
Abstract
Case Presentation
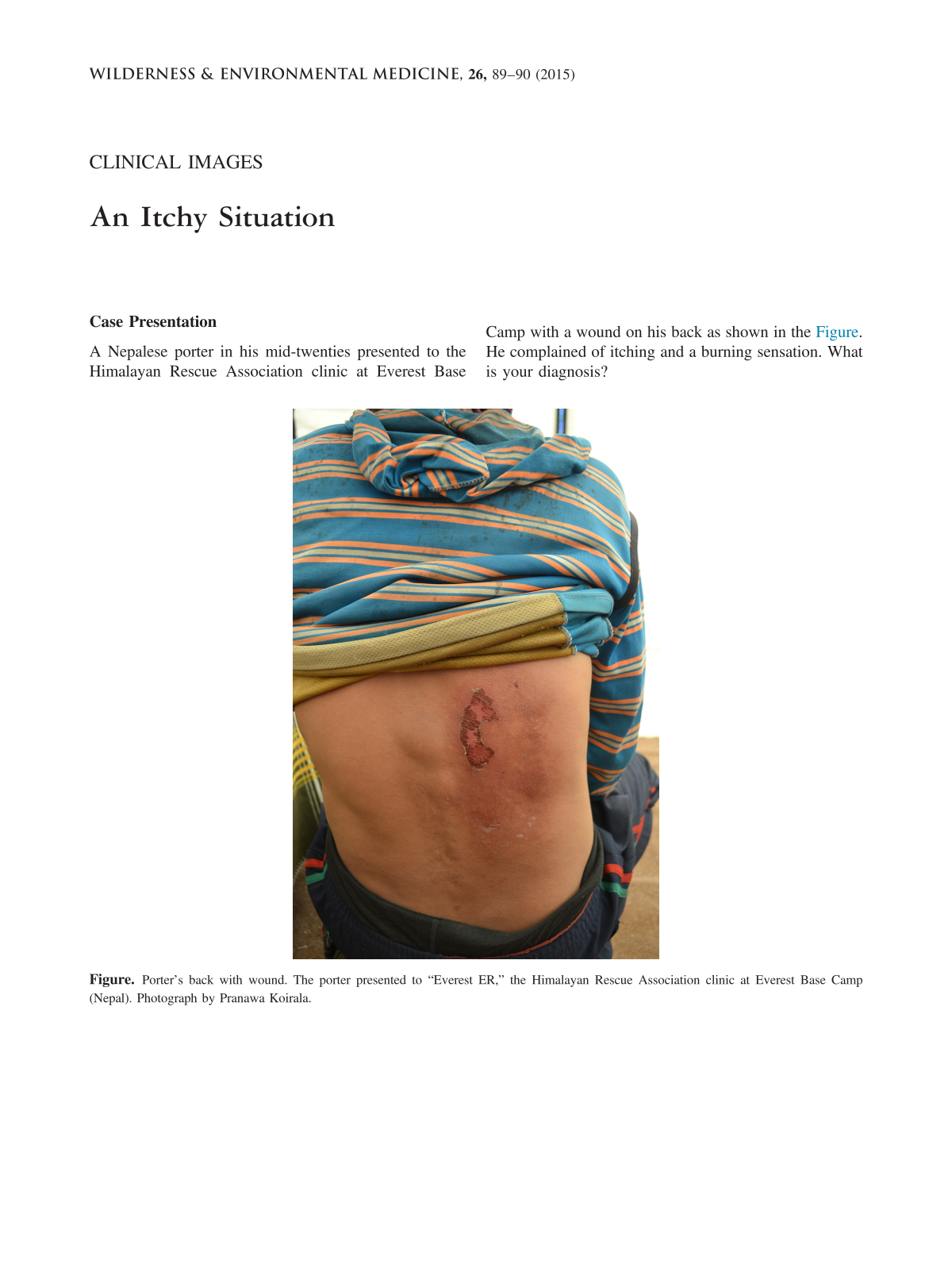
A Nepalese porter in his mid-twenties presented to the Himalayan Rescue Association clinic at Everest Base Camp with a wound on his back as shown in the Figure. He complained of itching and a burning sensation. What is your diagnosis?

Porter’s back with wound. The porter presented to “Everest ER,” the Himalayan Rescue Association clinic at Everest Base Camp (Nepal). Photograph by Pranawa Koirala.
Answer: Kerosene Dermatitis
The porter was carrying kerosene in a 5-gallon (19-L) plastic container, on his back, on the way to Everest Base Camp. The porter noted a leak a day or two after starting the trek. Since the container was expensive and no replacement container was available, he continued carrying it, thinking that there was not much spillage. Kerosene soaked through his t-shirt. He developed itching and a burning sensation. About 2 days before reaching Everest Base Camp he had a friend apply vegetable oil to the wound. In Nepal, it is commonly believed that using vegetable oil can heal kerosene dermatitis. After 6 days, he presented to the “Everest ER.”
On examination, the porter had the wound shown in Figure. The clinic staff gently washed the wound with normal saline solution, then applied aloe vera cream and a dressing. They advised the porter not to carry weight on his back until the wound healed completely. During the next few days, clinic staff dressed the wound twice more. The porter was then lost to follow-up.
Kerosene is widely used as a fuel and as an industrial solvent. It can cause contact dermatitis with chronic exposure. Jee et al 1 described 2 groups of factory workers, one with kerosene exposure to the hands (n = 79) and the other without kerosene exposure (n = 269). Of the first group, 84% had dermatitis of the hands, whereas only 1% of the latter group had dermatitis. 1 Most reported cases of contact dermatitis from kerosene are from chronic occupational contact, but kerosene dermatitis can also occur with acute exposure.
Contact with kerosene does not cause immediate skin irritation, but prolonged contact causes inflammation. Lesions usually develop in areas covered by clothes, rather than in skin exposed to air. Chemical dermatitis resembles first- or second-degree burns and is classified as a chemical burn. 2 Itching, stinging, and burning sensation are common complaints. 3 Initial skin lesions consist of erythematous discoloration. Blistering, scaling, fissures, and cracks occur in more chronic cases. There may also be superimposed infection. The smell of kerosene on clothes or a history of contact with kerosene suggests the diagnosis of kerosene dermatitis. In one published case, a 73-year-old woman presented with erythema with bullae and pustules on her abdomen and anterior right thigh. The lesions looked like partial thickness burns and had a faint smell like that of an organic solvent. The patient was unaware of exposure to any substance. On analysis of detached epidermis using a gas chromatography–mass spectrometry method, kerosene was found to be the culprit. 2
Initial treatment consists of gently washing the area with normal saline solution or clean water to remove any remaining kerosene to prevent further damage. Topical corticosteroids and emollients are widely used to treat contact dermatitis. 4 Topical antibiotics can be used in combination with steroids in cases that appear to be infected. 4 Kerosene dermatitis resolves without sequelae within about 3 weeks once the skin is no longer exposed to kerosene. 5
Avoiding contact with kerosene is the best method to prevent kerosene dermatitis. In case of contact, the skin should be immediately and thoroughly cleaned to prevent dermatitis from developing.
Footnotes
☆
This work was not supported.
☆☆
None of the authors have any financial conflicts of interest to declare.