
Abstract
Objectives
Sildenafil and, recently, bosentan have been reported to increase arterial saturation and exercise capacity at altitude. The mechanisms behind this are still poorly defined but may be related to attenuation of hypoxic pulmonary vasoconstriction (HPV) and improved gas exchange. This study was designed to examine and compare the effect of sildenafil and bosentan on pulmonary gas exchange during acute hypoxic exercise in a controlled laboratory setting.
Methods
Sixteen athletic university students (8 males, 8 females) were examined during exercise in a hypoxic chamber (11% oxygen) before and after the administration of either sildenafil (n=10) or bosentan (n=6). Respiratory and metabolic measurements were taken at rest and during increasing exercise intensity (up to 90% of their individual maximal oxygen uptake [V̇O2max]) in concert with arterial blood gas sampling.
Results
Both drugs resulted in small, but significant increases in arterial PO2 (2–3 Torr) and O2 saturation (3–4%) at rest and during hypoxic exercise, in both men and women. No significant changes in arterial PCO2 or ventilation were seen at rest or during exercise in hypoxia; however, heart rate (both at rest and during exercise) was increased with both sildenafil and bosentan in both men and women.
Conclusions
These data demonstrate that sildenafil and bosentan equally improve arterial oxygenation in acute hypoxia in both men and women, which could account for improved physical performance at altitude.
Introduction
Sojourners to high altitude (> 3000 m) typically experience hypoxemia and exercise intolerance. Under resting conditions, the alveolar-arterial PO2 difference (A-aDO2) is often unchanged (or normal) at high altitude, indicating that hypoxemia is due to reduced inspired PO2 without impairment in gas exchange. However, even during light physical activity at high altitude, the A-aDO2 becomes widened due to O2 diffusion limitation and greater ventilation/perfusion mismatching that progressively worsens with increasing work intensity. 1 -3 Pulmonary arterial hypertension and subclinical pulmonary interstitial fluid accumulation are among the mechanisms believed to be responsible for ventilation/perfusion mismatching and O2 diffusion limitation during hypoxic exercise. 1 -4
It has long been recognized that exposure to high altitude results in hypoxic pulmonary vasoconstriction (HPV), which is characterized by increased pulmonary arterial pressure (PAP) and greater pulmonary vascular resistance (PVR) due to hypoxia-mediated smooth muscle contraction in the pulmonary vasculature. In pathological conditions, where alveolar hypoxia may occur in localized lung regions, HPV is a useful adaptive mechanism to divert blood flow away from poorly ventilated lung areas and preserve pulmonary blood flow to well-ventilated areas of the lung. In contrast, at high altitude (where the entire lung is hypoxic), excessive HPV can be detrimental, resulting in increased PAP and leading to high altitude pulmonary edema (HAPE)—a condition that impairs gas exchange because of fluid accumulation in the alveoli and may be fatal if left untreated. 5 -7 Moreover, increased pulmonary arterial resistance may limit exercise capacity by limiting right ventricular afterload.
Sildenafil is a selective phosphordiesterase-5 inhibitor that dilates the pulmonary vascular bed by increasing intracellular guanosine 3',5'-cyclic monophosphate (cGMP), relaxing vascular smooth muscle in pulmonary arterioles, and has been shown to be beneficial in the treatment of patients with primary pulmonary arterial hypertension. 8 -11 Similarly, bosentan, a nonselective endothelin receptor antagonist preventing endothelin-1-triggered vasoconstriction in the lung, is also used in treating patients with primary pulmonary arterial hypertension. 12 -14 Recently, a single oral dose of bosentan has also been shown to reduce hypoxia-induced increases in PAP in healthy individuals exposed to acute hypoxia. 15 Both drugs have been shown to improve exercise capacity in patients with primary pulmonary arterial hypertension 9 ,16,17 and, as such, either drug may also be useful in treating or reducing HPV and/or HAPE. 11 ,18-21
Several altitude field studies have reported improved exercise performance with oral administration of sildenafil in healthy humans at high altitude and have shown improved blood oxygen saturation measured via pulse oximetry (Table 1). 22 -24 However, to date, only Richalet et al 23 have reported arterial PO2 (PaO2) measurements during exercise at real altitude and, here, PaO2 is only reported at ventilatory threshold after 2 and 5 days at high altitude following some acclimitization. Since it is well-established that pulmonary gas exchange is impaired during exercise under acute hypoxic conditions—manifesting as a reduced PaO2 and a widening A-aDO2—we sought to determine whether taking either sildenafil or bosentan would improve arterial oxygenation and pulmonary gas exchange during acute exposure to hypoxia. We hypothesized that pulmonary vasodilation, via sildenafil or bosentan, would improve pulmonary gas exchange during acute hypoxic exercise, resulting in a greater PaO2 and SaO2 and a reduced A-aDO2 compared to the same level of exercise in hypoxia without either drug. Furthermore, because of the burgeoning interest in gender-based differences in gas exchange during exercise, 25 -28 we also compared the drug treatment responses between our male and female subjects.
