
Abstract

To the Editor:
In 2011, the Centers for Disease Control and Prevention reported approximately 25.8 million children and adults in the United States were affected by diabetes mellitus, making diabetes one of the most prevalent chronic diseases in our population. 1 Although people with type 1 diabetes mellitus (DM1) constitute a small percentage of this population, the majority of them are involved in various levels of athletic activities, including endurance sports. 2 The American Diabetes Association published a position statement in 2004 reinforcing the fact that persons with DM1 can participate in all levels of activity granted that they have no complications of their diabetes and are in good glycemic control. 3 Subsequent to this position statement, there have been a few articles discussing the recommended management of glycemic control in diabetic patients participating in endurance sports. 2 –4 However, only a few papers have reported case series of athletes with DM1 in endurance and ultraendurance sports. 4 –6 The purpose of the present study was to report the number and performance of athletes with DM1 who participated in the Leadville 100 races.
The Leadville 100 consists of a 161-km mountain bike race and a 161-km ultramarathon in Leadville, Colorado, in August of each year. The courses range in altitude from 2800 m to 3840 m, and the majority are on forest trails with some mountain roads.
7
The Leadville 100 mountain bike race starts at 6:30
From 2011 to 2013, a total of 7215 athletes competed in the Leadville 100 races. Of these, 5194 athletes (4851 mountain bikers and 2364 runners) were able to successfully complete the races (72%). Nineteen athletes reported having DM1. Only 2 runners with DM1 started the race more than once (2011 and 2012, and 2012 and 2013). Both runners who were not able to finish the race on their first attempt were able to successfully complete the race the next year. The other 15 athletes with DM1 only participated once during the 2011–2013 period. The Figure illustrates the comparison of athletes with DM1 to all other athletes. The majority of the participants with DM1 were male, with average age of 39 years (range 22 to 61 years). The majority (68.4%) of athletes with DM1 were able to successfully complete the race. The average finish time for mountain bike and run for DM1 athletes, respectively, was 10 hours, 36 minutes (range 8 hours, 44 minutes, to 11 hours, 45 minutes), and 27 hours, 54 minutes (range 24 hours, 45 minutes, to 29 hours, 52 minutes). Because of the small number of athletes with DM1, including or excluding them from the entire population did not change any statistics (eg, completion rate). There was no statistically significant difference for successfully completing the races between athletes with DM1 and all other athletes (odds ratio 0.84; 95% confidence interval, 0.32 to 2.22).
