
Abstract
Objective
To examine the medical care at a highly competitive 161-km mountain ultramarathon.
Methods
Encounter forms from the 2010 through 2013 Western States Endurance Run were analyzed for trends in consultation and use of intravenous fluids.
Results
A total of 63 consultations (8.2% of starters) were documented in 2012 and 2013, of which 10% involved noncompetitors. Most (77%) of the consultations with competitors occurred on the course rather than at the finish line, and were generally during the middle third of the race. Of the on-course consultations, the runner was able to continue the race 55% of the time, and 75% of those who continued after consultation ultimately finished the race. Relative number of consultations did not differ among competitors within 10-year age groups (
Conclusions
This work demonstrates that the medical needs in a 161-km ultramarathon are mostly for minor issues. However, occasional serious issues arise that warrant a well-organized medical system.
Introduction
Marathon participation has shown continued steady growth for the last 3 decades, 1 while participation in ultramarathons has grown exponentially in recent years.2,3 Ultramarathons, defined as running races longer than the 42.195-km marathon distance, may take place in a single day, be continuous, or be staged (noncontinuous) over several days, and often occur in wilderness environments. In addition to the inherent physiological stress of running long distances, these events may carry additional risks attributable to environmental factors such as challenging terrain and adverse weather conditions. Furthermore, ultramarathons often present geographical barriers to the provision of medical care unlike the typical marathon that takes place in an urban setting. Ultramarathons also differ from marathons in terms of participant characteristics. For example, the participants in ultramarathons tend to have a higher median age than those running marathons.1,2 Because of distinctions such as this, the large volume of research on marathons is not necessarily suitable for clarifying medical needs at ultramarathons.
Two prior studies systematically examined the medical needs during staged, multiple-day ultramarathons,4,5 but as far as we are aware, there is only one report on medical issues during a continuous ultramarathon, and that was from a relatively short (45-km) event. 6 Thus, the main purpose of the present work was to examine the medical care that has been provided in recent years at the Western States Endurance Run (WSER), the first mountain 161-km ultramarathon, and one of the most physically challenging running events in the world. A secondary aim was to examine the trend in use of intravenous (IV) fluids at the event. This is particularly important given that it has recently been recognized that ultramarathons can have a high incidence of exercise-associated hyponatremia,7,8 that provision of IV isotonic or hypotonic fluids can exacerbate the condition resulting in serious consequences,9,10 and that IV fluids are often overutilized at endurance events. 7 ,9,11–14
Methods
The study was approved by our institutional review board, with the requirement for informed consent waived.
The WSER is a 161-km ultramarathon that travels mostly on single-track trail through the Sierra Nevada Mountains of Northern California from Squaw Valley to Auburn, California. The course has a total ascent of 5500 m, a total descent of 7000 m, and reaches a maximum altitude of 2667 m. Ambient temperatures can fluctuate widely from year to year and during each event. All participants are experienced ultramarathon runners who are either awarded an entry based on a recent high-level performance or drawn by lottery from applicants who have met specific qualifying standards. Runners have a 30-hour time limit to complete the distance. The race provides 24 aid stations, with the longest distance between these stations being 12.5 km. Medical support is available at 8 of the aid stations and at the finish line. Each medical station has a medical captain who is either a physician, nurse, physician assistant, or emergency medical technician, and is typically staffed by 1 to 10 additional individuals with a variety of medical credentials. A standardized encounter form is to be completed by race medical staff for each consultation. Competitors are not penalized for seeking medical attention, with the exception that IV hydration on the course results in disqualification.
Completed encounter forms were collected from all medical stations of the 2012 and 2013 events and only from the finish line of the 2010 and 2011 events. Encounter forms documented course location, subject identifying information, symptoms, presumed diagnoses, and treatment provided. Encounter forms and race split data were used to determine whether a runner continued and finished the race or not. Consultations related to pace runners and race volunteers were included in the analysis because these individuals contribute to the medical needs at the event. Minimum and maximum ambient temperatures during each race were obtained from the weather stations nearest to the race start and finish as done previously, and noted to likely overestimate the early morning temperatures at the higher altitudes and underestimate the afternoon temperatures in the canyons.7,15
The main reasons for each consultation, including the symptoms and presumed diagnoses that were recorded on the encounter forms, were initially listed collaboratively by the authors. Examination of this list revealed distinct categories within broad diagnostic groups of medical, musculoskeletal, and other conditions. For encounters listing symptoms and presumed diagnoses of nausea/vomiting and dehydration, the former was chosen as the main reason for the consultation under the presumption that the nausea and vomiting was the underlying cause of the dehydration. Because minor blister care was not uniformly documented and there were no known cases in which a runner dropped out at a medical station where they received blister care, blisters were not included in the analysis. For each encounter, we recorded the primary reason for consultation based on the defined categories, the course location of the encounter, the type of subject (competitor, pacer, or race volunteer), and the subject’s sex and age, as well as whether or not they continued in the race and finished if they were a competitor. In addition to these data from the 2012 and 2013 events, finish line encounters for years 2010 through 2013 were examined for whether treatment included IV fluids.