Effect of phosphodiesterase-5 inhibition on exercise performance
Each “+” symbol represents improved exercise perfomance compared to placebo group.
+ = <10% improvement, ++ = 10-20% improvement, +++ = 20-30% improvement, — = no change.
Methods
Subjects
This study was approved by the Human Subjects Ethics Committee at Innsbruck Medical School and conducted in accordance with guidelines outlined in the Declaration of Helsinki.
A total of 16 subjects (n=8 males, n=8 females) were recruited and provided informed consent prior to participating in a single-blinded repeated-measure (no-drug/drug) exercise study. Young athletic university students with no significant medical history were randomly allocated to either the sildenafil (total N=10; n=5 males, n=5 females) or bosentan (total N=6; n=3 males, n=3 females) group.
Initial screening and maximal exercise testing
Subjects provided a brief medical history and were screened for cardiovascular (3-lead ECG) and pulmonary (spirometry) disease prior to testing. Each subject performed 2 exercise tests measuring maximal oxygen uptake (V̇O2max), one in normoxia and one in hypoxia (fraction of inspired oxygen [FIO2] = 0.11%) while riding an electronically braked cycle ergometer (Ergometrics 900, Ergoline, Germany). Tests were performed on separate days (no more than 2 days apart) and all hypoxic testing was performed in a commercially available normobaric hypoxic chamber (Hypoxico Inc, New York, NY, USA). Subjects were outfitted with a face mask; measurements of minute ventilation (V̇E), O2 consumption (V̇O2), CO2 production (V̇CO2), and respiratory exchange ratio (RER) were taken and calculated using Jaeger Oxycon Mobile (Viasys Healthcare Inc., Jaeger, Hoechberg, Germany) equipped with wireless telemetry to a desktop computer. Initial workload for each maximal exercise test began at 50 watts (25 watts for females) and was increased by 25 watts at 1 minute intervals until volitional fatigue occurred. Maximal oxygen uptake was defined as the highest V̇O2 achieved during the final workload and it was used to establish the submaximal workload for steady-state exercise before and after drug treatment.
Drug treatment and exercise protocol
Subjects returned to the laboratory within 1 week of the maximal exercise testing to perform submaximal pre-/post-drug exercise at light, moderate, and heavy work intensities (which corresponded to 15%, 45%, and up to 90% of V̇O2max) in hypoxia (FIO2 = 0.11) while arterial blood gases and metabolic measurements (V̇O2, V̇CO2, RER and V̇E) were obtained (Figure). Subjects breathed through a face mask fitted to a non-rebreathing valve (Hans-Rudolph 2700, Kansas City, MO, USA) whose expiratory end was connected to a heated mixing box. Each exercise workload was maintained for approximately 5 minutes, with the exception of the last workload, which only lasted about 3 to 4 minutes (based on the subject's ability to complete this near-maximal workload). Blood samples were collected in duplicate at rest and during the last 1 to 2 minutes in each exercise workload. The same exercise was performed before and 1-hour after taking a single oral dose of either sildenafil citrate (50 mg tablet) or bosentan (62.5 mg tablet) on the same day (Figure). Subjects were only admitted into one treatment group and were not informed which drug they were given. They were required to rest for at least 2 hours (in room air) between the 2 identical hypoxic exercise tests (ie, pre-drug and post-drug). Ingestion of the drug occurred 1 hour prior to the second exercise bout (Figure).
