
Abstract
Objective
Altitude illness can occur in anyone who ascends to high altitude. Better understanding of altitude illness is associated with a lower incidence of acute mountain sickness (AMS). The purpose of this study is to compare, for the first time, the incidence and understanding of altitude illness between foreign trekkers and indigenous porters in Nepal.
Methods
Interviews and questionnaires were completed at the International Porter Protection Group Rescue Post at Machermo (4470 m). Participants completed the Lake Louise acute mountain sickness self-assessment questionnaire. They were also asked about their actions in response to high altitude illness scenarios as well as their perception of the vulnerability of porters vs trekkers to altitude illness. Ascent profile, age, gender, ethnic origin, and altitude of home residence were also obtained.
Results
Trekkers (n=131) had a significantly higher incidence of AMS (21% vs 8%) than porters (n=92; P < .02). Lowland porters (whose home villages were below 3050 m, n=61) had a numerically higher, though not significantly different, incidence of AMS (10% vs 3%) compared to highland porters (n=31). The majority of trekkers and porters recognized the symptoms of altitude illness and the most appropriate action to be taken. Despite the lower incidence of AMS in porters, around half felt that they were at greater risk than trekkers.
Conclusions
Porters had a lower incidence of AMS, which may be attributable to repeated ascents through the trekking season, or differences in reporting symptoms. Both trekkers and porters demonstrated appropriate knowledge of actions to be taken in response to altitude illness.
Acute mountain sickness (AMS) is a condition that can occur in anyone who ascends to high altitude. 1 It is relatively benign, but more rapid ascent can lead to life-threatening conditions such as high altitude pulmonary edema (HAPE) and high altitude cerebral edema (HACE).2,3 Acute mountain sickness not only affects foreign visitors but also members of the indigenous population, young and old, who normally reside at low altitude and ascend for work, recreation, or religious activities. 4 –6 The incidence of AMS in the Himalayas has been shown to range from 14% to 53% in foreign visitors, and 0% to 12% in the indigenous population. 5 ,7,8 Acute mountain sickness is best prevented by adopting a slow ascent profile. 1 Although recommendations vary, the Wilderness Medical Society has recently issued consensus guidelines advising ascent of no more than 500 m per day and a rest day after 3 or 4 days of ascent. 1 Unfortunately, recommendations such as these are not always widely appreciated.9,10 However, there is real potential for health improvements to be made when information is available. This is supported by recent studies demonstrating reduced AMS incidences in foreign visitors who have a better understanding of altitude illness than their predecessors.11,12 The impact of education on an indigenous population in the Himalayas warrants further investigation.
The purpose of this study is to compare the incidence and understanding of AMS between foreign trekkers and indigenous porters on a popular trekking route in the Solu Khumbu region of Nepal.
Methods
Setting
Data collection took place over a 6-week period, during Spring 2008, at the International Porter Protection Group (IPPG) Rescue Post and Porter Shelter at Machermo, a small settlement in the Solu Khumbu region of Nepal, situated at an altitude of 4470 m. Recruitment of trekkers occurred before the daily altitude lecture; porters staying in the porter shelter were invited to complete the questionnaire via a translator.
Assessment of acute mountain sickness
Acute mountain sickness was diagnosed using the Lake Louise AMS self-assessment score. 13 A diagnosis of AMS was made on the basis of headache with AMS score of ≥ 3, and severe AMS was defined as an AMS score of ≥ 5. Anyone who fulfilled the criteria for AMS was offered a consultation and treatment.
Questionnaire
Demographic data obtained included age, gender, ethnicity, location of the 3 previous nights' sleep, and altitude of permanent residence. Subjects who were descending were excluded.
Three questions (see Table 1) elicited knowledge of high altitude illness. These were in multiple choice format to simplify data collection and analysis. Question 1 is a scenario involving AMS, a self-limiting illness which requires rest at the same altitude until symptoms disappear. Question 2 indicates probable HACE and HAPE and, thus, requires immediate descent.
Questions regarding altitude illness
Statistical Analysis
Incidence of AMS between porters and trekkers and between high altitude and low altitude porters was compared using a χ2 test. Yates' correction for small sample size was used when comparing high and low altitude porters. The difference in mean ascent rates was compared using a t test. P values of < .05 were considered statistically significant.
