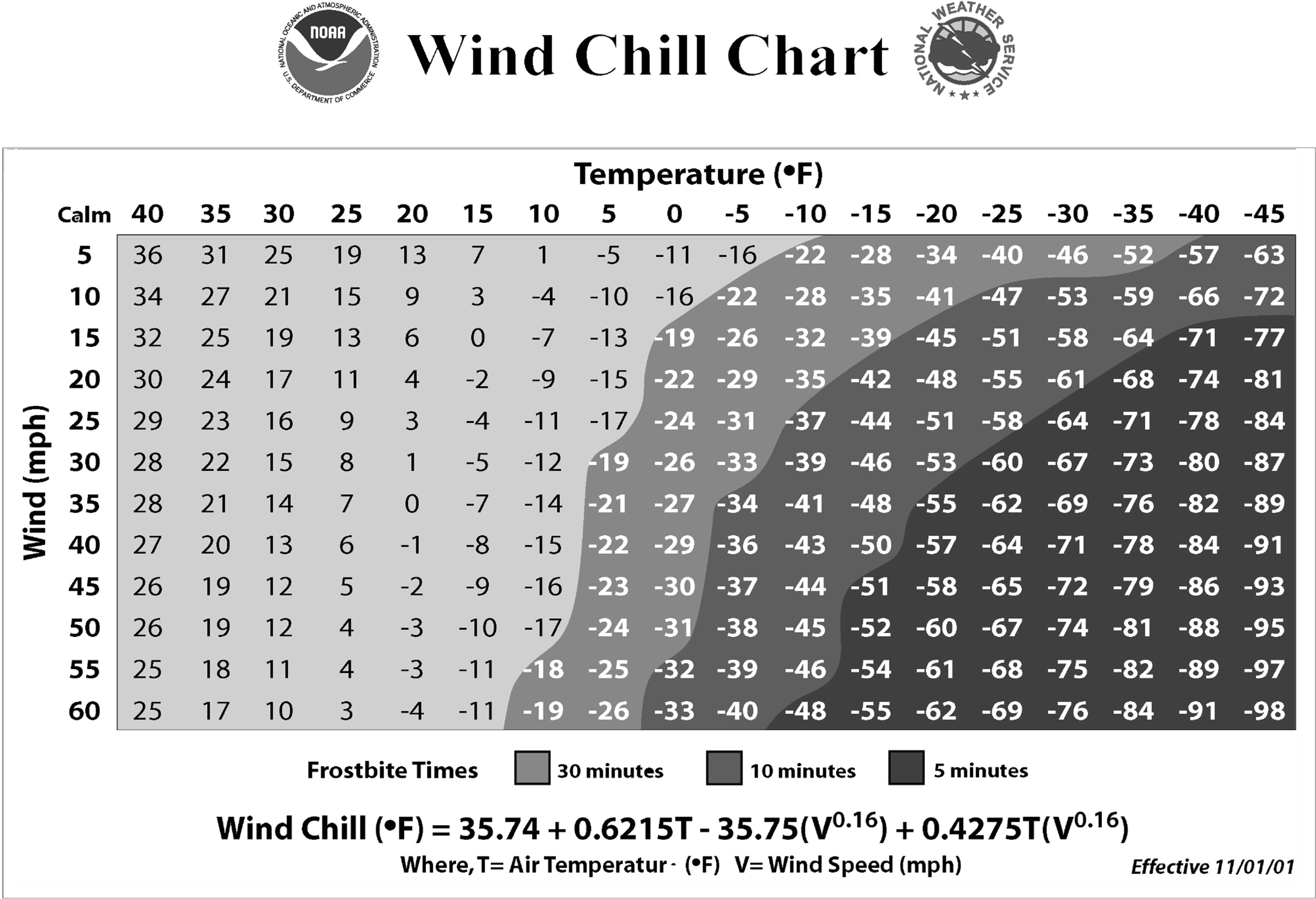
Frostbite times based on windchill temperatures. 15
Risk Factors for Cold Injury
A balance of heat production to heat loss is required to maintain a normal core body temperature in the resting and exercising individual. Decreased heat production, increased heat loss, impaired thermoregulation, and previous cold injury increase the risk of hypothermia, frostbite, and nonfreezing cold injuries.4,17 Windchill can be a significant factor with certain outdoor sports such as winter cycling and Nordic skiing, where athletes may underestimate the degree of heat loss from man-made (apparent) wind and risk for cold injury due to seasonal temperature variation. Preexisting medical conditions interact with the environment, energy availability, clothing, and anthropometric measurements to determine a patient’s response to cold exposure (Table 1). 4
Adapted from Table 3 in ACSM position stand on prevention of cold injuries during exercise. 4 Adaptations are themselves works protected by copyright. So in order to publish this adaptation, authorization must be obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.