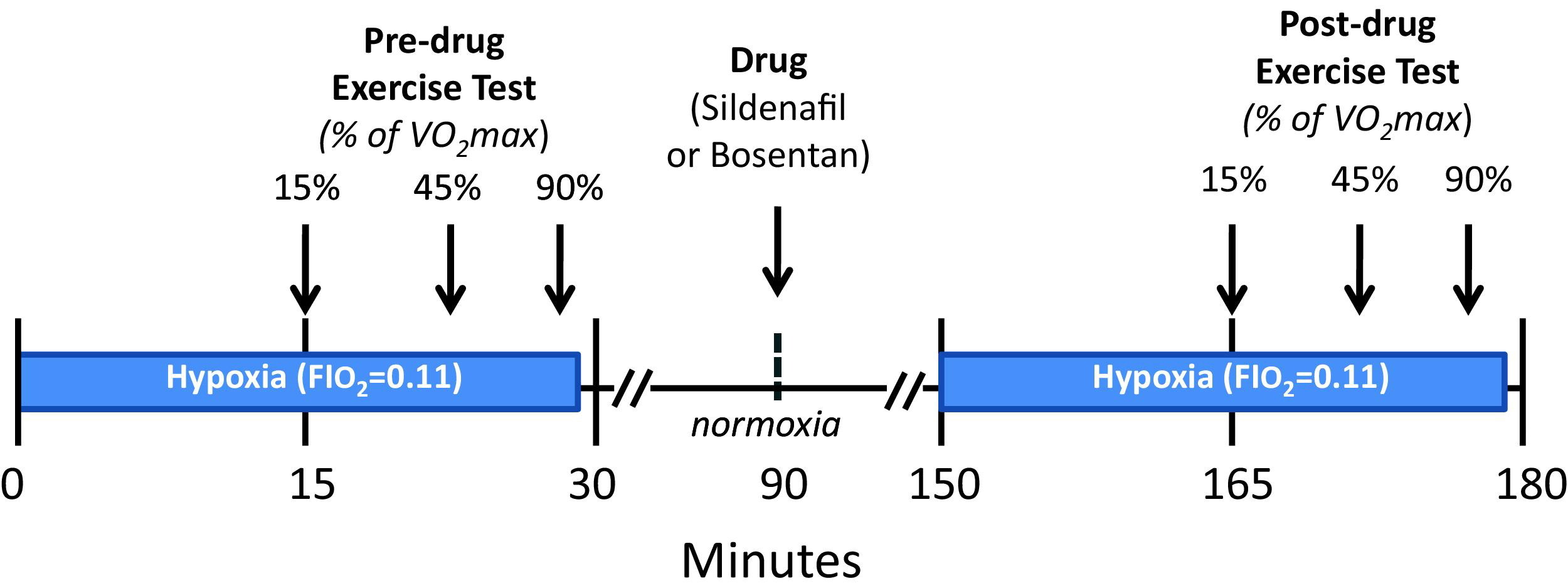
Timeline depicting the exercise protocol before and after drug treatment.
Arterial sampling and blood gas measurements
Arterial blood was sampled at rest and during exercise from a 20-gauge catheter (BD Arterial Cannula with FloSwitch, Becton-Dickinson, Swindon, UK) inserted in the radial artery. Two mL of arterial blood was drawn in a separate heparinized syringe and used for arterial blood gas assessment. Arterial blood gas samples were analyzed for partial pressure of O2 (PaO2) and CO2 (PaCO2), pH, hemoglobin (Hgb), O2 saturation (SaO2), electrolytes, and lactate, using a Bayer Rapidlab 865 blood gas analyzer/co-oximeter (Chiron Diagnostics Corp., Walpole, MA, USA). All blood gas values were corrected for temperature using tympanic temperatures measured during blood sampling.
Alveolar PO2 was calculated using the equation PAO2 = PIO2 – (PaCO2/RER)(1-FIO2 [1-RER]) and was used to calculate alveolar minus arterial O2 difference (A-aDO2).
