
Abstract
Objective
To review the presentations of a series of patients with suspected Irukandji syndrome in the Torres Strait, where the syndrome has hitherto been unknown or undocumented, in order to identify at-risk groups and improve the management of this condition in the region.
Methods
A mixed retrospective-prospective review of eight cases of patients with suspected Irukandji syndrome in the Torres Strait, with a focus on the differences between the clinical presentations and patient outcomes.
Results
Irukandji syndrome is the most likely explanation, based on current knowledge, of this series of marine envenomation syndromes in the Torres Strait. The syndrome appears to be more common in the monsoon season and young, Torres Strait Islander males likely represent a high-risk group in the region.
Conclusions
The Torres Strait can be added to the growing list of regions where Irukandji syndrome has been documented. The clinical picture, including time to onset of symptoms, constellation of symptoms and signs, analgesic requirement and time to recovery, can differ markedly between patients. There is a need for health promotion and education of health staff and the public regarding the risks, symptoms and signs of this condition. There is also a clear need for the use of case definitions and standardised management approaches for Irukandji syndrome, while the health community awaits the results of ongoing research into the pathophysiology and improved treatments for this interesting but dangerous tropical marine envenomation syndrome.
Introduction
Irukandji syndrome describes a characteristic clinical presentation following envenomation by a member of the group of tiny carybdeid (also known as Cubozoan, or box) jellyfish which inhabit tropical waters. The syndrome typically occurs 5 to 60 minutes following delivery of venom via nematocysts (an organelle within the nematocyte, or stinging cell) into the skin following contact with the jellyfish in seawater. 1 The clinical presentation is characterized primarily by pain, which can remain localized to the sting site or become generalized and widespread, and can be highly variable in nature.1,2 Other common features include distress, agitation, and signs of a hypercatecholaminergic state such as tachycardia, hypertension, diaphoresis, and piloerection.3,4 Other common features include muscle cramps, nausea, vomiting, and headache. 4 Many patients require parenteral opioid analgesia; severe cases may be complicated by cardiomyopathy, pulmonary edema, and intracerebral hemorrhage.1,5 Intensive care is occasionally required and 2 deaths have been reported in Australia. 5
The syndrome was first described in North Queensland by Flecker in 1952, who named it after a local indigenous tribe. 3 The first organism to be conclusively proven to cause the syndrome was Carukia barnesi, after Barnes' infamous experiment in 1961 in which he envenomed himself, a lifeguard, and his young son (all 3 survived). 4 Since that time, the majority of reported cases have been from the North Queensland region;2,5 large case series analyses have also been performed in Darwin in the Northern Territory 6 and in Broome on the northwest coast of Western Australia. 1 There have been isolated case reports of an “Irukandji-like syndrome” from other tropical regions such as Thailand, Hawaii, Florida, and the Caribbean, 6 and it is suspected that organisms other than C barnesi may be implicated. 6 -9
We report a series of 8 cases of suspected Irukandji syndrome in the Torres Strait Islands—an equatorial archipelago with a predominantly Melanesian population that lies between the northeast tip of the Australian continent and Papua New Guinea (see Figure).
