
Abstract
Direct ocular inoculation with African spitting cobra (Naja nigricollis) venom in the United States is uncommon, especially in an urban setting, but can lead to serious acute and chronic ocular injury depending on the extent of exposure. We report 2 cases of indirect ocular inoculation with venom from an African spitting cobra, manifesting as periocular soft tissue swelling, extensive conjunctivitis, and corneal epithelial erosion. Both of the reported cases involve young male patients who received prompt emergency evaluation and treatment including copious irrigation of the ocular surface, followed by close monitoring by an ophthalmologist resulting in excellent outcomes with minimal visually significant ocular sequelae.
Introduction
Direct inoculation of the ocular surface with snake venom is a rare occurrence in the United States. Such an accidental encounter would be most plausible to occur in a wilderness setting (outside the United States), though lifestyles and/or careers that promote close proximity to venomous snakes (eg, zookeepers) can provide a route for such an encounter in an urban environment. Direct ocular envenomation, particularly from various species of spitting cobras, can cause chemical injury with an array of purported findings ranging from mild conjunctival and corneal inflammation to frank corneal ulceration and perforation with eventual blindness. 1 The majority of cases in the literature documenting ocular effects of direct spitting-cobra envenomation arise from remote locations (eg, Africa). In this report, we document 2 cases of ocular exposure to African black-necked spitting cobra (Naja nigricollis) venom. These cases involve patients who presented to an urban, tertiary care medical treatment center for initial evaluation and subsequent care. Study approval was granted by the institutional review board at The University of California, Los Angeles (UCLA IRB no. G09-02-067-01).
Report of Two Cases
Patient 1
A 30-year-old man presented to the UCLA emergency department 2 hours after exposure to venom from an African spitting cobra (Naja nigricollis). The patient was a snake handler, and his exposure occurred after touching his hand to a hook used to milk venom and subsequently rubbing the skin directly underneath his left lower eyelid with the contaminated hand. He denied getting any venom directly into his eye but noted immediate burning pain in and around his left eye after the hand rubbing. He initially flushed the eye with tap water but after continued worsening of symptoms presented to the emergency department. Upon initial evaluation, visual acuity was 20/20 in the right eye and 20/200 improving with pinhole to 20/50 in the left eye; pupillary examination and tonometry were within normal limits. Slit-lamp examination revealed trace upper eyelid edema and trace conjunctival injection of the right eye. The left eye showed marked upper, greater than lower, eyelid edema and erythema, diffuse conjunctival injection (Figure 1A), and a large epithelial defect of the corneal surface measuring 5.5 mm horizontally by 6 mm vertically (Figure 1B). There was no limbal ischemia, and pH measured 7.4 in both eyes. Dilated funduscopic examination of both eyes was within normal limits. Using a Morgan lens (MorTan Inc., Missoula, MT), the left ocular surface was irrigated copiously with 2 L normal saline over 1 hour, and the patient was subsequently discharged on a topical antibiotic drop (ciprofloxacin hydrochloride 4 times daily) and a cycloplegic drop (cyclopentolate 3 times daily) for the left eye, which were continued for 1 week. The patient's left eye was pressure patched for the first day after the injury, and he was followed closely by the ophthalmology service, initially daily, until the epithelial defect was completely healed, and subsequently at longer intervals. The epithelial defect and eyelid swelling of the left eye healed completely by day 5 after injury, and the conjunctival injection resolved by 2 weeks after injury. Topical steroid therapy (prednisolone acetate 1% 4 times daily) was initiated on day 4 after injury and continued for 1 week in the left eye. Visual acuity of the left eye improved to 20/30 at 1 month after injury. Slit-lamp examination revealed a central area of corneal epithelial irregularity, a repeat dilated exam remained within normal limits, and refraction did not provide any additional improvement in visual acuity.