Group comparisons were made with χ2 and Fisher exact tests. Relationships for frequency of consultation and IV fluid treatment with maximum ambient temperature during the race were examined with Pearson correlation analyses. Statistical significance was set at a probability value of less than .05.
Results
Pertinent information about the 4 events considered in this analysis is shown in Table 1. Ambient temperature conditions were particularly cool in 2012 and hot in 2013. Competitors encountered rain and sleet in the early portion of the 2012 event.
Pertinent information about race competitors and ambient temperatures for the 2010 through 2013 events
A total of 63 consultations (8.2% of starters), each for a unique individual, were documented in 2012 and 2013 (Table 2). No runner repeatedly sought care. Six consultations involved noncompetitors: 1 safety runner, 1 aid station volunteer, and 4 pacers. Most (77%) of the consultations with competitors occurred on the course rather than at the finish line. Of those consultations on the course, the runner was able to continue 55% of the time after consultation, and 75% of those who continued after consultation ultimately finished the race. Overall, nausea and vomiting accounted for the largest number (24%) of consultations, and when a runner was seen for this reason on the course, they were able to continue 62% of the time without provision of prescription medication; 60% of those ultimately finished. In contrast, no runner seen for hypothermia or concussion continued. The relative number of consultations did not differ among competitors within 10-year age groups (8.6%, 8.8%, 7.0%, 5.1%, and 5.7% for age groups ≤29, 30–39, 40–49, 50–59, and ≥60 years, respectively,
Number (% of race starters) of consultations by reason/symptoms, location, and disposition for 2012 and 2013 events
Noncompetitors included 1 safety runner, 1 aid station volunteer, and 4 pacers.
The distribution of consultations by year, broad diagnostic group, and course location for 2012 and 2013 is shown in Table 3. Considering the 2 years together, the largest number of consultations (43%) occurred during the middle third of the race. But the distribution of consultations differed (
