
Abstract
Objective
To describe the prehospital management and safety of search and rescue (SAR) teams involved in a large-scale rockfall disaster and monitor the acute and chronic health effects on personnel with severe dolomitic dust exposure.
Methods
SAR personnel underwent on-site medical screening and lung function testing 3 months and 3 years after the event.
Results
The emergency dispatch center was responsible for central coordination of resources. One hundred fifty SAR members from multidisciplinary air- and ground-based teams as well as geotechnical experts were dispatched to a provisionary operation center. Acute exposure to dolomite dust with detectable silicon and magnesium concentrations was not associated with (sub)acute or chronic sequelae or a clinically significant impairment in lung function in exposed personnel.
Conclusions
The risk for personnel involved in mountain SAR operations is rarely reported and not easily investigated or quantified. This case exemplifies the importance of a multiskilled team and additional considerations for prehospital management during natural hazard events. Safety plans should include compulsory protective measures and medical monitoring of personnel.
Introduction
Natural hazard disasters have been a part of the recorded history of the Alps for centuries. The destruction of the city of Plurs, Switzerland, in the 17th century, and the village of Arth-Goldau, Switzerland, and the death of 457 inhabitants in 1806 are well-documented examples of historic rockslides. 1 Major events of the past century include the devastating rockslide of Monte Toc into the Vajont reservoir, Italy (1963), which caused the largest landslide in recent European history with 1917 fatalities, as well as the rockslide of Valtellina, Val Pola, Italy (1987), and Randa, Switzerland (1991).
Whether a natural hazard or any other environmental disaster, emergency situations require the implementation of medical search and rescue (SAR) operations in highly adverse conditions. 2 The risk for responding personnel may be minimal or may pose potentially severe or fatal consequences. 3 When planning an intervention, the risks incurred by personnel must be weighed against the expected benefit for the victims. However, the inherent need for immediate response may override the feasibility of adequate assessment of the potentially adverse effects of exposure to the situation. 2 Interestingly, the prevalence of fatalities in SAR teams and the physical and psychological sequelae are often not reported, and literature on SAR operations in mountainous areas is lacking.
The largest rockfall disaster in recent European history occurred on October 12, 2007, in a highly popular tourist area of the Italian Dolomites. The resulting dust cloud spread rapidly throughout the area, severely limiting visibility. The aim of this report is to describe the prehospital management and safety of the SAR teams and to monitor the acute and chronic health effects on personnel with severe dolomitic dust exposure.
Methods
Information on the emergency response operation was collected from the emergency dispatch center, mountain rescue organizations, and firefighter divisions. Medical screening including patient history, clinical examination, and pulmonary auscultation was performed on site in exposed personnel immediately after SAR duties, and medical and lung function data were collected 3 months (December 2007, n = 21) and 3 years (December 2010, n = 14) after the event. Participants were informed that they would be part of a follow-up study, and written informed consent was obtained. A reference sample of spirometry data was obtained from firefighters not involved in this event but who had had a routine spirometry test in 2007 (n = 20). The study was reviewed by the local ethics board.
Lung function was investigated in accordance with the standardized procedures of the American Thoracic Society 4 using a Pony Spirometer 3.9 (COSMED, Rome, Italy) and Minispir S/N 001771 (MIR Medical International Research, Rome, Italy). Measured parameters included forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and forced expiratory flow at 75% of FVC (FEF75). Reference values were calculated from the predictive equations of the European Resuscitation Society Statement. 5 All results are reported in percentage of reference value (mean ± SD) unless indicated otherwise.
Student’s
Results
Emergency Medical Service Response
On October 12, 2007, approximately 60,000 m3 of rock released from the northwestern slope of Mt Einser (2698 m), Italy, resulting in a dust cloud that spread rapidly throughout the region (Figure 1). The provincial emergency dispatch center was alerted at 9:41

Initial release of material from Mt Einser on October 12, 2007 (A), and dispersion of the dust cloud 5 (B), 10 (C), and 60 (D) minutes after release. Photo credit: P. Tschurtschenthaler, firefighter division Sexten.
