
Abstract
Objective
Physical activity is a cornerstone in therapy for patients with metabolic syndrome. Walking and hiking in a mountain scenery represents an ideal approach to make them move. The Austrian Moderate Altitude Study (AMAS) 2000 main study is a randomized controlled trial to investigate the cardiovascular effects of hiking at moderate altitude on patients with metabolic syndrome compared with a control group at low altitude, to assess a potential altitude-specific effect.
Methods
Seventy-one male patients with metabolic syndrome were randomly assigned to a moderate altitude group (at 1700 m), with 36 participants, or to a low altitude group (at 200 m), with 35 participants. The 3-week vacation program included 12 hiking tours (4 per week, average duration 2.5 hours, intensity 55% to 65% of heart rate maximum). Physical parameters, performance capacity, 24-hour blood pressure, and heart rate profiles were obtained before, during, and after the stay.
Results
In both groups, we found a significant mean weight loss of −3.13 kg; changes in performance capacity were minor. Systolic, diastolic, and mean arterial pressures and circadian heart rate profiles were significantly reduced in both groups, with no differences between them. Consequently, the pressure-rate product was reduced as well. All study participants tolerated the vacation well without any adverse events.
Conclusions
A 3-week hiking vacation at moderate or low altitude is safe for patients with metabolic syndrome and provides several improvements in their cardiovascular parameters. The cardiovascular benefits achieved are more likely to be the result of regular physical activity than the altitude-specific effect of a mountain environment.
Keywords
Introduction
Patients with metabolic syndrome are characterized by a cluster of cardiovascular risk factors, including central obesity, dyslipidemia, hyperglycemia, and arterial hypertension. Many etiological components of the metabolic syndrome derive from a sedentary lifestyle. Therefore, first-line treatment consists of a more active lifestyle, based on regular physical activity, and restricted caloric intake. 1 Walking and hiking are sports activities of low to moderate intensity that can be performed even by patients with metabolic syndrome featuring obesity and poor cardiorespiratory fitness. Physicians should encourage these patients to be more active in both their daily life and during holidays. Walking and hiking in a mountain setting represents an ideal approach to enhance their physical activity. Although physical activity is proven to be beneficial, corresponding data assessing the cardiovascular effects of hiking are sparse for patients with metabolic syndrome.
Thus, the project Austrian Moderate Altitude Study (AMAS) 2000 was initiated years ago. An initial pilot study demonstrated the beneficial effects of a hiking vacation at moderate altitude on metabolic parameters, namely, insulin resistance and lipid metabolism. 2 Thereafter, the AMAS-2000 main study, a randomized controlled trial including a control group at low altitude, was designed for distinguishing altitude-specific and exercise-induced effects. The metabolic results obtained from this study were published previously. 3 Here, we present the cardiovascular effects of a 3-week hiking vacation at moderate altitude (1700 m) and at low altitude (200 m) on patients with metabolic syndrome. Owing to the potential influence of altitude, we expected different results between them.
Methods
Study Participants
Study participants were invited by a local newspaper and television report to take part in the Austrian Moderate Altitude Study. At the University Hospital in Innsbruck, 71 male nonsmoking subjects (median age 56 years, range 36–66) with metabolic syndrome according to the criteria of the Adult Treatment Panel III and the National Cholesterol Education Program were included in the study. The patients’ medication was left unchanged during the whole vacation. The project AMAS-2000 was approved by the Ethics Committee of the Leopold-Franzens-University of Innsbruck. All participants gave written informed consent before the study.
Study participants (n = 71) were randomly assigned to a moderate altitude (MA) group (1700 m in Obertauern, Austria, n = 36) or to a sea level (SL) group (200 m in Bad Tatzmannsdorf, Austria, n = 35). Both groups were examined according to an identical time table. 3 The baseline characteristics of the study participants are summarized in Table 1. In both groups, the 3-week vacation program was held in a comfortable resort hotel and included 12 moderate intensity hiking tours (4 tours per week and 3 rest days, mean duration of a tour approximately 2.5 hours, exercise intensity 55% to 65% of the individual heart rate maximum evaluated by the baseline stress test). Hiking tours were guided by health professionals in homogenous groups (7 to 10 persons), and moderate hiking intensity was individually controlled by heart rate monitoring. Both study groups had comparable and balanced nutrition. The average total caloric intake was calculated to be approximately 1800 kcal daily in both study groups. At several times, blood samples were taken and body weight, height, waist, and hip circumference were measured. 3
Baseline characteristics of the study participants
Values are means ± SD (no significant differences between groups).MA, moderate altitude; SL, sea level; OGTT, oral glucose tolerance test; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Ergometry
An incremental 25 W, 2-minute symptom-limited maximal exercise test was performed on a cycle ergometer ER 800 (Ergoline, Bitz, Germany) 10 to 14 days before the hiking vacation and 7 to 10 days and 6 to 8 weeks after the vacation.
