
Abstract
Objective
We investigated the incidence and injury patterns of acute parachuting injuries evaluated at a level II military facility during a 5-year period to compile medical information that may assist in improving the safety of parachuting.
Methods
A retrospective chart review of all parachuting injuries that presented to the Madigan Army Medical Center emergency department in Tacoma, Washington, during a 5-year period from February 2005 to June 2011.
Results
A total 110 patient charts met inclusion criteria. Lower extremity injuries made up 65% of total injuries, followed by 22% head injuries, 22% neck or back injuries, and 19% upper extremity injuries. One patient died in the emergency department of head injuries, and 1 patient was transferred for an open-book pelvic fracture. The most common phase of the jump in which to sustain injury was at landing. A total of 15 patients were admitted to the hospital. It is of note that some patients had combined injuries. The mechanism of injury documented in 96 of 110 (87%) patients and 10 of 15 (66%) admitted patients was a difficult landing.
Conclusions
The rate of injury for each area of the body is within previously reported rates, with lower extremity injuries making up the largest category and leading to the majority of admissions. The most common time to sustain an injury was during landing, which represented a majority of both emergency room visits and hospitalizations.
Introduction
Parachuting has been used throughout military history as an effective means of distributing troops to an area of operation. Although this means of deploying troops is quite efficient, there have been significant injuries associated with this method of transportation. In a sentinel study of military parachuting injuries, Kirby 1 suggests it is expected that 0.5% of paratroopers jumping would not be able to carry out their mission owing to injuries. He suggests that poor landing grounds, high wind speeds, and heavy gear contribute to landing injuries that would make soldiers unfit for completing their mission. According to Knapik et al, 2 this risk has been found to be increased by wind speeds over 15 miles/h, landing in trees, colliding with the ground, parachuting at night, experiencing pendulum oscillations caused by the parachute, and by the parachutist being dragged across the ground after landing because of high winds. A study by Kotwal et al 3 examining 4 static line airborne missions conducted by US Army Rangers involving 634 jumpers identified a 12% injury rate with 4% (76 soldiers) requiring medical evacuation and 2% of the soldiers (n = 11) requiring surgical intervention. This study identified an 8-fold increase in the percentage of soldiers who were not able to continue the mission as a result of static line parachuting injuries. 3 Although these studies identify factors associated with sustaining injury and incidence of injury, no study has identified the injury patterns associated with static line parachuting.
In military parachuting operations, troops are deployed at low altitudes using a static line parachute, in which the parachutist hooks his or her parachute into a line that deploys the parachute on exiting the plane (Figure 1). Military operations in particular often deploy troops from both sides of the plane in a procedure termed CAPES (controlled alternating parachute exit system) to deploy a large amount of troops over a small drop zone and decrease the chances that troops become entangled with each other. 2 These deployment techniques, unique to military operations and smokejumpers from the Bureau of Land Management (BLM) and Forest Service, put paratroopers at risk of static line injuries that may result in neck and upper extremity injuries related to discharge from the plane.4, 5 This is in contrast to civilian injuries, which incur the added risk of free falling from a higher altitude than static line parachuting. Free fall parachutists (sky divers) are responsible for deploying their own parachute. 6 Although the military also performs free fall jumps, albeit in much smaller numbers, the static line jump is the primary means of parachuting for mass troop deployments. It is for this reason that we investigated the incidence and characteristics of static line parachuting injuries to determine and describe injury patterns sustained and to use such information to improve identification and treatment of such injuries and possibly mitigate injury in subsequent operations.

Paratroopers exiting alternately from both rear doors of an aircraft during a static line parachute operation.
Methods
Study Design
We did a retrospective chart review of all patients who presented to the Madigan Army Medical Center emergency department from February 2005 to June 2011 by searching our electronic medical record system, Essentris, for the clinical data of emergency department patients who sustained acute traumatic parachuting injuries. The medical record system was searched using the terms paratrooper, parachuting, parachute, and trauma in multiple fields of the medical records. Inclusion criteria for the study were acute traumatic parachuting injuries related to airborne training in the aforementioned 2005 to 2011 time frame. Injuries documented in trauma notes, progress notes, radiographic studies, and discharge summaries were included in the study. Exclusion criteria for the study included patients younger than 18 years and injury that was not sustained during an actual parachuting episode. Patients who presented with nonacute problems related to parachuting injuries, considered greater than 1 week since the parachuting operation, were excluded from the study. We extracted the phase of the parachuting operation in which the patient incurred injury by breaking the jump down into 3 phases: 1) exit of the aircraft until parachute deployment, 2) descent once the canopy opened, and 3) landing. A standardized database was then used to compile information that included chief complaints, injuries sustained, hospital course, and patient disposition. Using this information we were able to summarize the incidence and injury patterns of these patients with their ultimate medical dispositions (Table 1).