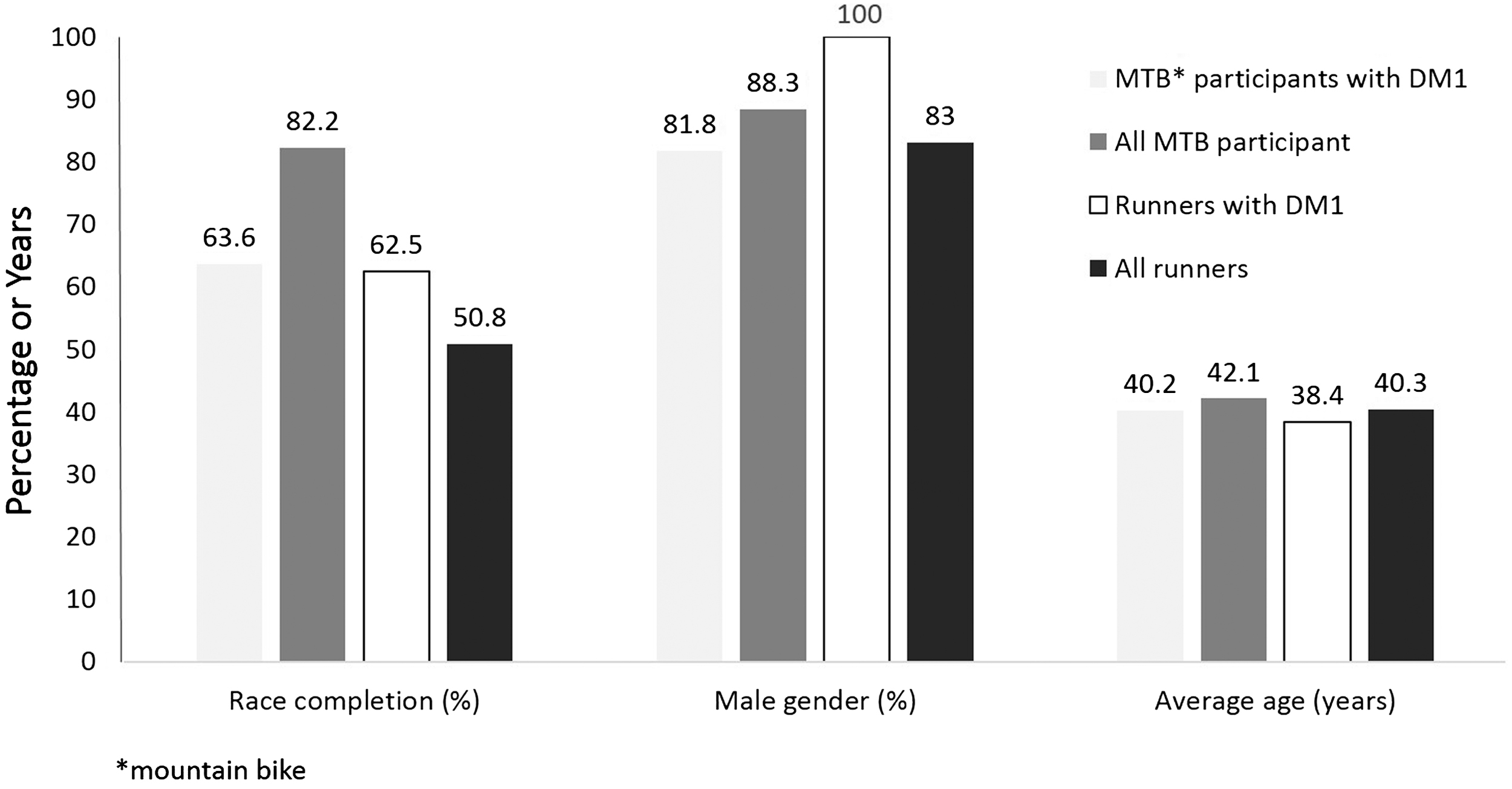
Athletes, both runners (open bars) and mountain bike (MTB) participants (shaded bars), with type 1 diabetes mellitus (DM1) were compared with all 2011–2013 Leadville 100 race participants (solid bars).
Ultraendurance events are growing in popularity. It is inevitable that athletes with chronic diseases, including DM1, who desire to push their limits will be encountered. In the retrospective, self-reported enrollment data from an ongoing longitudinal observational study, 0.7% of ultramarathon runners reported having diabetes (type of diabetes was not reported). 8 There have been only a handful of reported cases of athletes with DM1 who completed endurance races. 5 ,6,9,10 This number is much smaller for ultraendurance races.5,6 To our knowledge, this is the largest number of reported athletes with DM1 who participated in 161-km mountain bike and run races. It appears that athletes with DM1 are able to compete in ultraendurance events. Owing to its retrospective nature, our report has limitations connected to this type of study. When planning medical coverage for these ultraendurance events—which frequently have remote, difficult-to-access courses over a single track, mountain passes, and densely wooded areas—medical teams should be prepared to manage unusual, but serious circumstances such as hypoglycemia. 11 Many athletes with DM1 use insulin pumps and frequent or continuous glucose monitoring to stay on top of their insulin and caloric needs, and they can complete these ultraevents with few issues. However, that should not be assumed, because often athletes with DM1 are not aware of guidelines on how to manage glycemic fluctuations during long exercises and can run into serious problems with glycemic control. 4 Close glycemic and dietary monitoring before and during the race is the key to avoid complications. 12 Further prospective studies focusing on metabolic and physiologic changes as a result of these extreme exercises among athletes with DM1 are required.
Footnotes
Acknowledgments
We would like to thank Mr Joshua Colley and Lifetime Fitness for allowing us to conduct this study, and we also thank our study participants.