Statistical analyses
Data presented are expressed as mean ± SE, unless otherwise noted. Statistical analysis was first performed using a 3 × 2 analysis of variance (ANOVA)—drug (sildenafil vs bosentan) before and after treatment (with vs without drug) and exercise intensity (StatView 5.0, SAS Institute, Inc, Cary, NC, USA). When a significant main effect for the drug was found, separate post-hoc analysis (Boneferroni-Dunn) was performed on sildenafil and bosentan groups. When a significant main effect for the drug treatment was found, repeated measures ANOVA was used for determination of significant differences before and after drug treatment. Anthropometric data between groups was compared using an unpaired t test analysis. In all cases, significance was determined by a P value < .05.
Results
Subject characteristics and pre-screening data
Subject demographics, pulmonary function data, and maximal oxygen uptake (V̇O2max) are shown in Table 2. There was no significant difference in age among the subjects based on grouping by gender or drug treatment. As expected, females had lower body mass, shorter stature, smaller lung volumes, and lower V̇O2max compared to male counterparts (Table 2). However, when subjects were grouped according to drug treatment, no significant differences in body mass, pulmonary function, and/or V̇O2max existed. Regardless of grouping, the data in Table 2 indicate that all subjects had normal pulmonary function and represent a very aerobically fit population.
Comparison of subject's pulmonary function and maximal aerobic capacity based on separate grouping for gender and drug treatment
Data are mean ± SD. FVC, forced vital capacity; FEV1, forced expiratory volume at 1 sec; VO2max, maximal O2 uptake.
p < .05 using unpaired Student's t-test.
Metabolic and blood gas data
As expected, V̇O2, V̇CO2, and V̇E during submaximal exercise were lower in women compared to men (Table 3), but no difference was seen in V̇O2, V̇CO2, and V̇E in response to either sildenafil or bosentan drug treatment (Table 4). The RER, at rest or during exercise, was unaffected by either gender or drug treatment (Tables 3 and 4).
Metabolic and blood gas data in hypoxia (FIO2=0.11) at rest and during exercise before and after drug (sildenafil or bosentan) treatment
Data are mean ± SE.
significantly different compared to males in same group, p < .05.
Metabolic and blood gas data in hypoxia (FIO2=0.11) at rest and during exercise before and after drug treatment
Data are mean ± SE.
Treatment with either sildenafil or bosentan increased PaO2 by 2 to 3 mm Hg and SaO2 by 3% to 4% (Table 4) with similar increases observed in both male and females (Table 3). Drug treatment, however, had no significant effect on either A-aDO2 and P50 (ie, PaO2 at 50% saturation, Table 4) except for a small increase in A-aDO2 seen in females (Table 3). However, PaCO2 was found to be lower (P < .001) with sildenafil, but not significantly different with bosentan.
Significant main effect for gender was observed with arterial PO2 and saturation (SaO2), indicating that females had higher PaO2 and SaO2 compared to men at any given exercise level (Table 3). However, no significant main effect in A-aDO2 and P50 was observed between the genders (Table 3). Likewise, arterial pH was not different based on gender or drug treatment grouping (Tables 3 and 4).
Cardiac data
Heart rate, at rest and during exercise, was not different between males and females (Table 3). However, following treatment with either sildenafil or bosentan, heart rate was greater compared to pre-drug measurements made at rest and during exercise in both males and females (Tables 3 and 4).
Systolic, diastolic, and mean arterial pressure were not different, at rest or during exercise, when comparing gender (data not shown). However, systolic pressure was 10% lower with sildenafil (P < .05), but not significantly different with bosentan (P = .32), despite a similar 9% decline at rest; and no difference in systolic pressure was observed with either sildenafil or bosentan during heavy exercise. Likewise, no differences in diastolic or mean arterial pressure were seen at rest or during heavy exercise with either drug (data not shown).
