
Abstract
Jellyfish have a worldwide distribution. Their stings can cause different reactions, ranging from cutaneous, localized, and self-limited to serious systemic or fatal ones, depending on the envenoming species. Several first aid treatments are used to manage such stings but few have evidence behind their use. This review of the literature describes and discusses the different related first aid and treatment recommendations, ending with a summarized practical approach. Further randomized controlled trials in this field are needed.
Introduction
Jellyfish envenomation has become a serious health problem on coastal beaches throughout the world, but especially subtropical and tropical Atlantic, Pacific, Asian, and Australian coasts where the most notorious jellyfish species prevail. 1 Jellyfish are marine invertebrates belonging to the phylum Cnidaria, which is subdivided into 5 classes (Table 1): 1) Hydrozoa, which are not considered true jellyfish and include the Physalia species, which are siphonophores; the 2 major Physalias are Physalia physalis, known as the Portuguese man-of-war, and the Physalia utriculus, known as the Blue bottle; 2 2) Scyphozoa, the true jellyfish, include Cyanea capillata, known as the lion’s mane jellyfish, and Pelagia noctiluca; 2 3) Cubozoa, similar in form to the true jellyfish but more boxlike; 2 different orders are recognized: the large multitentacled chirodropids, which are among the most dangerous marine creatures and include Chironex fleckeri, known as the Australian box jellyfish, and the smaller 4-tentacled carybdeids, an example of which is Carukia barnesi (also known as an Irukandji jellyfish), which causes Irukandji syndrome; 2 4) Anthozoa are unique among cnidarians in that they do not have a medusa stage in their development; examples are soft corals and sea anemones; and 5) Staurozoa were conventionally considered to be an order in the class Scyphozoa, however, recent genetic studies suggested they should be elevated to class of their own; unlike most jellyfish, they do not have a free-swimming medusa stage, rather, the adult animal is a sessile polyp. 3 Species distribution varies geographically (Table 1). 4
Geographic distribution and characteristics of some cnidarian species 62
Cnidaria classically have bodies consisting of a jellylike substance enclosing the internal structures, from which structures called tentacles are suspended. Each tentacle is covered with thousands of cells called cnidocytes or nematocytes that house an organelle called a cnidocyst or nematocyst containing stinging barbed threads or tubules. Mechanical or chemical stimulation, or both, causes a large concentration gradient of calcium across the cnidocyte plasma membrane. The resulting osmotic pressure leads to water influx and increased pressure inside the nematocyst, causing the threads to uncoil and spring out like tiny darts firing venom into the victim. 5 These venoms differ in composition, biological activity, and potency among different species. Jellyfish venoms are complex and could be composed of potent proteinaceous cell membrane pores forming toxins, neurotoxic peptides, bioactive lipids, catecholamines, histamine, hyaluronidases, fibrolysins, kinins, phospholipases, and various hemolytic, cardiotoxic, nephrotoxic, myotoxic, and dermonecrotic toxins. 2 ,6–8 Both the venom components and the tubule biopolymers can initiate different types of immunological responses—innate, adaptive, immediate, or delayed hypersensitivity reactions—that can be amenable to anti-inflammatory and immunomodulatory treatment. 9 Thus, analyzing each species-specific venom allows for appropriate and effective treatment. 9
Methods
A review of the literature was performed to describe the different reactions to jellyfish stings and to point out the related evidence-based preventive and therapeutic management.
