
Abstract
Septic arthritis is a surgical emergency that can result in substantial morbidity and mortality, especially when diagnosis is delayed. We report a case of an otherwise healthy 12-year old boy, who developed an orbital subperiosteal abscess and paranasal sinusitis with concomitant septic arthritis of the left hip and osteomyelitis. We highlight the importance of repeat assessment of affected sites of infection, despite an overt, local infection of a primary site in an immunocompetent host. This is the first report of concurrent orbital subperiosteal abscess and left hip septic arthritis in literature.
Introduction
Septic arthritis is the presence of intraarticular seeding with living microorganisms. It is an uncommon but potentially fatal emergency that can lead to poor functional outcomes of the involved joints. It occurs predominantly as monoarticular septic arthritis, with the hip and knee being the most commonly involved joints, followed by the shoulder and ankle, with the hip appearing more frequently in children. 1,2
The presence of septic arthritis in a young immunocompetent patient is a rare phenomenon. Risk factors include leukaemia, diabetes mellitus, corticosteroid therapy, cytotoxic chemotherapy, rheumatoid arthritis, intravenous drug, trauma and intraarticular injections. 1,2 Although sinusitis from Haemophilus influenzae has been associated with septic arthritis, 3 Borenstein and colleagues mentioned the knee was affected in two cases, and one of the two cases had predisposing factors of rheumatoid arthritis. The two cases of septic hip caused by H. influenzae had no upper respiratory tract infection. There were predisposing factors of trauma in one case and systemic lupus erythematosis in another. We therefore report a rare case of a young boy with good past health who presented with concurrent orbital subperiosteal abscess, sinusitis, septic arthritis of the hip and osteomyelitis.
Case Report
The patient and parents were clearly informed that data concerning this case would be submitted for publication, and they agreed. A 12-year-old boy presented to an accident and emergency department with a 1-week history of fever and left eye and left hip pain. His symptoms progressed, despite being on amoxicillin and clavulanate prescribed by a general practitioner. There was no history of trauma, and he had no significant medical history. On physical examination, he was noted to have a fever of 38.3°C with marked left eye proptosis, multidirectional ophthalmoplegia and left facial swelling. Visual acuity was similar to his baseline at 20/50 oculi uterque (OU). Local tenderness over the lateral hip at the gluteus medius region was noted, with no swelling or erythema. His hip flexion was up to 90°, and the internal and external rotation was limited to 20°. There were no other joints involved.
Investigations revealed a raised white cell count of 15.5 × 109/L with a neutrophil predominance at 83%. Erythrocyte sedimentation rate and C-reactive protein were markedly elevated at 118 mm/h and 128.4 mg/L, respectively. A small amount of effusion and mild synovitis were detected on ultrasound scan of the left hip, with the joint space thickening and fluid measuring 3–4 mm in thickness. An aspiration was performed under ultrasound guidance with a small amount of blood-stained fluid aspirated. The cell count of the hip aspirate revealed to be 45,672 cells/mm3 with neutrophil making up to 65%.
Computed tomography of orbits and brain with contrast was performed which revealed a large left medial orbit subperiosteal abscess and marked left paranasal sinusitis of the ethmoid and maxillary sinuses (Figure 1). In view of these findings, an emergency functional endoscopic sinus surgery with open drainage using a Lynch incision was performed. After the surgery, there was resolution of the left eye proptosis and ophthalmoplegia.