Medical Screening
The mean age of participants at the 3-month screening was 36.3 ± 13.9 years (n = 21), and all participants were male. There were 12 nonsmokers, 6 ex-smokers, and 3 smokers. Smoking status remained constant during the period of investigation. Occupational dust exposure (metal, wood, and flour dust) was reported in 8 participants.
At the on-site medical screening there were no life-threatening events in any of the exposed personnel. Self-reported complaints included feelings of pressure in the chest (n = 1), nausea (n = 1), and upper airway viral disease (n = 1). The maximal reported duration of dust exposure was less than 6 hours (<2 hours, n = 1; 2–4 hours, n = 10; 4–6 hours, n = 4; unknown but <6 hours, n = 6), and 20 of 21 rescuers wore a European standard FFP1 respiratory face mask during SAR activities in the area (duration with mask <2 hours, n = 9; 2–4 hours, n = 5; unknown but <6 hours, n = 6). Between the 3-month and 3-year screening there were no reports of onset of a disease and no aggravation of previously existing diseases.
Spirometry Screening
In total 14 participants (67%) completed both the 3-month and 3-year spirometry screenings. Two individuals with pathological spirometry results attributable to preexisting conditions (1 ex-smoker with occupational dust exposure; 1 with chronic asthma) were removed from the analysis. Comparison of the 3-month and 3-year spirometry data showed a reduction in mean FVC (3-month, 110.5% ± 13.1% of predicted reference value; 3-year, 104.6% ± 11.6%; n = 12;
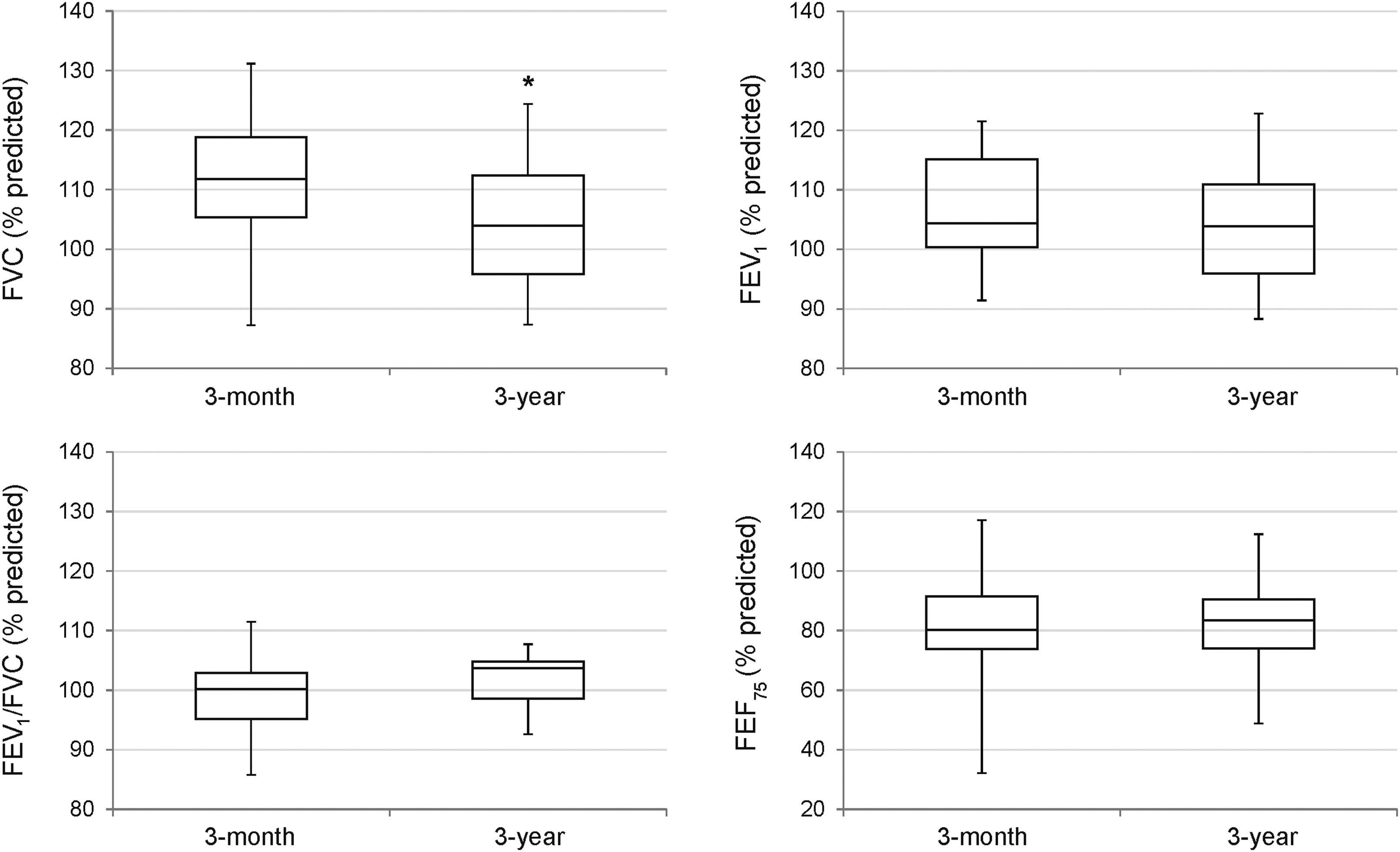
Box and whisker plot of lung function parameters at 3-month and 3-year postevent screening. * indicates significant difference from 3-month value (
There was no difference in lung function parameters between the test sample at the 3-month screening (values given above) and the reference sample of nonexposed firefighters in the same period (FVC, 112.3% ± 12.8% of predicted reference value,
Discussion
This is the first report of a SAR response and medical screening after a large-scale rockfall disaster. This study exemplifies a rapid and organized response of a multiskilled team and highlights the importance of monitoring and reporting health risks of emergency response operations in mountainous areas.
Medical screening after rockfall-induced dust exposure has never been reported despite exposure of rescuers and local residents in previous large-scale events. A rockfall event (approximately 30 million m3 of material) in 1991 in Randa, Switzerland, produced a dust cloud that severely limited visibility and resulted in depositions of up to 50 cm of fine material (containing silica and silicates) in surrounding villages. 6 Crystalline silica in the form of quartz or cristobalite has been classified as a human (group 1) carcinogen, 7 and chronic occupational exposure has been implicated in the development of silicosis and many other disorders. 