Patient characteristics
Results
A total 110 patient charts met inclusion criteria, with 109 (99%) of those identified as military jumps. One patient presented after a parachute jump without identifying whether that jump was a static line or free fall. That patient was discharged with the diagnosis of ankle sprain. A total of 140 injuries were identified among the 110 patients, with lower extremity injuries sustained on landing comprising the majority. Ninety-six of the 110 patients (86%) were injured at landing, with 71 patients (65%) sustaining lower extremity injury. Twenty-three patients (22%) sustained head injuries, with 2 of those being intracerebral hemorrhage. Spine and upper extremity injuries constituted 19% of injuries, with 22 spine and 21 upper extremity injuries, respectively (Figure 2).
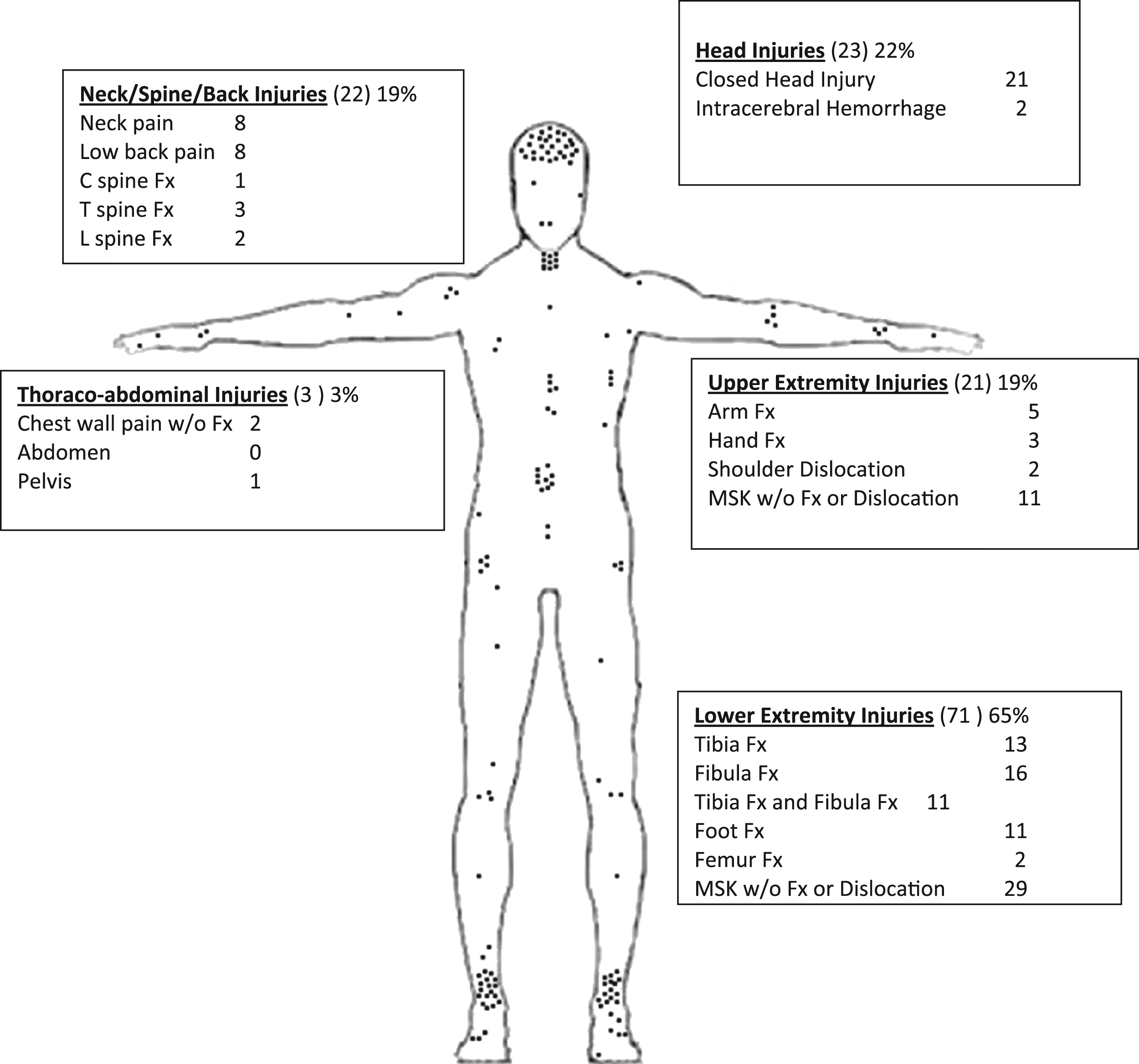
Distribution of injuries: body region (total reported injuries), percent of 110 patients with injury within body region. Fx, fracture; MSK, musculoskeletal.