Reactions To Jellyfish Stings
In general, reactions to jellyfish stings vary from the usual nonsystemic, localized skin reactions to the rare systemic life-threatening ones, depending on the species of the envenoming organism, the duration and extent of exposure, the number of nematocysts discharged, affected body area, location and thickness of affected skin, health, weight, age, and reaction of the host to envenomation, and the initial treatment administered.10,11
Local and immediate skin reaction occurs within minutes to hours at the site of the sting and is mainly related to the toxic effect of venom. This reaction is the most common presentation of a jellyfish envenomation. 12 Classically, the lesions are linear, urticarial, painful, and erythematous at the areas of tentacular contact. 12 A few days later, the lesions can become vesicular, sometimes hemorrhagic, and even necrotic or ulcerative in certain cases, as in Chironex fleckeri stings. 5 ,12–14 Regression and resolution of the blisters and pruritus may take as long as 10 days; however, mild hyperchromia and slight roughness in skin texture may still be observed for as long as 8 months after the sting. 11 The pain is mainly due to the effect of exogenous or endogenous mediators such as kininlike factors on cutaneous nerves. 12
Generalized skin eruptions or eruptions distant from the primary sting have been reported and are probably secondary to a hypersensitivity response to the antigenic component of the venom. 12 Recurrent skin eruptions involving the sites of the primary lesions may occur and usually consist of erythematous, pseudovesicular, urticarial papules with mild edema (histology: spongiotic vesiculation, dermal edema, and perivascular lymphohistiocytic infiltration 15 ). These eruptions might be due to the body reacting to the persistent stinging cells as antigen depots that keep on releasing the venom after some chemical or mechanical stimulation.14,15 Persistent eruptions as well as delayed (allergic) eczematous reactions have been also observed. A delayed reaction usually develops days to months after exposure. It is postulated that such a delayed reaction is the result of a type IV immunopathogenetic mechanism, in addition to the more frequent type I mechanism, with a central role played by Langerhans cells and T-helper lymphocytes. 5 ,12,14,16
Other nonsystemic reactions such as pigmentary changes, lichenification from persistent rubbing, keloids, granulomas, localized hyperhydrosis and lymphadenopathy, fat atrophy, vasospasm and subsequent limb atrophy, necrosis, gangrene, and contractures have been reported. 12 ,17,18 Conjunctivitis, eyelid edema, chemosis, and corneal ulcerations may occur when tentacles contact eyes. In certain cases, eye or corneal stings can lead to severe iritis and increased intraocular pressure or chronic glaucoma, sometimes even years after the sting. Sneezing and rhinorrhea could be associated.19,20 Severe dyspnea and upper airway obstruction may be caused by stings to the face. 21 An itchy dermatitis, called seabather’s eruption, on parts covered by the swimsuit has been described in certain areas (Florida, Caribbean, New York). It is attributed mainly to jellyfish larvae that get trapped between the skin and the swimsuit. Owing to persistence of nematocysts in the suit, recurrence of this reaction may occur with wearing the suit again. 22
Systemic reactions may occur in addition to the above reactions, particularly due to envenomation with certain species of jellyfish. These reactions may be due to direct action of the venom on the heart, liver, kidney, and nervous system 10 or to severe allergic reactions (early and late), although angioedema and anaphylaxis due to jellyfish stings are considered rare. 17 Irukandji syndrome is a serious systemic reaction caused mainly by a Carukia barnesi sting. It is characterized initially by mild to moderate, tolerable pain followed in 20 to 30 minutes by severe generalized pain and muscle cramping in the abdomen, chest, head, back, and limbs that becomes associated with autonomic features such as nausea, vomiting, profuse sweating, restlessness, and excessive shaking followed by pyrexia, tachyarrhythmias, and hypertension. In cases of severe toxicity, life-threatening hypertension and hyperkinetic cardiogenic shock, pulmonary edema, or a cerebrovascular accident may occur.17,23 Myocardial injury with or without pulmonary edema may ensue 4 to 18 hours after the sting.24,25
Stings by large adult Chironex fleckeri (Indo-Pacific or Australian box jellyfish), are reported to be the most toxic and dangerous jellyfish stings in the world. Severity of the injury depends on the size of the jellyfish and the extent of tentacle contact. 7 The sting results initially in a localized severe painful reaction followed by superficial ulceration, necrosis, and full-thickness necrosis in 1 to 2 weeks. Initial systemic reactions include headache, malaise, fever, nausea, vomiting, muscle spasm, pallor, respiratory distress, hemolysis, and acute renal failure. Death may also occur, and is the result of either drowning secondary to muscular spasm after envenomation or quick respiratory and cardiac arrest (in minutes) due to the spreading of the venom to the circulatory system. 17 ,26,27
Other species also have the potential to cause serious reactions. A case of Tako-Tsubo cardiomyopathy 28 and a case of proven anaphylaxis 17 have been reported as induced by the common Mediterranean jellyfish Pelagia noctiluca. Case reports of mononeuritis multiplex, 29 Guillain-Barre, 30 and acute myocardial infarction 31 have been mentioned as a result of some other jellyfish stings.