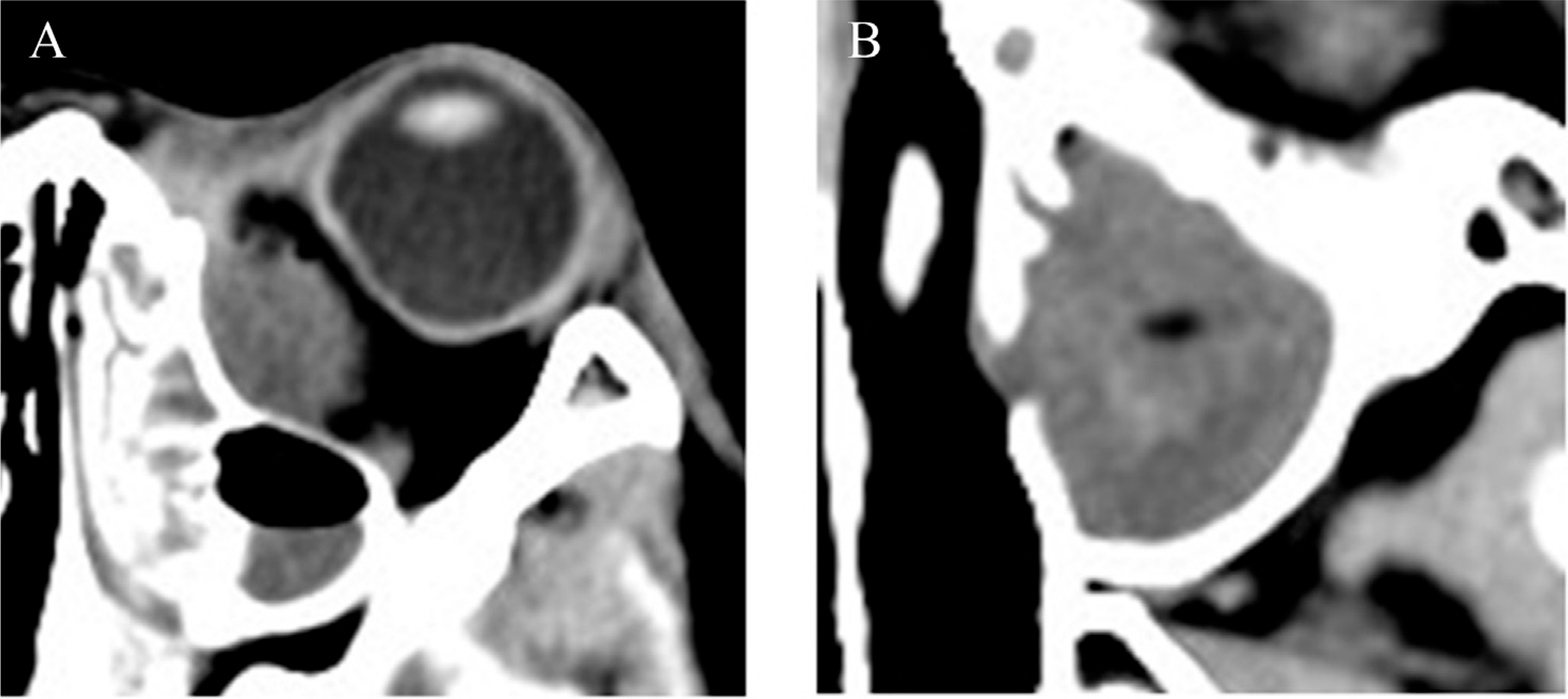
(A) Magnified views of the left orbital abscess, measuring 32 mm long × 14 mm wide x 21 mm tall, causing proptosis. An air–fluid level is also seen within the left ethmoid sinus; (B) near-complete fluid filling and mucus retention of the left maxillary sinus with gas locules seen. The presence of the above findings, combined with the lack of a sclerotic, thickened sinus wall, points towards an acute sinus infection.
He was empirically covered with cefotaxime, cloxacillin and metronidazole. Later, culture of the left maxillary sinus and nasal swab grew Streptococcus pneumoniae. Hence, the antibiotic regime was switched to penicillin G in accordance with the sensitivity results.
However, the fever and left hip pain persisted, despite these procedures and antibiotics. We then performed a contrast magnetic resonance imaging (MRI) of the left hip which showed a left hip joint effusion, synovial thickening and marrow oedema with increased enhancement in left acetabulum, compatible with acute osteomyelitis (Figure 2). Consequently, arthrotomy for drainage and lavage was performed to treat the septic arthritis. Before drainage, a needle connected to a syringe was first passed to check the pressure, and 10 mL of purulent joint fluid filled itself on puncturing the joint, indicating the increased intraarticular pressure. The cell count of the hip aspirate was elevated to 141,384 cells/mm3 with neutrophil making up to 87%.
