
Abstract
Objective
To describe search and rescue activity performed by the National Park Service (NPS) on Denali, the highest point in North America.
Methods
A retrospective review was performed of all search and rescue (SAR) operations by the NPS from 1990 to 2008. Descriptive analysis was used to describe these cases as well as chi-square and logistic regression analysis to determine which mountaineers were more likely to require a rescue.
Results
During the study period, 1.16% of all Denali climbers required NPS SAR response. The majority of medical cases (68.9%) were due to high altitude and cold injuries, and the majority of traumatic cases (76.2%) resulted from a fall. Mountaineers that attempt routes other than the standard West Buttress route are more likely to require rescue. Climbers are 3% more likely to require a rescue with each year of advancing age. Similarly, mountaineers from Asia are more likely to require a rescue (odds ratio = 4.1), although this trend has diminished in the past decade.
Conclusions
Mountaineers and rescuers should educate themselves on the environmental, logistical, and medical origins of Denali rescues. Certain demographic groups on certain routes are more likely to require a rescue on Denali. Rescuers should be aware of these groups and have the knowledge and capabilities to care for the medical issues that are common on SAR responses.
Introduction
Mount McKinley, commonly referred to by its native name of Denali, is a popular destination for mountaineers worldwide. As the highest point in North America at 6194 m (20 320 ft), more than 1000 climbers attempt to reach the summit annually. 1 The mountain is located within Denali National Park and Preserve and is managed by the National Park Service (NPS). The remoteness, northerly latitude, degree of glaciation, and high elevation of Denali provide extreme challenges for climbers. Because of the popularity and extended ascent time required for acclimatization, large numbers of climbers are present on Denali during peak season, in particular on the commonly climbed West Buttress route.
Mountaineers on Denali periodically require medical assistance or rescue. The NPS maintains an active mountaineering ranger patrol presence on Denali throughout the peak season. On the West Buttress route, ranger camps are established from May to late June at 2190 m (7200 ft) on the Kahiltna Glacier, in a basin at 4330 m (14 200 ft), and at a high camp at 5227 m (17 150 ft). While also serving as bases for environmental oversight, these camps function as a medical resource for climbers and allow advanced staging for search and rescue (SAR) activities. Trained personnel with a complete cache of rescue equipment are on-call 24 hours a day. Advanced medical supplies are available including oxygen, intubation equipment, a portable hyperbaric chamber, high altitude medications, and gear to care for common medical emergencies. Although the camps do not currently store or use advanced cardiac life support medications, they have the capability of supporting a sick or injured climber for several days if weather prevents a helicopter rescue. Because rescue personnel are stationed at the high altitude camps, they are acclimatized for high elevation. The NPS patrols on Denali are composed of a paid mountaineering ranger staff as well as rescue and/or medical volunteers.
The most recent multiyear review in the medical literature regarding Denali rescues was published in 1993 and includes data preceding 1988. 2 Since this time there has been significant evolution in the Denali National Park (DNP) mountaineering safety program including aggressive educational outreach, mandatory Denali registration with a user fee to support this program, a contracted high altitude Lama helicopter for SAR assistance, and the establishment of a regular peak-season ranger camp at 4330 m (14 200 ft). Another recent Denali study examined fatalities on the mountain. 3 A study published in 2008 reviewed rescue data for all Alaska national parks for 2002 only. 4 With increased climber presence on Denali, the demographic and medical factors of rescues need to be better characterized to ensure continued medical and rescue preparedness and to direct preventative intervention. The purpose of this study was to review the incidences and circumstances associated with mountaineering SAR activity on Denali.