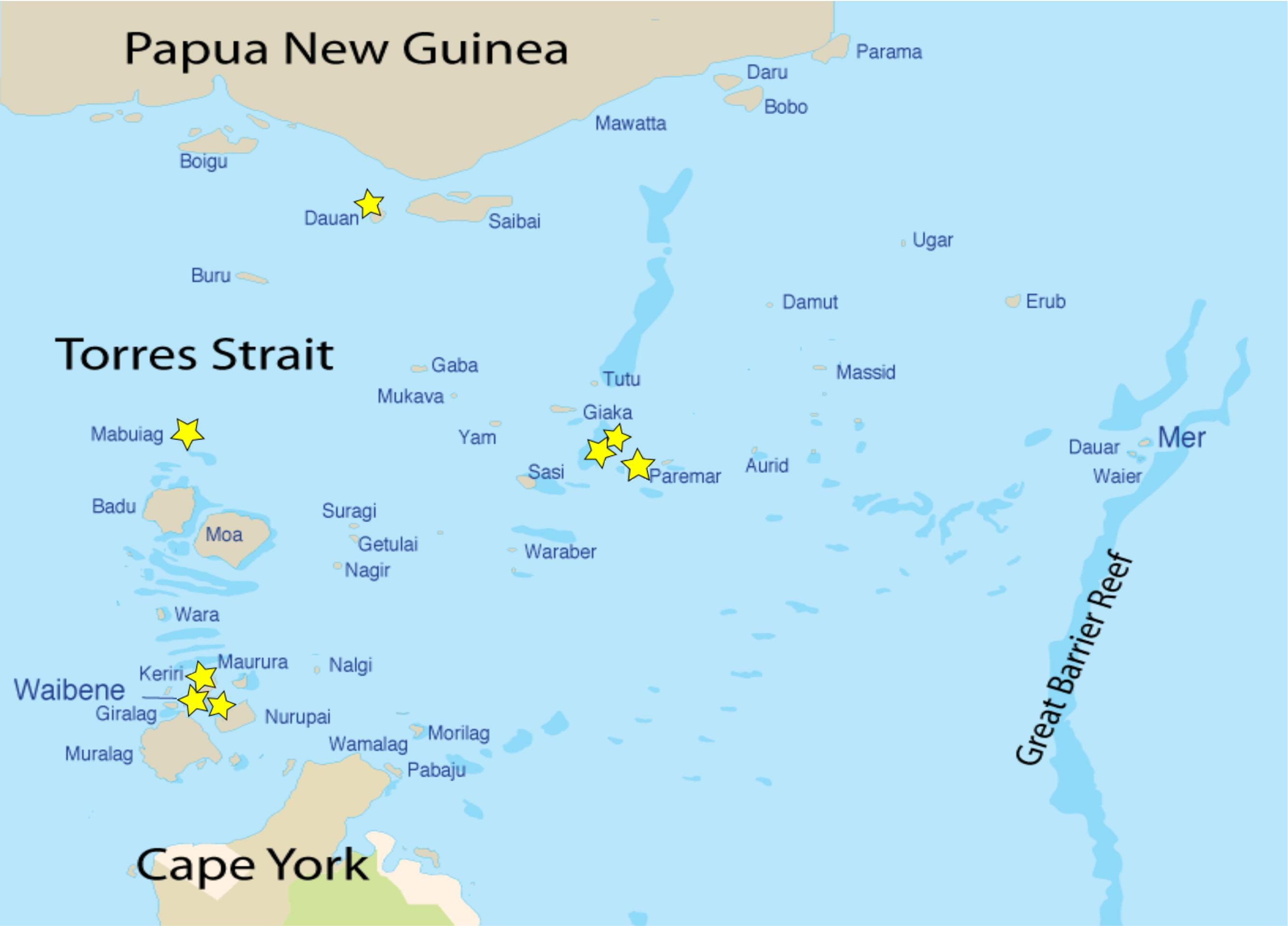
Torres Strait Islands with locations of cases indicated by stars.
Summary of Cases
The features of the 8 cases are displayed in the Table. Seven cases were young males, ranging in ages from 4 to 25, the other was a 29-year-old female. Six cases were swimming in shallow water at a beach, the other 2 were both crayfishermen (who dive for crayfish/lobster using a breathing apparatus connected to a boat on the surface) diving on an offshore reef; the latter 2 cases were envenomed in the same location on the same day. Three of the cases occurred on Waiben (Thursday Island), the administrative center for the Torres Strait Islands and the most populous island in the region. All cases occurred during the “wet” or monsoon season that, in the Torres Strait, is characterized by hot, wet, humid conditions with less wind than during the “dry” season. An attempt was made to document the prevailing environmental conditions for each case (temperature, humidity, winds, tides) but the data collected by the Australian Bureau of Meteorology was either incomplete or not available for all locations, and there was no discernible pattern in the available data, so this information was not included in the final analysis.
Features of cases of suspected Irukandji syndrome
TSI, Torres Strait Islander.