Ambulatory Blood Pressure Monitoring And 24-Hour Electrocardiography
All patients underwent ambulatory blood pressure monitoring (Mobil-O-Graph, IEM, Sheffield, UK) and 24-hour electrocardiography (Delmar Model 363, Digitalrecorder 483, Fountain Valley, GA) on the first or second day and on the last 2 days of their 3-week vacation. By ambulatory blood pressure monitoring, systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial BP were recorded every 15 minutes during the daytime and every 30 minutes during the night. From the 24-hour electrocardiography we studied heart rate (HR), the number of ventricular premature beats, ST-segment changes, and episodes of bradycardia defined as HR less than 50 beats/min. The pressure-rate product (PRP [= SBP × HR]) was calculated afterward.
Statistics
A repeated measures analysis of variance was applied for the analysis of time dependence and group differences. Tukey’s post hoc test was used for intergroup comparisons at the individual time points. Arithmetic means and standard deviations are presented for descriptive analysis. For absolute and relative performance capacity and laboratory parameters, paired and unpaired Wilcoxon tests were applied. Statistical significance was assumed at a level of P less than .05. Data were analyzed by utilizing the STATISTICA software of Windows version 5.1.
Results
Study Participants
In both groups, there was a significant decrease in body weight. The reduction was −3.22 ± 1.91 kg in the MA group at the end of vacation, and −3.04 ± 2.16 kg in the SL group. Furthermore, there were significant improvements regarding body mass index, body fat, and waist circumference (P < .001) as well as in the laboratory markers for metabolic syndrome such as fasting glucose, total cholesterol, and low-density lipoprotein cholesterol, and so forth, which have been published previously. 4
Ergometry
Before the vacation, the mean absolute maximum power output (Wmax) was 190.5 ± 27.2 W in the MA group and 201.65 ± 41.83 in the SL group; the mean values of relative maximum power output (Wmax/kg) were 1.98 ± 0.32 and 2.09 ± 0.44, respectively. In the MA group, there was a slight but significant rise in maximal performance by 4% (Wmax = 197.73 ± 33.16) after the active holiday; the respective values for Wmax/kg increased by 7% to 2.12 ± 0.38 in the MA group (P < .001). In the SL group, there was no significant change in maximal performance. In both groups, the nonsignificant increases in relative power output can primarily be explained by the achieved loss in body weight (MA group body mass index, 31.67 ± 3.35 kg/m2 before and 30.86 ± 3.24 kg/m2 after; SL group body mass index, 31.19 ± 2.88 kg/m2 before and 30.5 ± 2.76 kg/m2 after; P < .05, respectively).
In addition to these slight improvements in power output, there were significant reductions in HR, SBP, and DBP at the submaximal stage of 100 W in the MA group, indicating favorable cardiac adaptation. In the SL group, no HR reduction could be seen at the submaximal work load of 100 W. The HR recovery was improved in both groups but was more pronounced in the MA group at the third and fifth minute of recovery. The results of the exercise tests are shown in Table 2.
Parameters of exercise testing in the moderate altitude group and sea level group at various time points a
HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; HRrec, heart rate recovery; V
Time 1, 10 to 14 days before vacation; time 2, 7 to 10 days after vacation; time 3, 6 to 8 weeks after vacation.
Within group, vs time 1, P < .001.
Within group, vs time 1, P < .05.
Within group, vs time 1, P < .01.
Ambulatory Blood Pressure Monitoring And 24-Hour Electrocardiography
The vacation had a BP lowering effect in both groups. There were reductions in SBP, DBP, and mean arterial blood pressure of −7.97 ± 10.18, −3.76 ± 6.74, and −5.43 ± 8.06 mm Hg, respectively, in the MA group; and −5.11 ± 7.84, −3.04 ± 5.25, and −3.79 ± 6.27, respectively, in the SL group. In Figure 1, a comparison of the BP characteristics before and immediately after vacation is given for both the MA group and the SL group. Although there were a few significant differences between the groups at single time points, no relevant difference in the circadian profile could be seen between them.