Treatment
Prevention and proper management play important roles in minimizing discomfort and complications after jellyfish envenomation. However, the evidence behind the currently recommended therapy is relatively weak.2,32 The best preventive measure is to avoid any contact with seawater during the time jellyfish are invading. 33 Wearing a full-body Lycra stinger suit or equivalent provides good protection from stings.7,34 If stinger nets are used, they should be of less than 0.25 mm mesh size to provide enough protection against small jellyfish (eg, Irukandji) tentacles.33,34
Sufficient application of a topical sting inhibitor such as Safe Sea lotion (a waterproof sunscreen containing octyl methoxycinnamate and zinc oxide that has been reported to mimic the mucous coating used by clown fish to inhibit sea anemones stings) will also be helpful for swimmers at high risk of exposure to jellyfish as it has been demonstrated to significantly decrease the frequency and severity of stings.35,36 Thick layers of petroleum-based ointment are reported to be effective as well. 17 Moreover, it is important to avoid touching jellyfishes or their parts on the beaches because they often contain nematocysts that can discharge and sting. 37
First Aid Measures
The literature published on the treatment of jellyfish stings is limited, conflicting, and lacks consensus. Guidelines are available from the Australian Resuscitation Council (ARC) 38 and from the International Life Saving Federation (ILSF). 39 Generally, recommendations vary between tropical and nontropical areas with the variations in the geographic distribution of life-threatening and non–life-threatening jellyfish species,38,39 hence the importance of species identification, which at many times is not feasible.
In case of jellyfish stings, management consists of the following steps: 1) Rescue the victim from the water as soon as possible to avoid further contact with jellyfish tentacles and to prevent drowning. 38 The victim should be prevented from rubbing the stung area,38,40 as that may enhance discharge of nematocysts on the victim’s skin. Reassuring the victim helps reduce the skeletal muscle pump activity that panic brings. 17 It is advised that rescuers wear protective clothing and gloves so they can better rescue and treat the victim. 2) As per ARC guidelines, in case of tropical jellyfish (Chironex fleckeri and Carukia barnesi) stings that are life-threatening, the primary objective of the first aid treatment is to preserve life. Calling an ambulance is a must, and commencing basic life support for victims with cardiac arrest and injecting epinephrine as soon as possible may be needed for the rare cases with anaphylaxis. 38 Shortly after the sting, intravenous (or in field, intramuscular) administration of antivenom available for severe Australian box jellyfish (Chironex fleckeri) stings may also be required (Table 2). 7 ,10,26,38 There are significant concerns, however, regarding the efficacy of the antivenom in reversing the neurotoxic and myotoxic effects of the venom. 6 Magnesium sulfate, which has been reported to improve the effectiveness of the antivenom, may be added for victims of Chironex fleckeri with severe cardiovascular effects who did not respond to advanced life support (Table 2). 7 ,10,38,41 Magnesium has traditionally been used for the treatment of Irukandji syndrome; however, according to a recent randomized trial, its use needs to be reconsidered until there is good evidence to support it, as it did not demonstrate benefit. 42 Thereafter, the aim of first aid management consists of deactivation of undischarged nematocysts, inactivation of the toxin, and control of the pain.10,38
Deactivation of Undischarged Nematocysts
Most studies agree that regardless of the stinging species, fresh water should not be applied as first aid as it can induce nematocyst discharge by osmosis. 10 ,38–40,43,44 Seawater can be used to wash tentacles off affected areas. 38 ,40,44 Some of the chemicals traditionally used as home remedies to treat jellyfish stings in humans include acetic acid (vinegar), ethanol (liquor, perfume), ammonia or urea (urine), sodium bicarbonate (baking soda), papain (meat tenderizer), aluminum sulfate, and salt water. Applications up to 15 to 30 minutes have been mentioned. However, no evidence on the effectiveness of most of these treatments exists because of unavailability of randomized controlled trials. The type of first aid application used and its effectiveness seem to also vary with the species of jellyfish causing the envenomation.