Results
Demographics
Ninety-two porters and 131 trekkers participated in the study. The porters were all male and had a mean age of 27.1 (SD 9.9). The trekkers were 64% male with a mean age of 44.1 (SD 13.1).
The porters were mainly (67%, n=61) from the Rai ethnic group. This is a group from the middle hills south of Lukla (ie, not high altitude residents). Only 4% of the porters (n=4) were Sherpas, the high altitude group of the Solu Khumbu. The remainder of the porters were Chhetri (n=14), Bisokarma (n=4), Magar (n=4), Tamang (n=3), Nepali (n=2), and Brahmin (n=1). Traditionally, Magar, Tamang, and Rai are middle hills groups, and Chhetri, Bisokarma, Nepali, and Brahmin are lowland groups, but ethnic groups in Nepal overlap geographically and, therefore, porters were classified as being from high altitude if rice did not grow in their home village (since rice does not grow in significant quantities above 3050 m). 14
Trekkers were predominantly Caucasian (93%) and all resided below an altitude of 2300 m (mean 190 m ± SD 404 m).
Ascent profile
Mean ascents for the previous 3 days are shown in Table 2. The data is complicated by the recommendation to spend 2 nights in Namche Bazaar (3440 m). If trekkers/porters had ascended to Machermo from Namche in 2 days, then they usually had no height gain for the 24 hours prior to this. Porters had significantly greater height gain compared to trekkers in the 24 and 48 hours prior to arrival in Machermo (P < .001).
Mean height gain (s.d.) in metres in the 24, 48 and 72h prior to arriving at Machermo
The incidence and knowledge of AMS
The incidence of AMS was greater in trekkers than porters (P < .02). There was no statistically significant difference in the incidence of AMS between the low and high altitude porters (P < .5).
Responses to questions are illustrated below.
Nearly all the porters and trekkers chose safe responses to question 1. Seventy percent of trekkers and 71% of porters chose the only safe option (immediate descent) to question 2. Most trekkers (84%) thought both groups were equally vulnerable to altitude illness, whereas half the porters felt they were at greater risk.
Discussion
The key findings of this study are that the incidence of AMS was greater among trekkers than porters surveyed at the IPPG, and that the majority of both groups recognized the appropriate action to take when presented with a scenario of someone suffering from altitude illness.
Porters had a significantly lower incidence of AMS than trekkers, at 8% vs 21% (P < .02) (see Table 3). This is despite having a significantly faster ascent rate in the previous 24 and 48 hours (P < .001). As discussed above, since the data was collected over a 6-week period, the porters were likely to be pre-acclimatized from multiple trips later in the season. Also, a porter from a middle hills village at 2000 m, where inspired PO2 is 117 mm Hg, will still have some advantage over a trekker from sea level, where inspired PO2 is 149 mm Hg. It is also possible that there are differences in reporting symptoms between the 2 groups; trekkers may over-report symptoms due to lack of familiarity with a more challenging environment or a desire to seek medical treatments, whereas porters may be reluctant to admit symptoms due to concerns about losing employment if suffering from altitude illness. This financial pressure was illustrated during our study when 3 porters with AMS (one of whom had an AMS score of 6) declined to accept medical advice to rest at Machermo (4470 m) and, instead, opted to continue to carry loads to Gokyo (4790 m).
The incidence of AMS and Severe AMS amongst porters and trekkers attending the IPPG Rescue Post at Machermo
A difference in the incidence of AMS between porters and trekkers has been previously described in the Himalayas. 7 Basnyat and Litch found evidence of AMS in 8% of porters and 14% of trekkers who had shared the same ascent profile during a 22-day trek around the world's eighth highest mountain, Manaslu. 7 Hillenbrand et al found a greater incidence of AMS in those porters who were born below 2500 m (16.1% vs 0%) while ascending to Lobuche (4930 m) from Namche Bazaar (3440 m). 5 Although we were unable to demonstrate a statistically significant difference in our study, possibly due to small sample size, we showed a trend towards a higher incidence of AMS (10% vs 3%) in those who permanently resided below 3050 m (see Table 3).
While time spent at altitude may offer porters some protection, it is clear from this study that AMS does still occur, and education of trekkers about their porters being vulnerable to AMS should remain a priority.