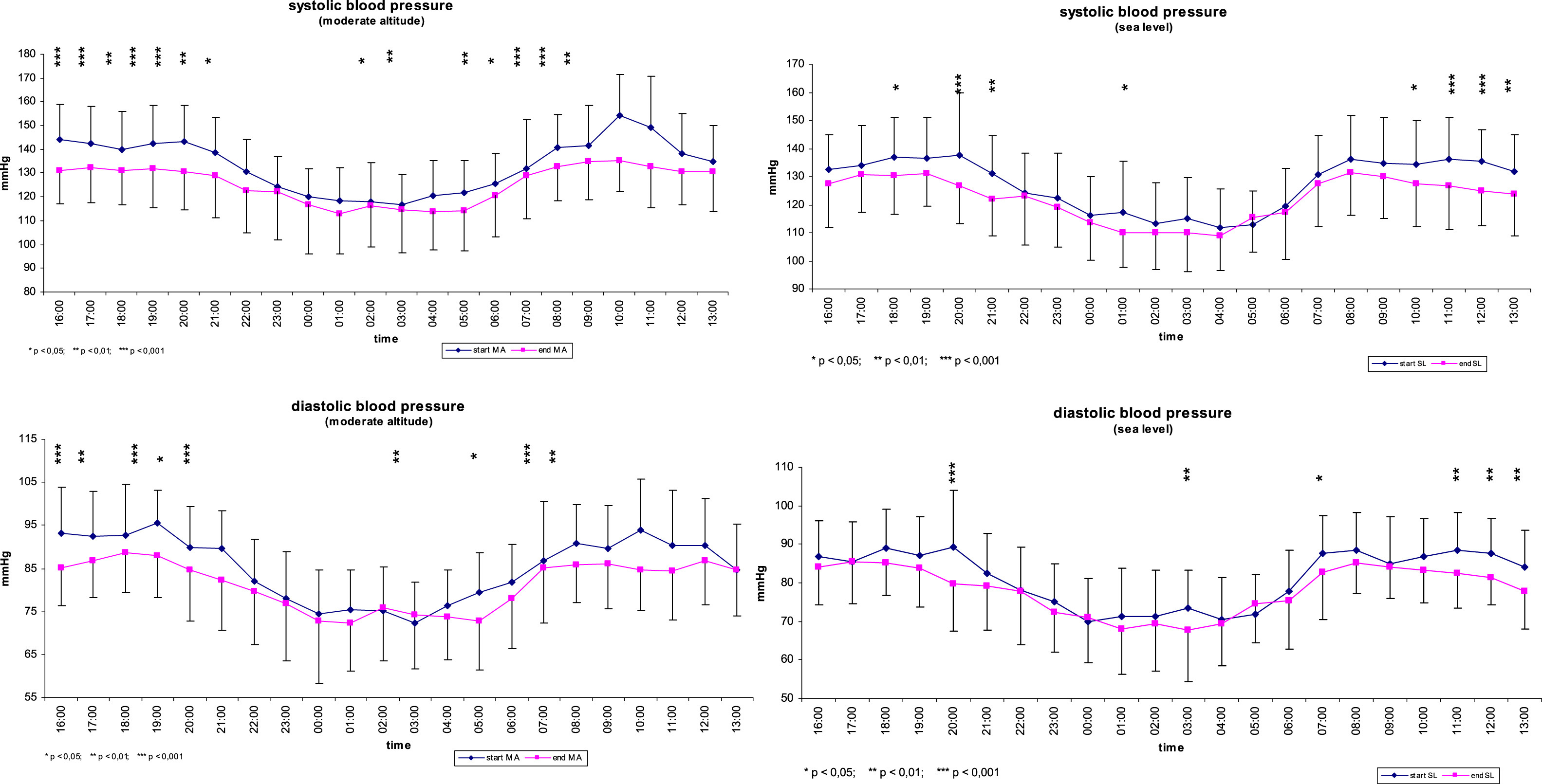
Results of ambulatory blood pressure monitoring for mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) at the start and at the end of the 3-week vacation in the moderate altitude (MA) group (left row [blue lines = start MA; pink lines = end MA]) and the sea level (SL) group (right row [blue lines = start SL; pink lines = end SL]).