A study comparing the effect of various chemicals on discharge and pain caused by jellyfish nematocysts revealed that the application of ethanol, meat tenderizer, ammonia, or vinegar (acetic acid 4% to 6%) stimulates nematocyst discharge of some species such as Physalia physalis, particularly those living in Australian waters, 2 ,43–46 and provides little or no relief from the pain. 44 Similarly, vinegar has a stimulation effect on nematocysts of Cyanea Capillata (Lion’s mane), Lytocarpus philippinus, 44 –47 and Chironex fleckeri (Australian box jellyfish). Also, despite being recommended by the ACR, 38 vinegar was recently discovered to increase the venom load in victims of Chironex fleckeri by 50%. 48 Immersion of the stung area with vinegar (acetic acid 4% to 6%) for at least 30 seconds, a practice commonly used on stings of two carybdeid cubozoa, Carukia barnesi (causing Irukandji syndrome38,49) and Carybdea alata 46 (Hawaiian box jellyfish), inhibits nematocyst discharge, but there is no clear evidence to support this tradition. Moreover, vinegar was shown to reduce nematocyte discharge and pain in case of Pelagia noctiluca sting in the Mediterranean Sea.50,51
Although debatable, considering the new evidence about vinegar on Chironex fleckeri, 48 it has been reported that if vinegar is not available, then cola soda or old wine with pH similar to vinegar may have moderate beneficial effects on the Chironex fleckeri (Australian box jellyfish) stung area. 49 A paste made of baking soda and seawater (50% baking soda, 50% seawater) has been recommended for Cyanea capillata (lion’s mane jellyfish), sea nettles (Chrysaora sp), and most common American Atlantic jellyfish located north of Norfolk, Virginia,17,50 but there seems to be poor evidence to support this recommendation. 52 Lidocaine solutions in 4% to 15% concentrations may be the alternative as it acts as a local anesthetic and can have an effect on the calcium ion channels in the nematocyst membranes hindering discharge.44,50 Methylated spirits and alcohols, ammonia, urine, and meat tenderizer should never be used for such stings, as they stimulate nematocyst discharge. 38 ,40,44,49
Removal of Tentacles
The next step in first aid treatment entails the removal of the remaining clinging tentacles and nematocysts. It has been recommended to cover the area with shaving cream, talc, flour, a paste of seawater with baking soda (50% baking soda, 50% seawater), or even dry sand, and then removing the tentacles using a knife, forceps, tweezers, a sharp instrument like a plastic object (eg, a credit card), or manually while wearing rubber gloves, but never bare hands.10,43 However, these practices seem to lack evidence. The ARC and the ILSF guidelines based on a book published by Williamson et al 53 in 1996 mentioned that vinegar-treated tentacles of the box jellyfish may be removed with safety, and if vinegar is not available, the tentacles may be picked off safely by the rescuers because only harmless prickling may occur on the fingers of the rescuer 18 ,38,39 owing to thickness of skin in this area. The ILSF reported, however, that the hands of the rescuer should be washed as soon as possible as stinging cells remain on the hand and can sting more sensitive areas of the body, such as eyes. 39
Pain Control
Controversy also exists regarding the immediate analgesic therapy to be used. Exton et al, 45 in their uncontrolled retrospective case series, observed that pain relief for Cyanea capillata (lion’s mane jellyfish), Physalia physalis (Portuguese man-of-war), and small box jellyfish stings was best obtained by application of cold packs. Conversely, a randomized study later showed that more relief of pain was obtained after 10 minutes of warm water immersion (45°C, with care not to exceed that because of increased risk of scalding) rather than with cold packs application onto Physalia physalis (Portuguese man-of-war) stings. This effect was more accentuated after 20 minutes. 53 This finding confirms the results reported in two previous randomized trials done as well on Physalia stings in Australia and in Florida in the United States.54,55 In case of Carybdea spp (Irukandji jellyfish) stings, Taylor et al 56 also demonstrated in a small trial involving volunteers that hot water (45°C) immersion was the only successful local analgesic compared with ice, vinegar, and aluminum sulfate. Furthermore, in case of a Carybdea alata (Hawaiian box jellyfish) sting, hot water may relieve pain better than cold packs.57,58 This finding was commensurate with the results of a recent systematic review, in which there was a good level of evidence that hot water provided for pain relief of such stings. 59 A few studies reviewed advised against the use of hot compresses, however, particularly in case of Chironex fleckeri (Australian box jellyfish) stings as they can increase systemic absorption of the venom. 10 ,38,60