Hypoglycemia, various endocrine abnormalities, and low caloric intake decrease shivering response and heat production. 4 Increased total body heat loss can occur with chronic skin conditions, hyperhidrosis, and low percentage of body fat. Young children and those older than 60 years are at higher risk of cold injury. 4 The nervous and vascular systems are critical to thermoregulation and medications that modify these systems by decreasing a patient’s response time or increasing vasoconstriction may increase the risk of cold injury. Rayaud syndrome has been shown to impair thermoregulatory mechanisms, resulting in decreased blood flow to the digits during cold exposure and prolonged rewarming. 18 There is also evidence to suggest that athletes with previous frostbite injury have a 2- to 4-fold greater chance of repeat cold injury. 17
Cold environments can also worsen preexisting respiratory and cardiovascular diseases. Cold-induced broncho- constriction is common in cold weather athletes and patients with known asthma or exercise-induced asthma.4,19 Broncho- constriction is thought to be related to the low humidity and high respiratory rates found in cold conditions. 19 The change in airway temperature stimulates the release of inflammatory mediators resulting in edema, bronchospasm, and asthma-like symptoms. 20 The incidence of cardiovascular-related events increases with cold exposure likely from a cold-induced increase in mean arterial pressure, total peripheral resistance, cardiac work, and myocardial oxygen requirements during both rest and exercise. 4 ,21,22 Increased cardiac demand and arterial pressure in cold temperatures can increase risk for angina and other cardiac events.22,23 Cold water swimming has been shown to alter or mask a patient’s usual angina symptoms, also placing patients at greater risk.4,24
Preparticipation History
A good history screens for illnesses that increase risk of cold injury or can be worsened by cold exposures. Attention should also be given to patient education, preparedness, and expected environmental conditions. The average ambient temperature and daily range, average wind velocities, precipitation probability, immersion potential, and altitude will determine the baseline risk for cold injury. In addition, defining anticipated exertion level, duration of exposure, wilderness experience, and previous cold injury allows for further risk quantification and targeted education to decrease risk.
Example history questions include the following
25
: Have you been diagnosed with frostbite, hypothermia, or cold-related injuries in the past? If you have had previous cold injury or frostbite, do you develop symptoms or have problems with repeat exposure to cold? Do you smoke or use nicotine products? What medications are you using (paying special attention to central nervous system depressant and vasoconstrictive medications)? Do you have heart disease, angina, or a family history of heart disease? Do you cough, wheeze, or have difficulty breathing during or after exercise? Have you ever used an inhaler or taken an asthma medication? Do your symptoms get worse in the cold? Do you have diabetes or thyroid problems? How well is the condition managed? Do you have normal sensation in your hands and feet? Do you have Raynaud syndrome? How do you manage the symptoms? Do you have any chronic skin conditions such as psoriasis or eczema?
Preparticipation Physical Examination
The physical examination for a patient athlete before cold exposure should not differ greatly from the normal preparticipation physical examination. 25 The examination should include a general assessment of age, gender, and percent body fat (if suspected low) as these factors affect cold tolerance. Specific attention to cardiovascular, peripheral circulation, respiratory, thyroid, skin, and neurological examinations is important to define abnormalities that may predispose to cold injury. Consider cardiac stress testing for individuals at elevated risk for cardiovascular disease.
Clearance: Risk Factor Modification/ Recommendations
The preparticipation examination provides the perfect opportunity to educate patients on specific risk factors and prevention of cold injuries. For all cold injuries, the best treatment is prevention. Preparation for environmental exposures is extremely important.