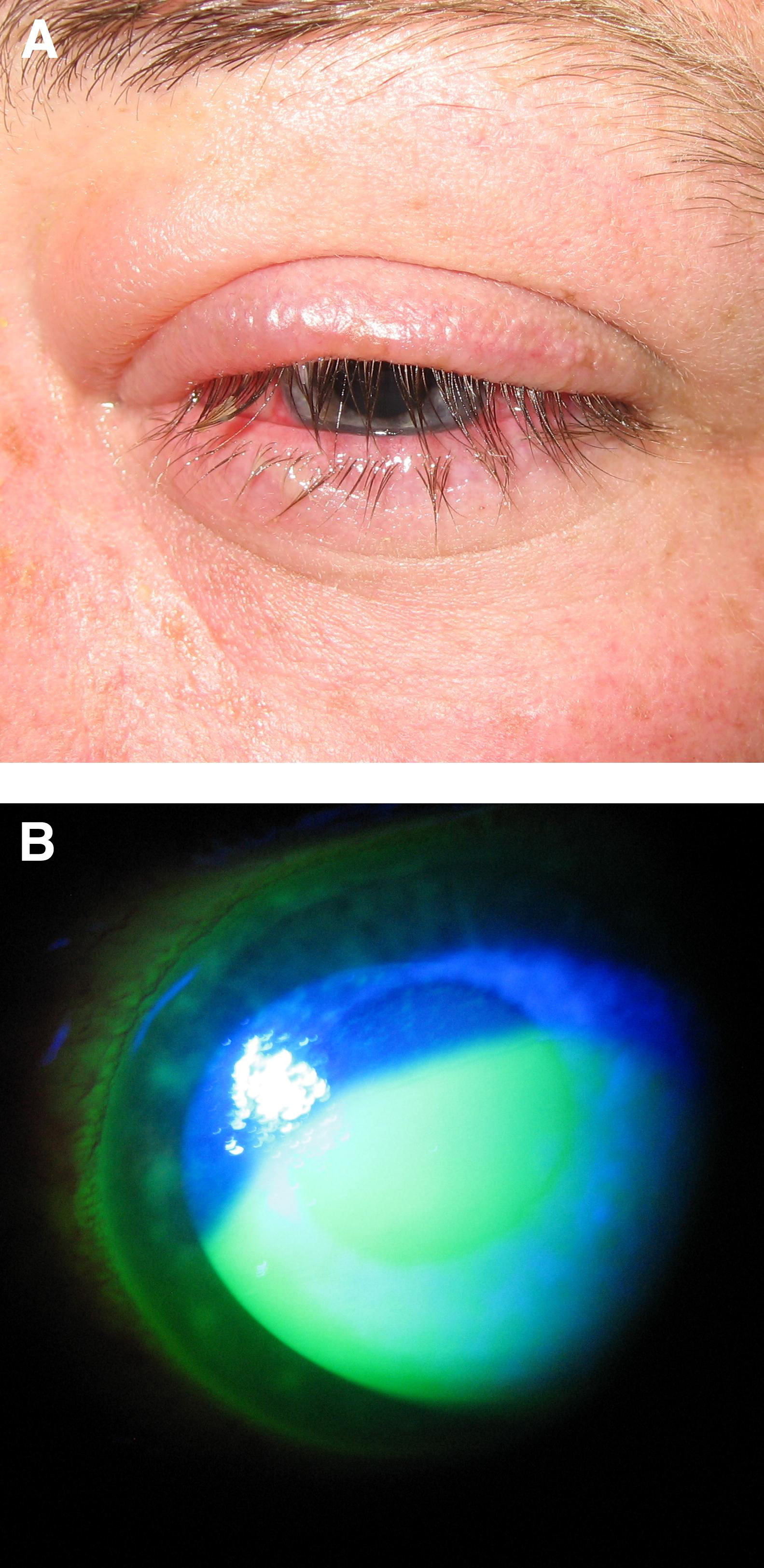
Slit-lamp biomicroscope photograph of the left eye of patient 1 on day of injury. (A) Marked upper, greater than lower, eyelid edema with erythema and diffuse conjunctival injection. (B) Fluorescein instillation reveals a large epithelial defect of the cornea.