As per ARC, for Physalia and other nontropical jellyfish, whose stings are less life-threatening, the primary objective of the first aid treatment is to relieve pain. The ARC recommends rinsing the sting area well with seawater to remove invisible nematocysts, then placing the stung area in hot water (45°C) for 20 minutes. If local pain is unrelieved by heat or if hot water is not available, a cold pack or ice in a dry plastic bag may be applied.38,45 For tropical jellyfish, particularly in case of Chironex fleckeri (Australian box jellyfish) stings, cold compresses are recommended by ARC for analgesia. Pain relief after hot water immersion is probably through heat inactivation of the jellyfish toxin or through modulation of pain receptors in the nervous system.61,62 It is worthwhile to mention that heat therapy should be provided either by means of an accurately controlled hot shower or hot water immersion in a thermal isolator, because the hot water temperature decreases to suboptimal range after 5 minutes in a conventional metal tray and after 15 minutes in a sharp box. 63 Water temperature should be tested by adults before use on children. 59
Other traditional home remedies such as ethanol and ammonia seem to be ineffective in decreasing pain from jellyfish stings. 44 ,46,58 Stingose (an aqueous solution of 20% aluminum sulfate and 1.1% surfactant) has shown evidence as an effective pain killer for Physalia stings. 2
Analgesics (systemic or oral) and even narcotics such as fentanyl or morphine may be necessary, for example, in cases of Irukandji syndrome 63 or severe skin pain in stings of tropical water jellyfish, mainly, Chironex fleckeri (Australian box jellyfish). 2 In other cases, simple oral analgesics such as ibuprofen or acetaminophen are recommended, taking into consideration that they require at least 40 minutes to become effective. 17
Subacute Treatment
For a few days after a sting, the stung area should be cleaned regularly, and topical antibiotics that are effective against marine pathogens, such as chloramphenicol or erythromycin, should be applied. 10 Some researchers state that local antibiotics are not necessary because secondary infection is rare. 17 Antihistamines, prostaglandin inhibitors (nonsteroidal anti-inflammatory drugs), and topical or systemic steroids may be used in case of more severe persistent local reactions if infection is not present. Tetanus prophylaxis may be considered, as well as systemic antibiotics in case of secondary infection.10,43 However, no evidence exists regarding such treatments.
Hemorrhagic bullae may be punctured but the roof left intact and treated as a local wound. 17 Incision and drainage of fluctuant lesions may be necessary. 17 Granuloma annulare often remits with occlusive potent topical corticosteroids. 17 A localized granulomatous reaction should respond to intralesional corticosteroids. 17 Nonresponding, delayed, persistent, or recurrent cutaneous reactions can be managed with topical steroids. 14 In intractable cases, topical immunomodulatory drugs (tacrolimus and pimecrolimus) can be used as a second line treatment. 5 They do not seem to prevent relapses, however.5,15
Conclusion
Depending on the envenoming species, reactions to jellyfish stings vary from the common skin reactions to the less common, serious, or even fatal ones. Consensus is lacking regarding the first aid treatment after jellyfish sting because of limited data to make evidence-based recommendations. Many of the popular first aid treatments lack evidence to support their use. Pending further studies in this field, we suggest following the flowchart provided in the Figure.