Materials and methods
We performed a retrospective descriptive analysis of Denali NPS mountaineering SAR records from January 1990 through December 2008. The following criteria were used to define SAR for the purposes of this study: mountaineering-related, reported by a Case Incident Report (CIR), and action taken on the part of NPS to rescue or search for a climber thought to be in distress and thought to be alive at the start of the SAR mission. Case Incident Reports are documents generated by the NPS for any major occurrence within a national park and include descriptions of all SAR activity. This SAR definition excludes cases of climbing teams who performed unassisted self-rescue but who may have presented to NPS patrols strictly for medical assistance, for example at the 4330 m (14 200 ft) ranger camp. This definition also excludes aircraft crash incidents, air drops of supplies, and known body recoveries. The term
Records of climbers intending to ascend Denali were obtained with the assistance of DNP South District mountaineering ranger staff based in Talkeetna, Alaska, and the DNP medical director. Demographic data, details of the incident, and medical information (when available) were extracted from these records. One co-author (A.B.) extracted all data from CIRs. South District CIRs and medical run sheets were reviewed for the dates noted above. Though every SAR was recorded by CIR, not all SARs had an associated medical run sheet, in which case relevant medical information was derived solely from the CIR. Demographic information was obtained from the CIR and the climber registration database maintained by DNP South District staff for all Denali climbers. In the case of a discrepancy between the CIR and the registration database, information from the registration database was used.
Both guides and clients were grouped into the category of “guided group” for this analysis. Prior to 1994, the NPS database did not distinguish between guide and client status and it was therefore not possible to separate these populations. National Park Service personnel, which include both NPS rangers and rescue/medical volunteers, were likewise categorized as “guided” because at least one member (eg, the NPS mountaineering ranger) was very familiar with the geography of Denali, its weather patterns, risks, and potential climbing pitfalls.
Statistical Analysis
Categorical variables are presented as percentages and numbers. Continuous variables are presented as medians. Pearson's chi-square test and logistic regression analysis were used to calculate odds ratios and statistical significance. Univariate and multivariate analysis was performed, and a logistic regression model was developed to explain the likelihood of a rescue. Statistical significance was set at .05. All statistical analyses were carried out using SAS version 9.1.3 (SAS Institute Inc., Cary, NC). The University of Utah Institutional Review Board reviewed and approved the study.
Results
During the study period, 261 of 22 385 registered Denali climbers (1.16%) required NPS SAR response. The mean age of SAR subjects was 37.2 years (median 35, SD ±10.4, range 18–65, interquartile range 16). Thirty-one (11.9%) fatalities were captured in our SAR definition and included in the analyses presented below. Table 1 displays descriptive information of these SAR subjects, and Table 2 describes country of origin.
Descriptive data of registered Denali climbers requiring National Park Service (NPS) search and rescue (SAR) response, 1990 to 2008
VIP, volunteer in the park (NPS volunteer ranger).
Country of origin of SAR subjects
Countries contributing less than 5% of total cases.
Search and rescue took place on the West Buttress route in 184 (70.5%) cases and on another Denali route in the remaining 77 cases. The mean elevation of SAR cases was 4844 m (15 892 ft) with a range of 2073 to 6187 m (6801–20 299 ft). Of the 261 subjects, a helicopter operation was involved in 212 (81.2%) cases, a ground team was deployed in 138 (52.9%), and 99 (37.9%) cases involved both helicopter and ground teams. One hundred seventeen (44.8%) SARs occurred while the subject was descending. Of the 77 total falls recorded as the primary reason for SAR, 59 (77%) occurred on descent.
The inciting cause for each SAR response is described in Table 3. Denali is known for high altitude and extreme cold, and the majority of causes of medical cases reflected these features. The chief complaint of medical SAR cases is noted in Table 4, and the incidence of altitude and cold injuries among SAR cases is described in Table 5. Of the 101 cases involving a traumatic mechanism, anatomic body location was noted in the medical record of 76 (75.2%). When examining these 76 cases, 24 (31.6%) involved head trauma, 31 (40.8%) torso trauma, and 44 (57.9%) extremity trauma.
Reason/cause for SAR
Chief complaint of general medical SAR cases (excludes altitude and cold-related injury)
Includes one known case of appendicitis.
Gastrointestinal bleed, hematemesis, nausea, vomiting, diarrhea.
Diagnosed as ultraviolet keratitis.
Diagnosed as deep venous thrombosis.
Suspected transient ischemic attack by evaluating physician.
Incidences of cold and high altitude afflictions as primary reason for SAR
HAPE, high altitude pulmonary edema; HACE, high altitude cerebral edema; AMS, acute mountain sickness.