Discussion
The main finding of this study is that, in a controlled laboratory trial, sildenafil and bosentan significantly increased arterial oxygenation (ie, PaO2 and SaO2) at rest and during exercise during short-term exposure to acute hypoxia. We also examined whether taking either drug would be influenced by gender. In this regard, there was no systematic difference between the drug-treated men and women in hypoxia, at rest or during exercise. However, these data do show that women (with or without drug treatment) were less hypoxemic at rest and during exercise in hypoxia compared to their male counterparts.
Improved pulmonary gas exchange in hypoxia with sildenafil or bosentan treatment
In healthy individuals, pulmonary O2 transport is normally perfusion-limited and, thus, arterial oxygenation is largely dependent on blood flow through the lungs. However, under hypoxic conditions (especially during exercise), O2 can become diffusion-limited (impairing O2 transfer across the alveolar-capillary membrane), resulting in a widening A-aDO2. By definition, the diffusing capacity of O2 in the lung (DLO2) is determined by 3 components: 1) the alveolar-capillary membrane (DM); 2) the gas (O2) pressure differential (ΔP) across DM; and 3) the time it takes for O2 to react with hemoglobin (which is a function of O2 reaction time [θ] and the volume of capillary blood [Vc]). Thus, increasing pulmonary blood flow (by reducing PVR) would not be expected to benefit an O2 diffusion-limited lung. However, Snyder et al have shown an improved lung DM conductance when correcting for the changes in pulmonary Vc following sildenafil treatment. 29 These data suggest that, while reducing PVR may not alter pulmonary blood flow per se (ie, cardiac output), 15 sildenafil may increase pulmonary capillary volume and lessen the effects of the O2 diffusion-limitation under hypoxic conditions by decreasing capillary transit time within the pulmonary capillaries. 29
Other potential explanations of improved gas exchange that must be considered include: 1) improved ventilation/perfusion matching (V̇A/Q̇); 2) reduced shunting; and/or 3) hyperventilation. From these data, it cannot be directly addressed whether or not V̇A/Q̇ was improved or if a reduction in pulmonary shunting also occurred. But, we would note that, in mechanically ventilated pigs under normoxic conditions, V̇A/Q̇ was not significantly altered with sildenafil dosages at 25, 50, or 100 mg. 30 It is not known whether the same is true under hypoxic conditions in the face of HPV. To the extent that HPV is unevenly distributed in healthy human lungs, it is possible that converting low V̇A/Q̇ lung regions to normal—or more homogeneous—V̇A/Q̇ units could improve gas exchange and arterial oxygenation. Indeed, because impaired pulmonary gas exchange and widening A-aDO2 are thought to be linked with the development of pulmonary hypertension (leading to pulmonary interstitial fluid accumulation) and V̇A/Q̇ mismatching with exercise at high altitude,1,3 it is not surprising that reducing pulmonary vascular resistance might increase PaO2 under hypoxic conditions. Supporting this is the observation that HAPE-susceptible subjects develop greater exercise-induced V̇A/Q̇ inequality compared to control subjects, 4 and that an increase in PAP is thought to be one of the principal mechanisms resulting in HAPE. 5 -7 We cannot exclude the possibility that either alveolar and/or interstitial fluid accumulation (ie, increased leaking of water from the capillaries because of greater capillary permeability, whether as a result of increased PAP or independent of PAP) could itself contribute to diffusion impairment of O2 that is often seen in hypoxic conditions. Nonetheless, the present finding that drugs which reduce PVR result in improved PaO2 during hypoxic exercise is consistent with the notion that HPV and pulmonary hypertension are significant contributors to pulmonary gas exchange impairment, and it also suggests that V̇A/Q̇ was likely altered in order to improve gas exchange following sildenafil or bosentan treatment. Supporting this, a recent study showed that treating patients with COPD-associated pulmonary hypertension with sildenafil worsens V̇A/Q̇ matching. 31 Worsening gas exchange (ie, V̇A/Q̇) could be expected in COPD patients since global vasodilation of the pulmonary vascular bed would work against the beneficial action of HPV. Indeed, in the case of COPD, HPV is needed to redistribute pulmonary blood flow away from damaged (poor gas-exchanging) lung regions and preferentially send blood to areas of the lung with better gas exchange. In contrast, for healthy individuals exposed to environmental hypoxia, it would be postulated that drugs like sildenafil and bosentan would reduce (or prevent) hypoxia-induced pulmonary vasoconstriction and, therefore, mitigate (or prevent) the development of pulmonary hypertension sequelae.