In addition, the vacation had a HR lowering effect in both groups. The range of mean HR decrease was 5 beats/min in the SL group and 3 beats/min in the MA group, with unchanged characteristics of the circadian profiles. Even the number of ventricular and supraventricular premature beats and the extent of ST-segment changes were comparable between the groups. The PRP, calculated from the ambulatory BP monitoring and 24-hour electrocardiography data, was significantly lower at the end of the 3-week vacation in both groups, but congruent between them (Figure 2).
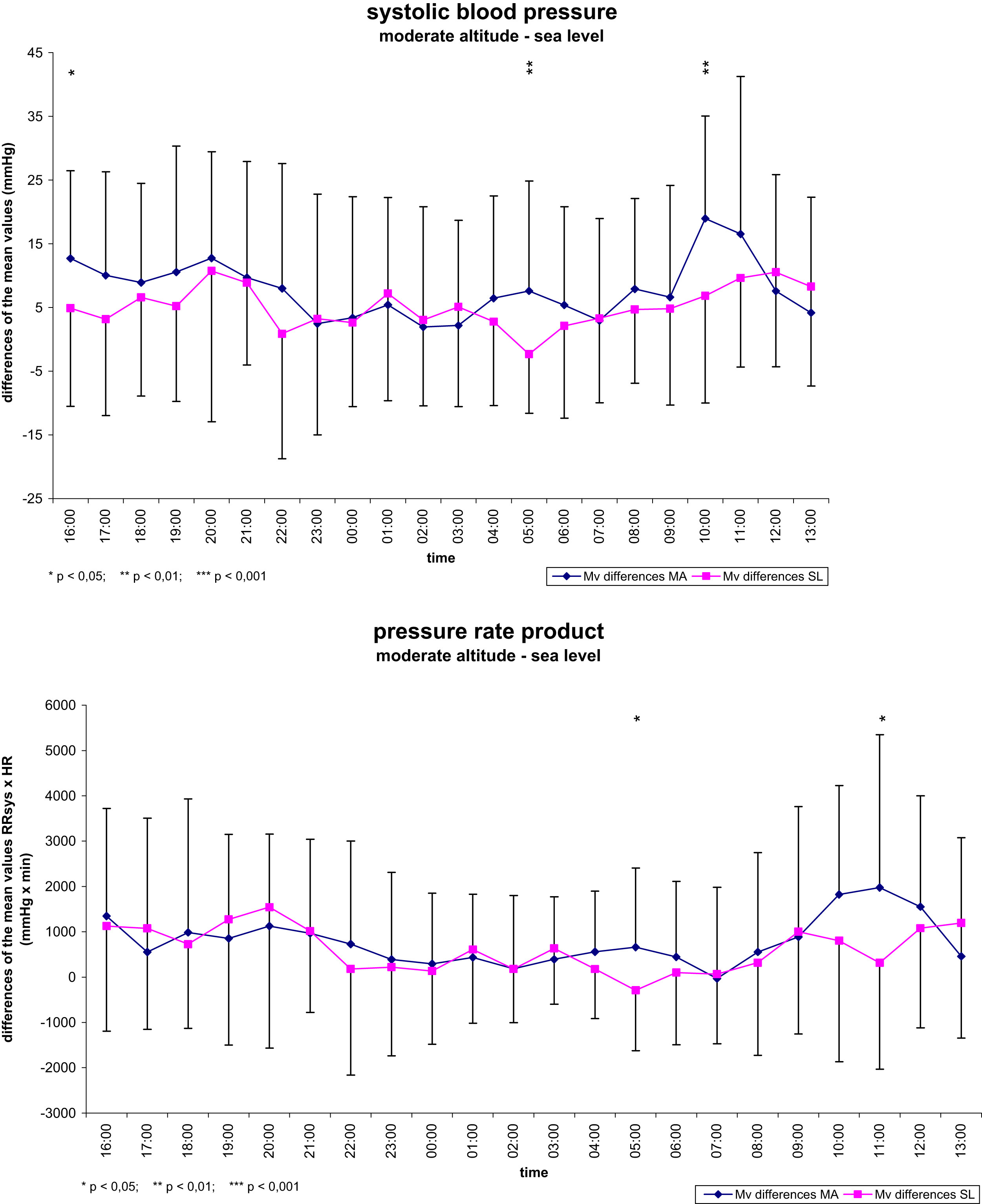
No differences in the circadian profiles of blood pressure and heart rate between the moderate altitude (MA) group (blue lines = start MA; pink lines = end MA) and the sea level (SL) group led to comparable pressure-rate products at the end of the 3-week vacation.