Many cases had multiple reasons for SAR.
One of the SAR cases was unable to be matched to the NPS database because of insufficient information; this single case was excluded from epidemiologic analyses. In the univariate analysis, men and women showed a similar rate of rescue (odds ratio [OR] = 0.91; 95% confidence interval [CI] 0.61–1.37,
Factors that predicted National Park Service SAR assistance on Denali: final multivariate logistic regression model
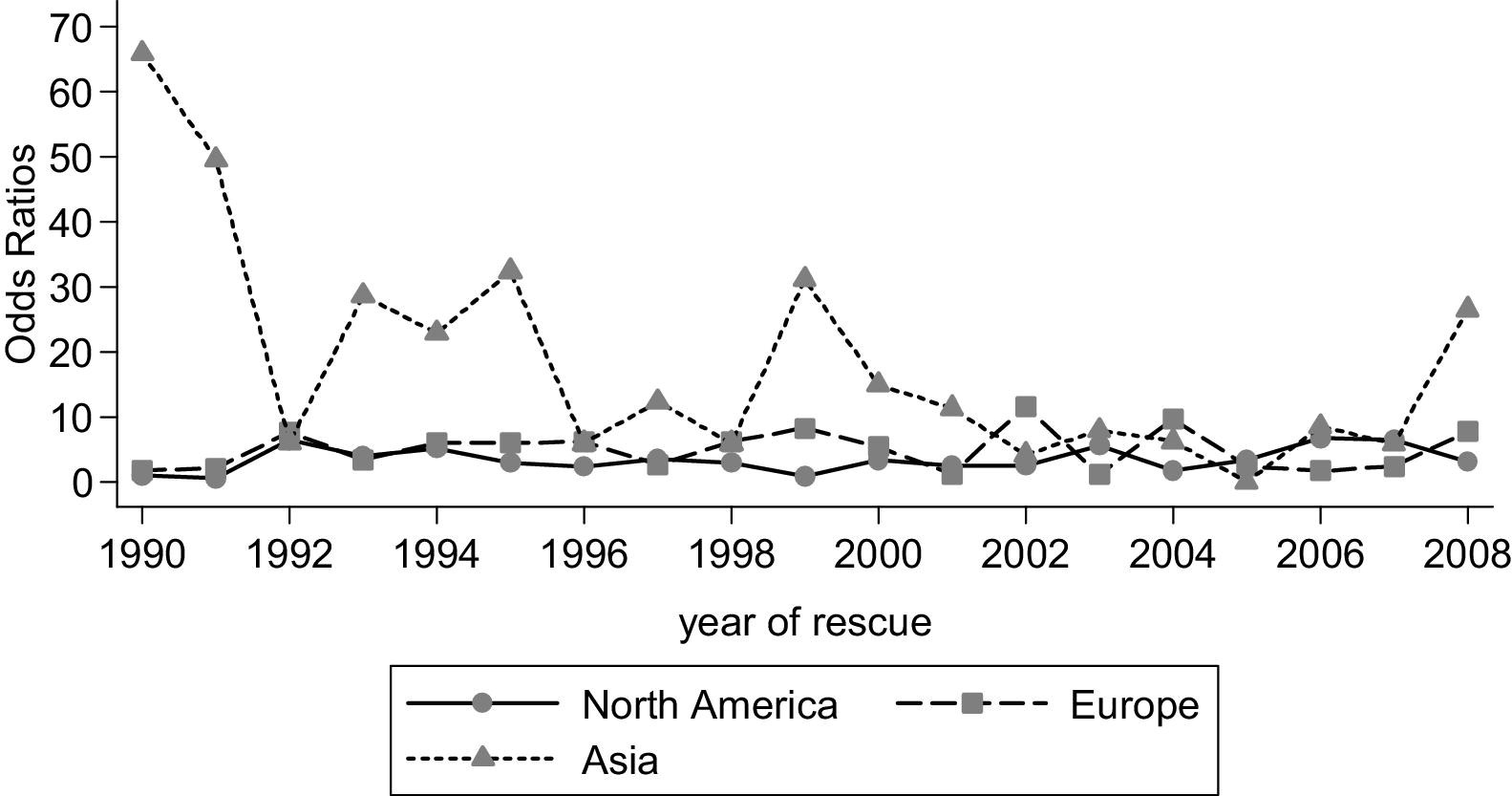
Adjusted estimate of a rescue for climbers from North America, Europe, and Asia, 1990 to 2008. The estimate was adjusted for year of rescue, age, route name, summit, continent, as well as interaction between year of rescue and continent.