In contrast to V̇A/Q̇, it appears unlikely that hyperventilation played a significant role in improving PaO2. Although a statistically significant decrease in PaCO2 was observed with sildenafil treatment, this did not translate to a significant elevation in ventilation (Table 4). Moreover, a significant decrease in PaCO2 was not seen with bosentan treatment, which demonstrated similar increases in PaO2 as that seen with sildenafil (Table 4). Thus, it is seems unlikely that hyperventilation can explain the greater PaO2 occurring with sildenafil or bosentan treatment.
It is worth noting that there was a leftward shift in the O2 dissociation curve, as evident by the decline in P50 with sildenafil and a similar decline (albeit nonsignificant) with bosentan treatment (Table 4). Given the hypoxic conditions used in this study (FIO 2 =0.11), it is evident that PaO2 will be positioned on the steep linear portion of the O2 dissociation curve. It is tempting to speculate that, had the P50 not declined, it is possible that a greater post-drug increase in PaO2 and SaO2 might have occurred. Nevertheless, with the degree of hypoxemia present, even the relatively small (2-3 Torr) increase in PaO2 we observed could be expected to aid and improve O2 availability to exercising muscles and, consequently, might improve exercise tolerance and/or performance at altitude. 18 ,20,24
Cardiac function
One of the benefits of reducing PVR during exercise in hypoxia may be a reduction in right ventricular afterload—aiding left ventricular diastolic filling—which could improve cardiac performance as well as exercise tolerance at high altitude. While improvements in cardiac function have been reported in patients' taking sildenafil for primary or secondary pulmonary hypertension, the majority of studies using sildenafil in healthy subjects show little, if any, change in cardiac output. 9 ,32,33 Moreover, cardiac output/cardiac function is not different during acute hypoxic exercise in healthy subjects treated with a single dose of bosentan (up to 250 mg), 15 thus there seems little chance that reducing RV afterload could improve exercise in normal healthy subjects. 19 Taken together, these data are consistent with the fact the intrinsic cardiac function is not a limiting factor for cardiac performance during exercise at high altitude and, therefore, improvements in cardiac function contribute very little, if at all, to improved exercise performance in healthy subjects at high altitude.
We were surprised to see that the resting heart rate was significantly elevated in both the sildenafil and bosentan groups (Table 4), especially since most studies at high altitude have not reported the same response. 22 ,23,34 But, in fact, ours is not the only study to find an increase in resting heart rate with sildenafil. Ricart et al also report a significant increase in resting heart rate with sildenafil under both normoxia and hypoxia conditions. 35 But, in contrast to our study, they report no difference in heart rate during hypoxic exercise. 35 It is interesting to note, however, that Hsu et al have reported healthy individuals as sildenafil “responders” and “nonresponders.” 24 In their study, “sildenafil-responders” showed improved cardiac output and exercise performance in hypoxia, whereas “nonresponders” did not. 24 These data suggest that treating healthy individuals with sildenafil (or similar drugs, such as bosentan) is not likely to be beneficial to everyone, but an explanation for this differential response remains to be determined.
Although we did not measure cardiac output and/or pulmonary artery pressure (PAP) in this study, the effects of sildenafil and bosentan on cardiac output, PVR and PAP have already been well-studied and documented. For example, Ghofrani et al report a 19% decrease in PAP at rest and an 18% decrease in PAP during exercise in healthy mountaineers in a field laboratory located at Mount Everest base camp (5245 m) who were taking the same oral dose of sildenafil (50 mg) we used in this study. 22 Richalet et al also show sildenafil-induced decreases in PAP (approximately 21–35% between 2 and 5 days), and report similar improvements in PaO2 with sildenafil after 2 and 5 days at high altitude (4350 m). 23 Likewise, Modesti et al report a 32% decrease in PAP one day after a single dose of bosentan (62.5 mg) at 4559 m. 21 Thus, there is ample evidence establishing the pulmonary vasodilating effect of these drugs in healthy subjects, and little reason to expect that PAP would not have been similarly reduced in response to sildenafil or bosentan treatment in our subjects.