The time to onset of symptoms ranged from almost instantaneously to nearly an hour post-sting. All cases experienced pain, which tended to start locally (at the presumed envenomation site, which was exposed skin on the limbs in most cases and in the lower abdomen in one case) and then became generalized. Half of the patients had a visible welt at the presumed envenomation site; it was not clear whether this welt was due to contact with the tentacle or the bell of the organism. The majority of the cases also experienced either tachycardia or hypertension, or both. Three patients had mildly elevated cardiac enzymes (normal range: troponin <0.04 μg/L; creatinine kinase, CK: <198 U/L) and one had anterior T-wave inversion on electrocardiogram (ECG). All but one of the cases required opioid analgesia, in the form of either oral codeine, intravenous (IV), or subcutaneous morphine; doses of morphine ranged from 2 mg to 20 mg. Only one patient received IV magnesium, with some improvement in pain but no affect on hypertension.
Discussion
As case reports of Irukandji syndrome and Irukandji-like syndrome have accumulated around the world, our understanding of the causative organisms, predisposing climatic conditions, pathophysiology of clinical presentations, optimal management strategies, and preventative measures has slowly improved. It seems likely that new organisms will continue to be implicated and identified, as previous studies in Broome, Darwin, and Cairns have suggested, and as laboratory identification techniques improve. 6 -9 Performing skin scrapings from the presumed envenomation site for patients with Irukandji syndrome has yielded some positive results in terms of identification of causative organisms, however this technique requires the presence of specially skilled laboratory personnel trained in the identification of marine organisms (whole or in parts) via microscopy. 6
Given the regional variability, it is important that patients and health staff in tropical locations are aware of the potential threat posed by jellyfish in their regions, including envenomation syndromes, and have an understanding of the variety of clinical pictures with which envenomed patients can present.
This clinical variability has doubtless contributed to the difficulties in formulating a solid evidence-based management approach to Irukandji syndrome. Common initial therapeutic measures include the application of topical vinegar—this practice is widespread in Australia as a first aid measure for box jellyfish (Chironex fleckeri) envenomation (to inactivate undischarged nematocysts) but, since the initial sting in Irukandji syndrome often goes unnoticed, the application of vinegar—if employed at all—is often delayed. 6 Most patients who present to the hospital with recognized Irukandji syndrome receive some form of analgesia. 2 The quantity and class of the analgesic depends on the severity of pain; there is a lack of evidence surrounding the ideal dose and efficacy of the different formulations of opioid analgesics in this context.2,6 Other therapies commonly employed in Irukandji syndrome include antihypertensives (such as glyceryl trinitrate) 2 and magnesium sulphate.10,11 The role of magnesium in treating Irukandji syndrome (given its proven efficacy in other hyperadrenergic conditions such as pregnancy-induced hypertension and pheochromocytoma) is the subject of ongoing research; with mixed results in the literature so far, its use remains (for the moment) based on theoretical and anecdotal evidence pending the outcomes of current and future randomized controlled trials.10,11
The importance of health staff education and the value of local protocols was demonstrated in an Australian study of 34 health facilities in which clinicians' recognition of the syndrome and knowledge of appropriate management strategies was assessed. Deficiencies in both areas were identified, along with a lack of management guidelines in remote locations. 12 Comparison of these cases in the Torres Strait, with other cases described in series elsewhere in Australia, reveals similar trends in terms of clinical presentations and requirements for opioid analgesia, suggesting that case definitions for Irukandji syndrome are a useful tool in diagnosis and management of marine envenomations.
Now that it has been recognized that the syndrome occurs in the region, and given the lack of a standardized approach to the management of these cases in the Torres Strait, it is recommended that the 2 hospitals and 17 primary health care centers within the district employ case definitions and protocols for Irukandji syndrome.
Conclusions
These 8 cases represent the first published reports of suspected Irukandji sydrome in the Torres Strait Islands, where young males swimming or diving during the monsoon season appear to represent a high-risk group. With the established importance of local protocols, the need for patients to be aware of the risk, and the requirement that health staff be cognizant of the variability in presentations and main treatment modalities for Irukandji syndrome, we believe we are adding important information to the growing body of work on this interesting but potentially lethal tropical condition.