Proper layering of clothing can help maintain adequate core temperature and decrease heat loss in cold weather. The innermost layer, which is in direct contact with the skin, should not retain moisture, but rather wick moisture away from the body to maintain an insulating air layer next to the skin and transfer water to outer layers of clothing. 4 The exception to this is wool, which can retain heat even when wet. The middle layer or layers are primarily for insulation and should be made of a material such as fleece or wool. The outer layer must allow moisture transfer, allow ventilation, and protect against wind and rain. 4 Layering allows the athlete to find a balance of warmth while preventing sweat during periods of exertion. Clothing needs will change with the ambient temperature, wind chill, and exertion level. As the level of exercise intensity increases, the amount of clothing insulation needed to maintain body heat at a given temperature decreases. Clothing needs vary among individuals, so athletes should be encouraged to individualize appropriate dress and layering according to their experience during previous cold exposure and training. 4 The risk of hypothermia increases in wet conditions, making dry clothing essential. It is important for athletes to realize that most “waterproof” clothing is advertised as breathable, but exercise sweat rates easily exceed the breathability of many waterproof or water-resistant materials, which may become a vapor barrier that traps moisture next to athlete’s bodies. It is safe to assume that the more waterproof clothing is the less it will breathe.
Specific to frostbite is the recommendation to wear well-fitted clothing and boots. Frostbite injury occurs when tissue heat loss is too great for local tissue perfusion. 5 Clothing or footwear that is too tight can constrict peripheral blood flow leading to cooler extremities or digits.4,5 One common mistake is adding an extra pair of socks for added insulation, which may actually constrict blood flow and worsen the risk of frostbite injury. Chemical hand and foot warmers can be used to maintain peripheral warmth, but should not constrict blood flow. The importance of keeping the core and large heat-dissipating areas (eg, head, neck, armpits) covered and warm to prevent peripheral vasoconstriction and increased risk for cold injury to the distal extremity is frequently overlooked.
Caloric intake is also important in the prevention of cold injury. Energy expenditure can be 10% to 40% higher in cold environments, due to shivering response, heavy clothing, equipment, and/or increased work associated with walking in snow. 4 However, if the core temperature stays above resting values (heat production offsets heat loss), then cold exposure does not increase oxygen uptake or caloric requirements above normal for the exertion level. 4 ,26,27 If increased energy expenditure above baseline is expected, the increased calories can be obtained through frequent snacks during the day. While maintaining good hydration is important to maintain adequate performance, mild to moderate dehydration alone does not increase the risk of cold injury. 4
All athletes can respond to a changing environment, layer clothing appropriately, and maintain adequate nutrition and hydration. Recognizing the signs and symptoms of early frostbite can prevent worsening of the condition. Frequent cold checks during the athlete’s exposure is important to recognize early skin and/or behavior changes.
Summary and Conclusions
The following specific recommendations can be discussed with athletes who have been identified to have a higher risk of injury. Endocrine conditions, including thyroid disorders and diabetes, should be well controlled before cold exposure. Optimize management of all chronic dermatologic conditions. Consider changing vasoconstrictive medications to alternate classes. Avoid cigarette smoking, drugs, alcohol, and central nervous system–depressant medications. Prophylactic use of antiperspirants containing aluminum hydroxide can be used to decrease foot and hand sweating in patients with known hyperhidrosis, expected prolonged exposure to wet conditions, or previous nonfreezing cold injury such as trench foot.
4
Patients at risk for or with a history of previous trench foot should be encouraged to change socks frequently during exposure to cold and wet conditions. For patients with asthma or exercise-induced bronchocon-striction, ensure appropriate medication management and symptom recognition before activity. All patients at risk for cold-induced bronchoconstriction with or without asthma should have a B-2 agonist inhaler available.16,19 Patients with known coronary artery disease should use caution in cold environments. Must be able to recognize angina symptoms and alter activity as needed to reduce cardiac demand. Angina symptoms can be masked or altered by cold water immersion. Cold water swimming or immersion should be avoided.4,24 Use of a facemask warms and humidifies inhaled cold air, which has been shown to reduce the reflexive increase in blood pressure and can be considered in at-risk populations.
28
Raynaud syndrome should be managed through lifestyle changes and medication management if needed. Avoid cigarette smoke. Consider a calcium channel blocker (preferred initial treatment) or topical nitroglycerin (recommended with caution because of a high side effect profile).
29
Patients with a history or cold urticaria can be prophy-lactically treated with antihistamine medications and consideration should be given for a prescription epinephrine autoinjector for severe cases.9,10
Footnotes
The authors report no conflicts of interest.
This article appears in a “Care of the Wilderness and Adventure Athlete” special issue, jointly published by Clinical Journal of Sport Medicine and Wilderness & Environmental Medicine.