Gender difference in gas exchange
Gender differences in pulmonary structure and function have been well-described. 25 -28,36-39 As expected, women had smaller lung volumes (Table 2) and lower minute ventilation, V̇O2, and V̇CO2 during exercise compared to men (Table 3). Despite this, we found that women consistently had greater PaO2 and SaO2, at rest and during exercise—both before and after drug treatment—compared to men (Table 3). It is worth noting, however, that A-aDO2 was not significantly different between men and women, indicating that overall gas exchange was equally impacted by hypoxia in both men and women (Table 3). Contrary to recent studies that suggest that women (by virtue of smaller airways, reduced lung size, and/or lower ventilatory response to exercise 26 ,27,40-42) may be more prone to gas exchange impairment during exercise than men; these data show that young athletic women have at least the same, if not better gas exchange (eg, higher PaO2 and SaO2) during hypoxic exercise compared to men. While present findings are consistent with another observation that pulmonary gas exchange during exercise is not worse in women when matched to men according to age-, height- and aerobic capacity, 25 we would caution against widespread generalization of our results due to the limited number of subjects in our study. Indeed, the principal purpose of this study was to examine gas exchange during hypoxic exercise before and after treatment with sildenafil or bosentan. Using the repeated measures study design, with each subject serving as their own control, provided much greater statistical power (in determining drug effect) than that which can be obtained from a cross-sectional study design (ie, as with ours gender comparison). Further studies with a much greater number of subjects will be needed to make a more compelling cross-sectional comparison in gas exchange between men and women. Nevertheless, it is evident from our data that there was no significant difference in the gas exchange response (between men and women) to the respective drug treatments.
Perspective
There is great concern over ergogenic drugs in many professional and competitive sports arenas. On the other hand, to many amateur athletes and/or active individuals (such as recreational skiers, mountain climbers, outdoor enthusiasts, etc.) these drugs are seen as beneficial because they can minimize and/or alleviate altitude-related problems and improve tolerance of physical activity at high altitude. While the present data suggest that pulmonary vasodilators can improve PaO2, the question relating to whether sildenafil or bosentan may be used (or abused) by healthy individuals in order to achieve better high altitude performance remains uncertain. This is evidenced by the conflicting reports with respect to the benefit of sildenafil on exercise performance at high altitude (Table 1). One explanation for variability between these studies may be related to the degree of HPV and/or the level of hypoxemia occurring among individuals. Thus the benefit from any pulmonary vasodilating drug may depend on the degree of pulmonary hypertension induced by hypoxia (or exercise), so that subjects with a greater degree of hypoxia-induced hypertension are likely to achieve the greatest benefit compared to those with a lesser or minimal increase in PAP. This would imply that any benefit from pulmonary vasodilators on pulmonary gas exchange may only be realized in the presence of pulmonary arterial hypertension, which could—at least in part—explain the varied responses to exercise performance currently reported in the literature (Table 1) and why some individuals respond to treatment and others do not. While there is evidence that sildenafil treatment can improve physical performance in some healthy individuals under hypoxic conditions, the notion that similar benefits might occur in healthy subjects taking sildenafil under normoxic (ie, sea level) conditions is not supported. 24
Conclusion
These data show that sildenafil and bosentan, both of which are clinically used to reduce PAP in patient populations with pulmonary hypertension, are capable of improving pulmonary gas exchange in young healthy (male and female) subjects exercising in hypoxia. It is be tempting to speculate that the improvements in oxygenation we observed in our healthy subjects might translate to improved physical performance at high altitude. However, it must be emphasized that our study was not designed to address this question, and evidence of improved exercise capacity in healthy individuals taking sildenafil or bosentan is limited and remains equivocal at best. Nonetheless, these data suggest that sildenafil and bosentan can improve PaO2 during hypoxic exercise. Even though the improvement was small (2–3 mmHg), it is likely to be physiologically important given the degree of hypoxemia and the energy demands encountered during hypoxic exercise.