8 A review of chronic occupational exposure (mean, 7 to 25 years) to low silica concentrations (8% to 30% of respirable dust) concluded that there is evidence of chronic bronchitis, emphysema, and small airway diseases also in the absence of radiological signs of silicosis. 9 Energy-dispersive x-ray spectroscopy of the dust material from the Mt Einser event showed a silicon content of less than 2% and a substantial content of magnesium (11.15%). The effects of acute exposure to these concentrations are unknown, and reports in the literature are lacking. There were no instances of severe acute or subacute respiratory diseases after this event, and spirometry testing of rescuers did not indicate a clinically significant impairment 10 or reduction in lung function based on 6 hours or less of acute exposure using an FFP1 face mask. It should be noted that comparative preevent spirometry data were not available because volunteer rescuers in these organizations do not undergo regular medical screening, but comparison with a similarly aged reference sample did not reveal any differences.
Rockfall events have occurred repeatedly in the Dolomites and can be expected in the future in regions where thawing permafrost has increased slope destabilization. 11 SAR personnel should be equipped with protective measures to minimize dust exposure during rockfall events. Safety plans for response operations during natural hazards are a pertinent issue to prehospital emergency services operating in mountainous areas and should be defined well in advance and include on-site medical monitoring and follow-up of exposed personnel. Additional considerations are important, especially coordination with geotechnical experts for monitoring acute hazards in the area. Central coordination through an emergency dispatch center may assist in allocation of resources and dispatching of adequately trained and equipped teams.
Limitations
Because of the nature of the event, the study design has inherent limitations. First, the sample size is small and the exposure time and severity was variable among SAR personnel. Additionally, the control group participants may have had previous occupational exposures that potentially affect spirometry results, although the clinical findings suggest normal lung function in these participants.
Conclusions
The risk for personnel involved in mountain SAR operations is rarely reported and not easily investigated or quantified. This is the first report of a SAR response and medical screening after a large-scale rockfall disaster. Further longitudinal investigations should be encouraged to increase our understanding of health and safety risks involved in response to natural hazards in mountainous areas and the impact of medical monitoring.