Number (% of race starters) of consultations by broad diagnostic group and course location for 2012 and 2013 a
Data are inclusive of 6 noncompetitors.
The number of individuals receiving IV fluids at the finish line was 33 in 2010, 15 in 2011, 1 in 2012, and 7 in 2013. No IV fluids were provided on course in 2012, and 2 individuals (1 competitor and 1 pacer) received IV fluids on course in 2013. The proportion of finishers consulting and being treated with IV fluids at the finish line decreased (
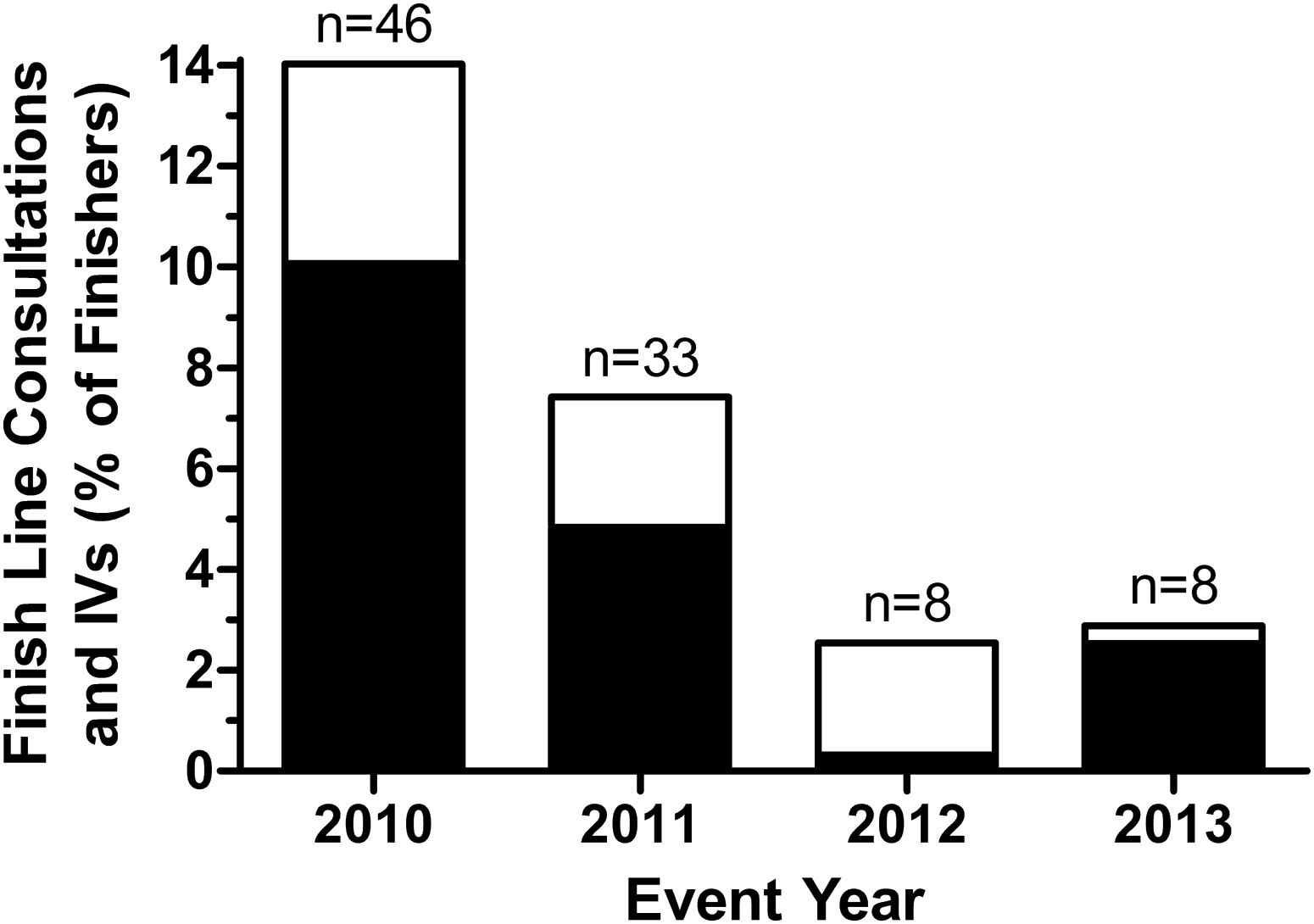
Use of intravenous (IV) fluids (black bars) and consultations (summation of black and white bars) at the finish line expressed as percentages of finishers. The number of finish line consultations each year is also provided.
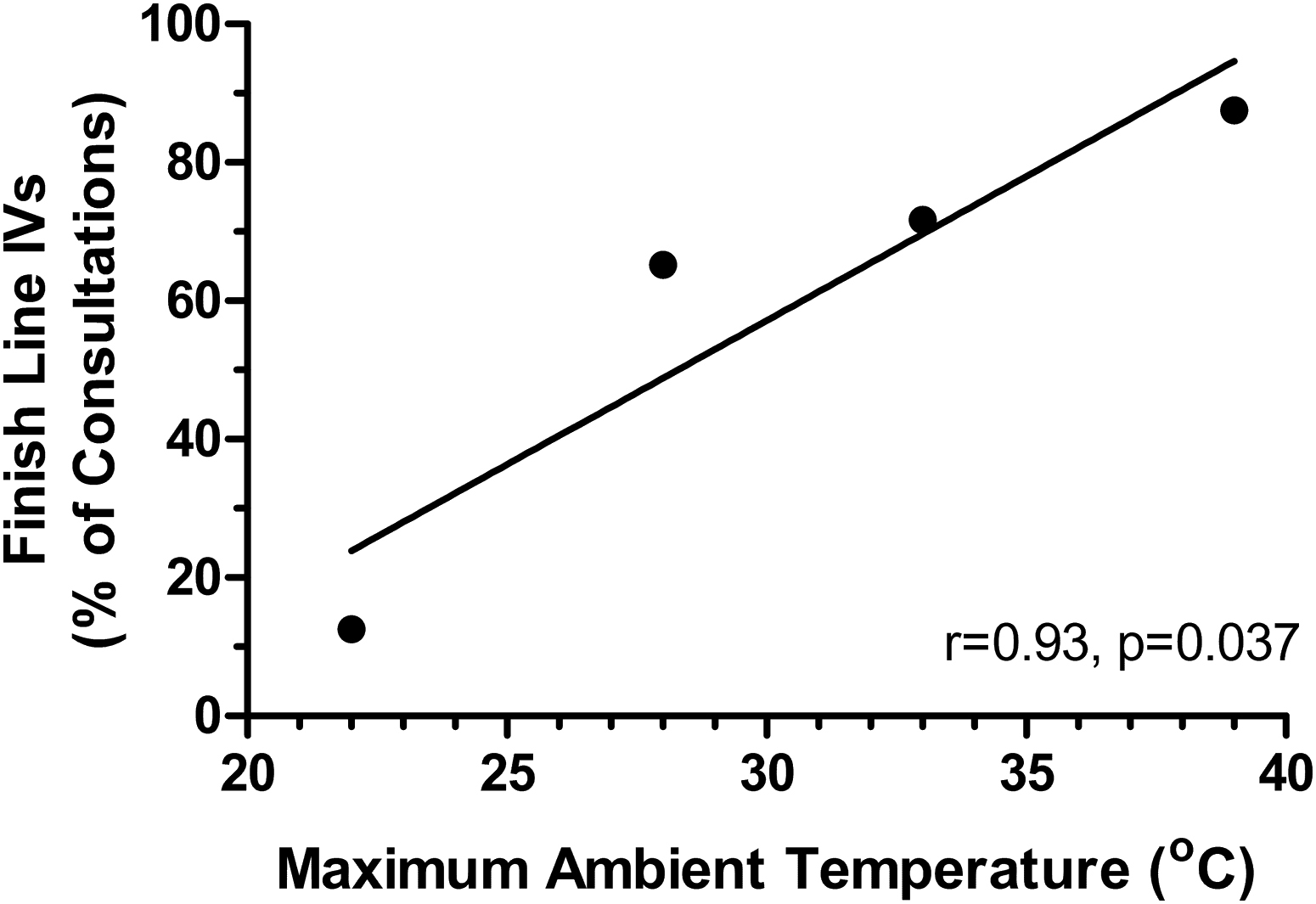
Relationship of runners receiving intravenous (IV) fluids at the finish line expressed as a percentage of consultations at the finish line with race-day maximum ambient temperature.
Discussion
A key finding of this study is that only a small proportion (8.2%) of starters sought medical care, and some of those individuals who received care (10%) were not competing in the race. The latter finding may not be surprising given that the event reports involvement of more than 1500 volunteers and most of the competitors use at least 1 pacer. When considering those involved with the event as a competitor, pacer, or volunteer, the overall incidence of consultation was approximately 1%, and is substantially lower if one also considers the number of individuals present at the event as spectators and crew members for competitors. This would suggest that the medical needs at this event are probably of comparable magnitude to other mass gathering events. 17