Those climbing the West Buttress route were less likely to be the subject of SAR activity (OR = 0.32, 95% CI 0.25–0.43,
Discussion
Search and rescue circumstances and medical complaints varied widely in our study. As expected, subjects with high altitude-related disorders accounted for a large percentage of those rescued on Denali. The actual number may even be higher because of the vague signs and symptoms of altitude disorders and overlap with other medical disorders. In addition to high altitude disorders, rescuers should prepare for general emergency complaints including cardiac, respiratory, and abdominal/gastrointestinal disorders. Other studies examining medical cases on wilderness expeditions 5 –9 confirm that a wide spectrum of emergencies must be expected. Trauma overall was slightly less common than medical complaints, but falls were the single most common reason for activating SAR.
Independent climbers, clients, guides, and NPS personnel alike required rescues during the study period. This reinforces the reality that no one demographic or age group is immune to challenges in high altitude mountaineering. Individuals in a guided party were, however, less likely to need a SAR overall. Climbers may be safer overall as a member of a guided group. However, it should be noted that guides likely performed many rescues independently of the NPS and these incidents were not captured in this study. Three SAR events were initiated for members of NPS patrols. Members of SAR teams are experienced climbers but not protected from the hazards of climbing. Although rescues typically involve careful planning and coordination, the rescuer may become the victim, as a result of poor decisions regarding the environment of the rescue (eg, weather, terrain) or the willingness of rescuers to assume additional risk to aid a fellow climber.
Our data also show that climbers from certain continents, for example Asia, are rescued at significantly higher rates than those from other continents. Data are similar to fatalities on Denali, in which climbers from Asia were more than 3 times more likely to die than North American counterparts. 3 However, odds ratios for Asian climbers requiring rescue appeared to be reduced in the 2000s compared with the 1990s, suggesting safer climbing practices by this population.
Comparing our data with Denali rescue data from the period 1978–1987, 2 the rate of SAR has been steady or declined slightly from 1.9% to 1.2%. Search and rescue from altitude illness has declined slightly (26% in Lattimore 2 vs 20% in the current study). These shifts may be a result of the NPS efforts to educate climbers on preventable medical conditions, however many other factors may be involved as well. National Park Service education is accomplished by mailing education materials to all registered climbers as well as conducting a safety briefing in Talkeetna immediately prior to the climb. The Denali climber education program was established as a directed effort to improve the safety of climbers and may mitigate the objective hazards of mountaineering. Although climbers may now be more educated on preventable medical issues, falls and weather continue to be constant risk factors in mountaineering. Also, the mean age of climbers rescued from 1978 to 1987 was 32 years, compared with 37 years in this study from 1990 to 2008. This shift of rescues parallels the increasing age of mountaineers on Denali.
Schussman et al 10 published an incident rate of 2.5% among mountaineers in Grand Teton National Park (GTNP), which is higher than the rate of SAR on Denali. Notably, the GTNP study, similar to Denali, found that falls on snow or ice were the most common incidents. National parks in the United States typically employ SAR teams that are on-call to respond to emergencies. These teams may be paid or volunteer.
Our data on the medical problems prompting SAR on Denali in many ways mirror the spectrum of wilderness medical emergencies. Abdominal pain, gastrointestinal and respiratory issues, and chest pain are frequent general expedition complaints and were high in frequency in Denali SARs as well as in other studies. Fatigue was the top medical cause for SAR in our study and frequently accompanies the vigor required to climb high altitude mountains. This complaint is not usually ascribed as a top medical problem in the wilderness; however, our results show that the complaint must be considered seriously as it commonly prompts SAR.