Patient 2
A 22-year-old man presented to the UCLA ophthalmology urgent walk-in clinic 2 days after injury to his left eye involving exposure to spitting cobra venom. He was wearing protective goggles while handling an African spitting cobra (Naja nigricollis). Venom was spit by the snake, contacting the malar area below his left eye but with no direct ocular exposure. He removed the goggles to “get air” and noted immediate pain involving his left eye. He presented shortly after injury to an outside hospital emergency department, where his left eye was copiously irrigated with 3 L of fluid. He was told that he had an abrasion covering the entire surface of his left cornea and was started on antibiotic (ciprofloxacin hydrochloride) and cycloplegic (cyclopentolate) drops. On initial evaluation by our facility (day 2 after injury), visual acuity was 20/20 in the right eye and 20/30 in the left eye. Slit-lamp examination was remarkable for a large epithelial defect of the left cornea measuring 4.1 mm horizontally by 3.2 mm vertically, moderate diffuse conjunctival injection of the left eye, and a mild pseudomembrane, which was removed. The epithelial defect healed completely by day 4 after injury, at which time topical steroid drops (prednisolone acetate 1% 4 times daily) were initiated and continued for 1 week. By 2 weeks after injury, visual acuity returned to 20/20 in both eyes, and slit-lamp examination of both eyes was within normal limits.
Discussion
Direct human ocular exposure to spitting cobra venom has been previously documented in the literature, with varying degrees of ensuing ocular injury. 1 –4 Here, we report 2 cases of significant acute ocular toxicity related to indirect ocular exposure to spitting cobra venom, with 1 patient enduring a mild long-term decrease in visual acuity of the affected eye. Ocular injury secondary to indirect exposure to snake venom has not previously been documented in the literature. We illustrate the acute ocular findings, emergency treatment, and subsequent clinical course of this type of patient, which may be encountered in the urban clinical setting.
Snake venom contains a variety of bioactive proteins including neurotoxins and proteolytic enzymes, which can have significant local destructive effects. 5 This local toxicity is likely independent of pH given the neutral pH measured prior to irrigation of the ocular surface in patient 1. The effect of indirect exposure to snake venom on the ocular surface appears to manifest as periocular soft tissue swelling, extensive conjunctivitis, and corneal epithelial erosion. It is plausible that the ocular injuries could have progressed to involve deeper ocular structures with more visually significant damage had the patients not received prompt evaluation and treatment in the emergency department setting. Topical antibiotic prophylaxis in the setting of a large epithelial defect such as that seen in these patients is prudent to reduce the chance of a secondary corneal infection. Topical steroid use after epithelial surface healing in these patients is directed to potentially prevent symblepharon or other late inflammatory sequelae, which did not develop in our patients, though the efficacy of such treatment could be considered controversial. It has been suggested in various animal studies that heparin and topical antivenom could reduce the severity of chemical injury related to spitting cobra venom, mechanistically theorized to work via calcium chelation, which could limit toxin-stimulated release of degradative corneal collagenases that are calcium dependent, and direct binding of the active toxin, respectively. 6 Applicability of this information to human subjects should be considered with apprehension, and further investigation is warranted.
Given the occupational and potentially preventable nature of the injuries sustained from indirect facial exposure to snake venom in the setting of protective goggle wear, we would recommend more rigorous personal protective equipment to all snake handlers that would cover the entire face when handling venomous snakes. Additionally, hand washing with soap and water after handling snake venom is recommended to reduce the likelihood of subsequent indirect venom exposure. As with any chemical injury to the eye, initial treatment should be focused on copious and prompt irrigation to dilute and remove any toxin. Prompt consultation with and close monitoring by an ophthalmologist after this type of injury should be obtained to optimize patient outcome.
Footnotes
Acknowledgments
The authors would like to thank Gina Yoo, MD, for her assistance with management of the patients presented in this report.