Fifteen patients (14%) were admitted to the hospital, 1 died in the emergency department of head injuries, and 1 was transferred with an open-book pelvic fracture. Thirteen of the 15 admitted patients were injured during the landing phase of the jump. The patient who sustained a pelvic fracture became entangled in another jumper’s parachute during the descent phase of the jump and landed abnormally at a high rate of speed without adequate parachute canopy. Although the injury occurred as a result of landing, the precipitating factor occurred during descent. The other entangled patient died of head injuries. A second patient, admitted patient number 13, sustained a femur fracture as a result of getting his legs caught in his parachute as it opened (Table 2).
Admitted patient characteristics
CHI, closed head injury; Fx, fracture; ICH, intracerebral hemorrhage; LE, lower extremity; MSK, musculoskeletal.
Discussion
This review may serve to aid those medical providers and first responders who provide medical coverage to static line parachute operations. The relevance of military to civilian parachuting deserves further attention. The first thing to take into consideration is that static line or low-altitude jumping are not styles unique to the military. A similar application is found in the civilian world in firefighting. Smokejumpers are deployed from the air to the ground in forward areas to fight forest fires. Like military parachuting, this style of airborne deployment is by static line, and even more commonly under less than ideal conditions. The BLM and the Forest Service both employ smokejumpers who are static line parachutists. Nationally, there are about 325 Forest Service and 145 BLM smokejumpers working primarily in the western United States and Alaska. Smokejumpers are the only federal firefighting group to keep accurate injury reports since 1992. The national rate of injury for Forest Service smokejumpers performing parachute operations is on average 0.7% or 7 per 1000 jumps. 7 This is similar to the 0.5% rate of injuries forecasted during military parachuting and much lower than the rates identified by Kotwall et al 3 among Army Ranger jumps in Afghanistan and Iraq. Although the specific injuries of smokejumpers were not reported, one assumes that the injury type and distribution would mirror military parachuting.
For that reason, this paper may provide useful information for regions that use smoke jumping to fight wildfires. The next commonality between civilian and military parachutists is that proper landing technique is pivotal in avoiding injury. Dedicated studies focused on improving landing safety with different equipment design and safety gear (such as previously evaluated ankle braces) would likely be high yield. Better carrying techniques for other equipment such as rucksacks (packs) could also be explored. In addition, the prevention of head injury in parachuting has not been as thoroughly explored as prevention of ankle injuries, and recent military focus on traumatic brain injury prevention and treatment may be useful when applied specifically to parachute injuries in both sectors.
Our overall impressions are that although parachuting techniques may vary between military and civilian organizations, the overriding principle is that orthopedic and closed head injuries continue to be the most common injuries and that landing continues to be implicated as the culprit of most parachuting accidents. Parachute training and equipment design that focuses on these areas will likely be most beneficial. Medical facilities near popular parachuting areas may wish to focus on access to orthopedic care as well as adequate follow-up for closed head injuries and musculoskeletal injuries to optimize patient care.
Conclusions
The rate of injury for each area of the body is similar to previously reported rates, with lower extremity injuries making up the largest category, leading to 66% of admissions. Rate of upper extremity injury was at the upper limit of previously reported rates in military parachuting (0–14.5% shoulder and 0–5% for arm injuries). The most common time to sustain an injury was during landing, which represented a majority of both emergency room visits and hospitalizations (87% and 66%, respectively). There were a few important limitations in this interpretation of the data. First, we are not able to comment on the rates of injury as we have no ability to identify the total number of static line parachute jumps that took place during the study period.
Based on the retrospective design of this study, we cannot reliably state that a hard landing or poor landing technique caused these injuries, although an association is clearly seen. Because Army special operations units typically conduct parachute operations in smaller groups, they commonly jump from an opened cargo ramp in single file with the parachute deploying from the jumper’s rear instead of his or her side as happens during CAPES. One could expect a higher rate of upper extremity injuries on exiting the aircraft in units that solely conduct CAPES. Patient charts did not identify whether jumps were from the cargo ramp or CAPES. Only 1 patient was injured on exiting the aircraft when his head struck the aircraft. This is fairly common during CAPES but almost impossible during a jump from a cargo ramp.
There was no information available in the charts that detailed the background parachuting experience of each individual jumper. Because all of these charts were presumably from Army special operations groups as no other type of unit or civilians perform static line parachute jumps from the base, these soldiers would have needed at least 5 prior jumps to be a part of the group parachuting exercise. As such, there is a possibility that some of these soldiers had fewer than 10 lifetime static line parachuting jumps, with others having hundreds. Therefore, further information regarding injuries sustained versus number of prior jumps would also be helpful. We were able to identify the age of each patient, and as expected, the youngest age group, 20- to 29-year-olds, represented 46% of patients.
Footnotes
☆
Disclaimer: The opinions or assertions contained herein are the private views of the authors and are not to be construed as official statements or perspectives reflecting the views of the Department of the Army or the Department of Defense.