Another key finding of this work is that more than 60% of consultations were for issues categorized as medical in nature, as opposed to being in the broad diagnostic groups of musculoskeletal or other. Overall, nausea and vomiting accounted for the largest number (24%) of consultations. Prior work has demonstrated that gastrointestinal issues are common in ultramarathons. 18 –22 In fact, among 161-km ultramarathon participants, nausea or vomiting was found to be the main explanation for dropping out, and to be a major factor adversely affecting performance among finishers. 21 The cause of these symptoms is thought to be multifactorial, related to nutritional and fluid consumption, gastrointestinal motility, visceral hemodynamics, endotoxins, and neuroendocrine effects that are altered during ultraendurance events. 23 Limited prior work suggested that the incidence of gastrointestinal complaints was not related to ambient temperature. 21 However, the present finding that there were fewer consultations for nausea/vomiting under the cooler ambient conditions calls this into question.
The present work also found that most (77%) of the consultations with competitors occurred on the course rather than at the finish line. Considering the 2 study years together, the largest number of consultations (43%) took place during the middle third of the race. However, the distribution of consultations over the course was altered by ambient temperature conditions in that the largest proportions of consultations occurred during the last third of the race when conditions were cool, whereas they were mostly during the middle third of the race when conditions were hot. This is likely related to the fact that runners generally experience the highest ambient temperatures during the middle third of the race. Recognizing such effects is important in planning for medical care during these events.
It is worth noting that of those consultations that took place on the course, the runner was able to continue 55% of the time after consultation, and 75% of those who continued after consultation ultimately finished the race. This suggests that most of the on-course consultations were not for serious issues. On the other hand, rare serious issues did occur, as evidenced by the fact that 1 runner required emergency evacuation in both 2012 and 2013.