Discussion
The main findings of the AMAS-2000 main study (“cardiovascular part”) are 1) that a 3-week hiking vacation at moderate altitude is safe for patients with metabolic syndrome, and 2) that the achieved improvements in cardiovascular parameters are more likely to be the result of pronounced physical activity and recreational training than the altitude-specific effect of a slightly hypoxic environment.
Metabolic syndrome has become a major public health challenge worldwide, with increasing prevalence in both developing and industrial countries. 4 The roots of this “pandemia metabolic syndrome” lie in a sedentary lifestyle. In addition, physical inactivity and high caloric intake cause a positive long-term energy balance resulting in visceral obesity, insulin resistance with hyperinsulinemia, and an overdrive in sympathetic nervous activity, which all increase the patient’s cardiac risk. 5 Therefore, first-line treatment must implicate a change of lifestyle, namely, pronounced physical activity and restricted caloric intake.
Walking in general and hiking in mountain scenery are sport activities of low to moderate exercise intensity, and are simple and feasible for nearly everybody. Nevertheless, there is some concern whether physical activity under the slightly hypoxic conditions of moderate altitude is safe for patients with metabolic syndrome, which features an increased cardiac risk a priori. This doubt is based on registry data from Alpine regions showing an increased incidence of sudden cardiac death during hiking and skiing in adults aged more than 40 years.6,7 These epidemiological data revealed that the risk for sudden cardiac death was greatest on the first day at altitude, but altitude per se and the duration of activity did not appear to modify the risk. 6 The most important risk factor for sudden cardiac death was prior myocardial infarction. Moreover, unaccustomed physical activity seemed more likely to trigger sudden cardiac death than altitude per se. In both the AMAS-2000 pilot study and main study, all subjects tolerated the vacation very well, and adverse events did not occur. Therefore, we conclude that under controlled conditions, moderate holiday activities are safe at any altitude between 200 m and 1700 m above sea level even for patients with metabolic syndrome.
To answer the question whether the beneficial hemodynamic effects seen in the AMAS-2000 pilot study were altitude-specific or exercise-induced, we performed the AMAS-2000 main study, which included a control group at low altitude. At moderate altitude as well as at sea level, there was a significant reduction in systolic, diastolic, and mean arterial BP in both groups, with no differences between them. The extent of BP reduction seen in our study is comparable to the results of a large meta-analysis by Fagard. 8 In these pooled data, the weighted net reduction of SBP and DBP in response to dynamic physical training averaged 3.4/2.4 mm Hg, whereas it was even doubled in our study (MA group, 8.0/3.8 mm Hg; SL group, 5.1/3.0 mm Hg).
The HR profiles recorded in our study showed a slight decrease in the mean circadian HR as well. This significant HR reduction was seen in both groups in a comparable dimension. The decreases in the circadian BP and HR profile lead to a diminished PRP whose reduction may be of even short-term benefit. Recently, the Ohasama study demonstrated that a reduction in PRP has a very favorable long-term impact on mortality. 9 As we found no significant difference between the groups, we conclude that all favorable hemodynamic effects seen in the AMAS-2000 main study are the consequence of increased physical activity. Hiking was, moreover, beneficial for weight control. Owing to the increased energy expenditure and caloric restriction, all subjects lost weight (approximately −3 kg). In contrast, changes in performance capacity were slight. More pronounced improvements in fitness can obviously only be achieved by longer training periods and more individual training.
In conclusion, the data from the AMAS-2000 main study prove that daily hiking for hours at moderate altitudes or at any sea level beyond represents an excellent therapeutic opportunity for physical and mental regeneration even for persons with a cluster of cardiovascular risk factors. Thus, walking and hiking should be generally recommended as an essential procedure of lifestyle modification for patients with metabolic syndrome.
Footnotes
Acknowledgments
This project was partly supported by the Austrian Ministry of Economics, the Austrian Tourism Boards of Kärnten, Salzburg, Tirol, and Vorarlberg, the Austrian National Tourist Office, the Austrian Tourism Organization, the villages of Obertauern/Mauterndorf and Bad Tatzmannsdorf, and the Tiroler Landeskrankenanstalten GmbH.