The majority of wilderness rescuers have a basic level of medical training, and it may be challenging for a responder of this type to diagnose complex abdominal, cardiac, or respiratory complaints. Furthermore, certain medical problems, for example pneumonia and high altitude pulmonary edema, may present similarly, but treatment strategies differ significantly. Sufficient medical direction should be present for medical personnel operating in remote locations where extended treatment may be required. This can be provided via prewritten protocols or by online telephone or radio medical direction. Rescue and medical personnel must possess a wide variety of knowledge and skills to manage challenging incidents and treat those in need.
The NPS Denali medical and rescue program maintains a presence observed at very few high altitude mountaineering locations. In 1991, the NPS began to use a high altitude Lama helicopter for Denali rescues. Positioned in the town of Talkeetna adjacent to Denali, this helicopter is available during the climbing season to assist mountaineers in life-threatening situations or medical need. Flying time from Talkeetna for the helicopter to reach the camp at 14 200 feet is approximately 45 minutes. The helicopter has allowed the NPS to evacuate many climbers who may have otherwise perished. The use of rescue helicopters must always be balanced with the potential hazard and cost incurred in their operation.
Some critics have maintained that a rescue camp such as the one on Denali diminishes the essential self-reliance that mountaineering groups should possess during high altitude expeditions. However, the Denali rescue and medical camp has likely prevented many SAR events by providing medical assistance and education at a central location on Denali. The cost savings and ethical impact of preventing these larger-scale and perhaps riskier rescues is difficult to estimate.
Our study shows that rescue personnel on Denali are requested to assist and care for a significant number of sick or injured climbers. High altitude mountaineering involves a degree of risk that is not typically observed in other environments.3,11 Altitude, severe weather, and other unpredictable variables make climbing Denali a serious endeavor. Its ascent demands skill and experience for a mountaineering party to be safe and self-sufficient. Rescue personnel must receive adequate medical training and maintain a high medical and technical skill level when working in a high altitude mountain environment. It is also advantageous to maintain providers on the mountain who are acclimatized to high altitude to adequately function in these rescue scenarios. Rescue personnel must educate climbers on the potential pitfalls of high altitude mountaineering. They must be vigilant in observing and identifying certain populations that may be at risk for requiring a rescue and be prepared to halt an unprepared or potentially hazardous climbing team. This study provides both specific and epidemiologic data that can be used by rescue personnel for strategic planning, education, and resource allocation on Denali as well as other high altitude mountains.
Limitations
The primary limitation of this study was its retrospective nature. Although the NPS maintains detailed records, it is possible that not all rescues were captured with the CIR system. Additionally, this study did not intend to characterize cases that presented to the ranger camp. This is especially true for cases of high altitude illness and frostbite that presented to the ranger camp but did not require a formal SAR operation. Complete information was not always present in the CIRs, and as a result one case was not able to be matched to the NPS database. Anatomic location and specific injuries from traumatic mechanisms were not always complete, and therefore these results should be interpreted cautiously. Rescues performed by private parties were not described in this study. Rescue rates for various complaints may therefore not indicate the actual incidence of these complaints, only those requiring NPS participation in a rescue. Experience level of climbers was not able to be measured by these methods and may be an important factor in avoiding a rescue. Confounders invariably exist when comparing SAR rates over time. Weather, route conditions, and climber populations are not consistent from year to year. Indeed, these factors compose much of the risk of mountaineering.
Conclusion
Medical providers and rescuers on Denali and other high altitude mountains must have knowledge of a wide array of traumatic, general medical, and high altitude disorders. Rescue groups should educate mountaineers on the measures that can be taken to prevent and limit the number of rescues. Certain mountaineering groups have a higher likelihood of requiring SAR. The NPS mountaineering ranger program was called upon each year of this study for critical search and rescue activities.
Footnotes
Acknowledgments
The authors thank the staff of the Talkeetna Ranger Station for their assistance: Daryl Miller, Missy Smothers, Roger Robinson, Joe Reichert, Gordy Kito, Mik Shain, John Leonard, Dave Kreutzer, Meg Perdue, and Maureen McLaughlin.