The present work examined whether any runner characteristics could be identified that appeared to make them more susceptible to requesting consultation. In this regard, we were able to examine age and sex, and found that these variables did not affect the relative chance of a competitor seeking consultation. Other variables, such as years of running experience and number of prior 161-km ultramarathon finishes, might be variables worth exploring in the future.
To our knowledge there has been no prior systematic evaluation of IV use at an ultraendurance event, although the topic has generated considerable debate. 9 ,11–14 Through such discussion, it is evident that IV fluids have been overutilized in some environments. Besides not generally being required for postevent rehydration, there is concern that IV hydration with isotonic or hypotonic fluids could have disastrous consequences in an athlete with exercise-associated hyponatremia. 7 ,9,10,16 For this reason, there has been an effort at the WSER to educate our medical staff on this issue. The findings from the present work suggest that this effort has made a favorable impact as there has been a reduction in finish-line IV use (from 10% to less than 3% of finishers) during the past 4 years that was independent of variations in ambient temperature conditions. Besides education of medical staff, it is also possible that the reduction in IV use also relates to education of participants about proper during-event and postevent hydration, and the circumstances in which postevent IV rehydration may be appropriate. These educational efforts may also account for the reduction in consultations at the finish.
The findings from this study provide an opportunity to compare the medical needs at a 161-km mountain ultramarathon with what has previously been reported for marathons and staged multiple-day ultramarathons. The present consultation rate of 8.2% falls within the range of 2% to 12% that has been reported for marathons.17,24 However, it is substantially lower than what has been reported for a 5-day staged 209-km ultramarathon in which 56% of participants were seen with a medical problem 5 or for 7-day staged 250-km ultramarathons in which 85% of participants were indicated to have been evaluated for at least one illness or injury. 4 The most common issues for which medical care is sought in marathons and short ultramarathons relate to medical, as opposed to musculoskeletal or other, issues.6,25 This was consistent with the present findings. However, musculoskeletal issues and blisters predominate in multiple-day events. 4 ,5,26,27 Our prior work has shown that blisters and “hot spots” impact race performance among 40.1% of finishers in 161-km ultramarathons, but these issues are the main reason for failing to finish only 5.8% of the time. 21 In other words, blisters and hot spots are a common annoyance, but rarely the cause for failing to finish a 161-km ultramarathon. Although the present work did not include medical consultations for blister management, it is apparent that the need for such care is not of the same magnitude as for multiple-day events. Thus, it appears that both the incidence and general categorization of issues for which consultation is sought in a continuous 161-km ultramarathon may be more comparable to that of a marathon than a staged multiple-day ultramarathon.
The present work is an initial effort to characterize medical needs at a 161-km mountain ultramarathon and so some limitations to the work should be noted. Most importantly is the fact that most of the analysis herewith is based on only 2 years of data and that the study was focused on a rather unique event. Being one of the most desirable and competitive 161-km ultramarathons in the world, WSER competitors tend to have considerable running experience, and appear to be better trained than at other large 161-km ultramarathons. 21 These factors undoubtedly affect the medical needs at the event, so generalization of the present findings should be done with caution. Additionally, the present examination of 2 years that were quite different in ambient weather conditions indicates that medical needs are affected by ambient conditions, so this is another factor of importance when considering the present findings in planning the medical needs at other events. Finally, we acknowledge that the encounter forms were completed by volunteer medical staff of varying levels of expertise, which could have affected the recorded information. Formal prerace education for medical staff on diagnostic coding and use of standardized diagnostic categories, along with formal testing of consistency in documentation, would have been optimal for reducing errors in determination of the main diagnostic category for each consultation.
From this work, we draw several conclusions about the medical needs at a highly competitive 161-km mountain ultramarathon. First, the overall incidence of consultation is not high, and is comparable to what has been reported for some marathons. Second, most consultations take place in the middle portion of the race and the type of issues vary with ambient conditions, so these factors should be considered in the determination of how best to distribute medical resources during these events. Finally, although most consultations in this event were for nausea and vomiting, or other issues that were not serious, occasional serious issues do present, making it essential for a well-organized medical system to be in place for these types of events.
Footnotes
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the VA Northern California Health Care System.
☆
Presented in part at the American College of Sports Medicine annual meeting, May 29, 2013, Indianapolis, IN.
☆☆
Disclaimer: The contents reported here do not represent the views of the Department of Veterans Affairs or the United States Government.