In response to the scenario questions, the vast majority of porters and trekkers chose safe options regarding the correct approach to treating AMS (question 1, Figure 1). Porters were ostensibly more cautious, and a greater proportion chose to descend rather than rest at the same altitude. However, as described above, financial pressures may prevent them from making the same decisions in real life. Regarding the correct approach to treating HACE/HAPE (question 2, Figure 2), the majority of both porters and trekkers chose the safe option of descending immediately; of concern, however, is that approximately a third of both groups chose to delay descent, which could be potentially life-threatening.
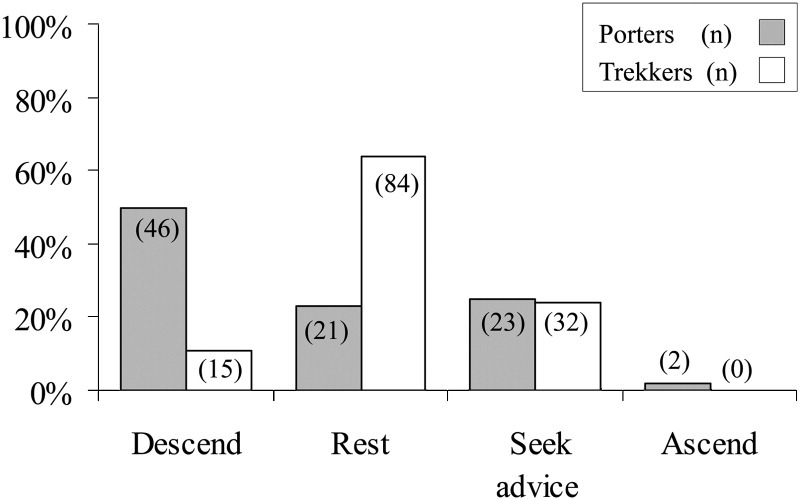
Responses to AMS scenario.
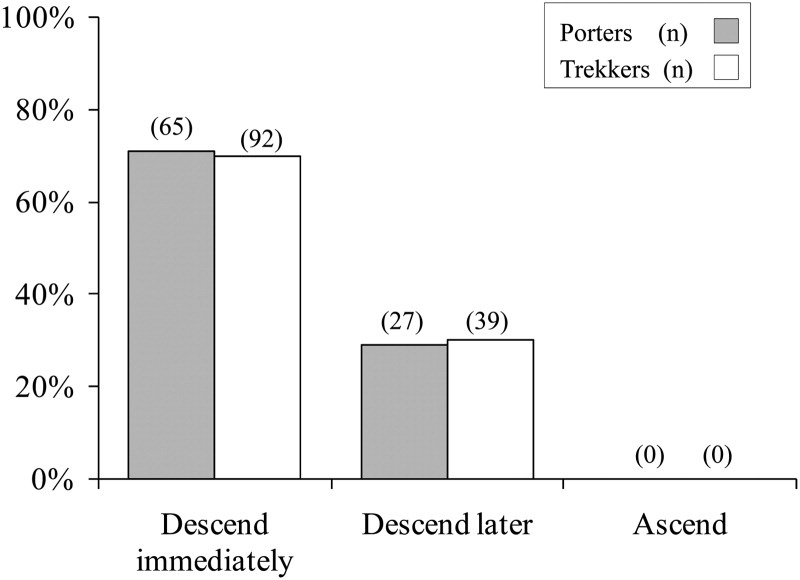
Responses to potential HACE scenario.
Trekkers' and porters' knowledge of altitude illness is likely to reflect, in part, greater availability of information such as signs put up on the trail by Khunde Hospital, the HRA, and the IPPG, as well as extensive information in the medical sections of guidebooks. Porters who have previously passed through the rescue posts may have attended talks or seen the educational video, “A Porter's Story.”
Previous studies have described the impact of education on Western trekkers. In an observational study conducted on 2 separate groups of 500 trekkers 12 years apart, Gaillard et al found that the incidence of AMS in the Annapurna region had fallen from 43% to 29%. 11 Importantly, this not only coincided with an increase in AMS awareness but also the use of AMS prophylaxis and, crucially, a slower ascent profile. Vardy et al conducted a questionnaire-based study of 130 trekkers that demonstrated an association between increased incidence of AMS and imprudent answers to scenarios similar to those used in this article. 12
One interesting difference between the 2 groups was seen in the perception of who was at greatest risk of developing AMS (question 3, Figure 3). It is interesting that porters regard themselves as being more vulnerable to altitude illness than trekkers, though in actual fact they reported less AMS.