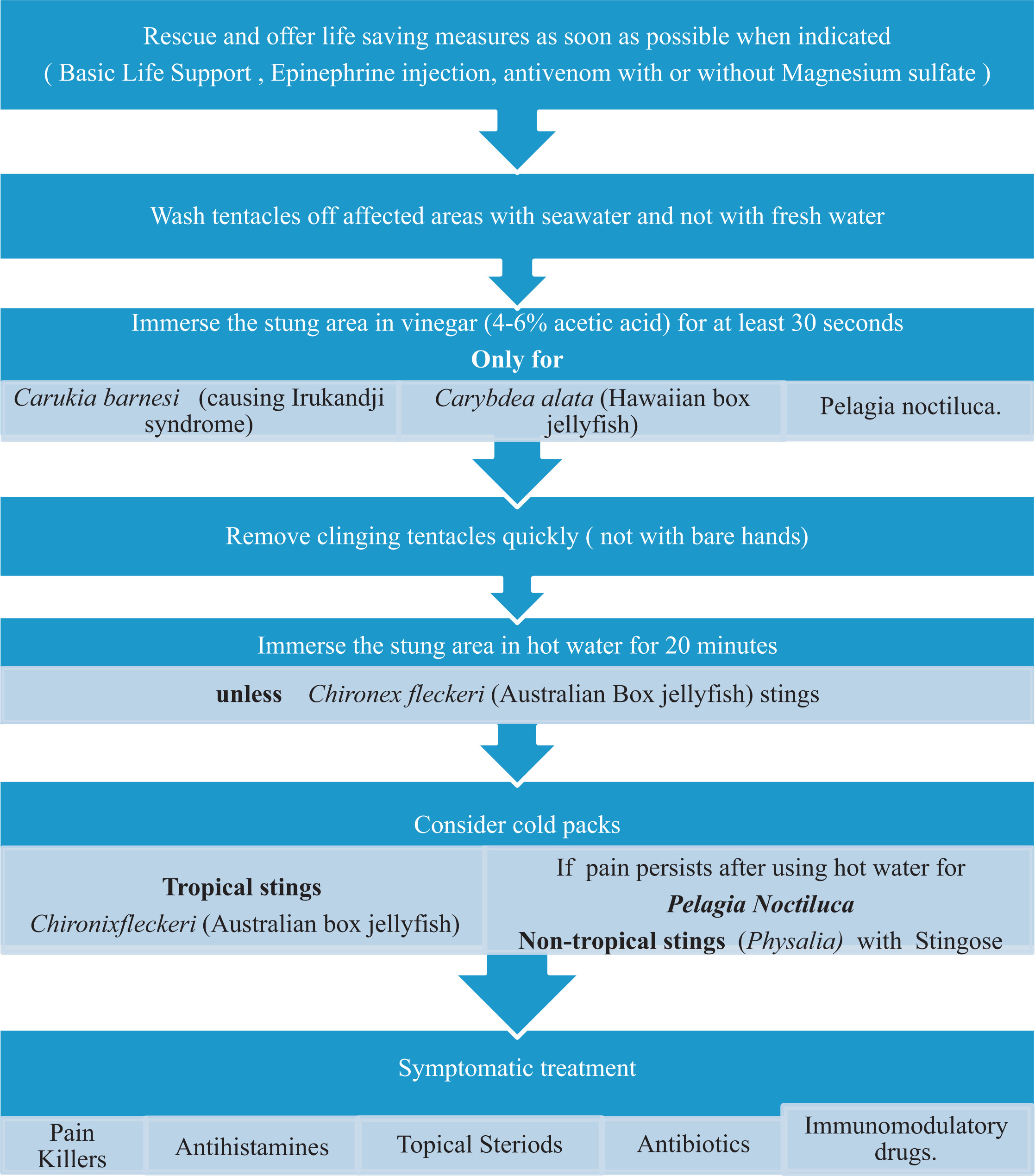
Jellyfish sting management flowchart.
Disclosures
The authors report no financial or other conflict of interest.