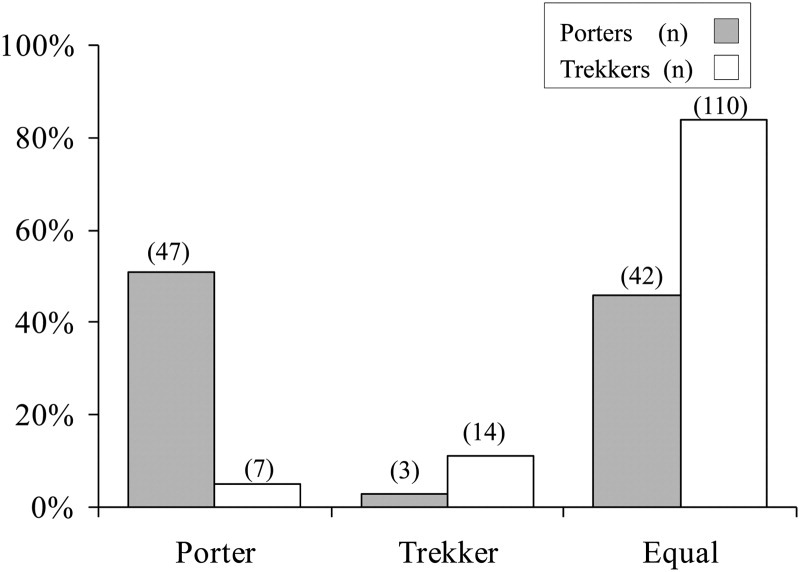
Perceived vulnerability to altitude illness.
Following long periods of time in the mountains, many porters will have seen cases of high altitude illness in family, friends, and colleagues. Unfortunately, in many cases their access to diagnostics, medication, and means of evacuation are more limited than those of trekkers, particularly in other trekking regions that do not have the facilities of the IPPG Rescue Post.
Porters do not have control over ascent profiles and, as observed during this study, are reluctant to admit symptoms to their employers since not ascending with their clients would mean loss of earnings. Perhaps these are some of the reasons contributing to their perceived increased vulnerability.
Limitations
While porters were recruited from the porter shelter and, thus, were likely to be enlisted sick or not, trekkers had to be motivated and well enough to leave their lodge to attend the daily talk. This likely contributed to an underestimation of the incidence of AMS in trekkers.
Porters often work on many treks during a season and are, therefore, likely to benefit from greater acclimatization later in the season. This factor was not accounted for. If repeating the study, it would be ideal to include only porters for whom this was the first trek of the season, or to account for previous treks and possibly observe a downward trend in AMS as the season went on. A seasonal trend has not been reported in the literature, but Hillenbrand et al found that the incidence of AMS in porters on an ascent to Lobuche (4930 m) was lower in those who had spent a week or more waiting for work in Lukla (2804 m) compared to those who had just arrived (5% vs 11%). 5
Finally, we did not take into account the use of acetazolamide prophylaxis, which would have reduced the incidence of AMS and was more likely to be used by trekkers.
Conclusions
To ensure that the incidence of AMS is kept to a minimum, education will need to continue. Information may be disseminated in lectures, guidebooks, magazines and, more recently, a booklet produced by the UK-based charity Medical Expeditions regarding altitude travel that is available as a free download in a number of different languages, including Nepali (
If information on the prevention, diagnosis, and treatment of altitude illness is made freely available to porters and trekkers in all high altitude trekking regions of the world, it may be possible to further reduce the incidence of altitude illness and to prevent a catastrophic outcome should serious altitude illness arise.
Footnotes
Acknowledgments
Sincere thanks to all the trekkers and porters who took part in the study. Thanks also to the staff at the IPPG post, Kanchha Rai and Chhewang Sherpa, for looking after their medics so well. Finally, many thanks to Dr. Cheryl Tallon who continued to recruit trekkers during the time that the first author was away from the post.
This work was previously presented at the Oxford Hypoxia Symposium, Oxford, UK, December 2008.