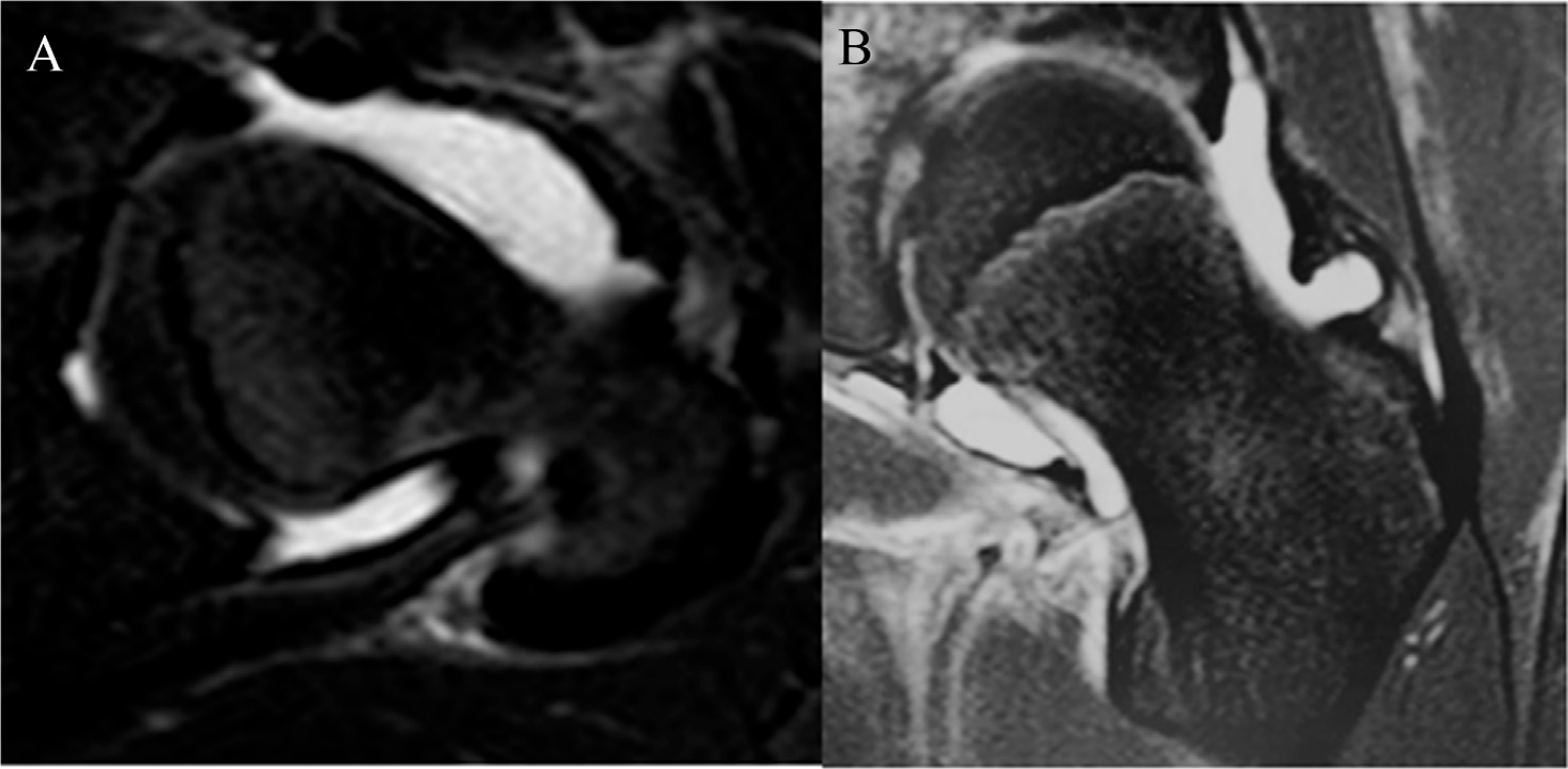
(A) Transverse plane of T2-weighted MRI magnified views of a hyperintense collection enveloping the left neck of femur. (B) Coronal plane. MRI = magnetic resonance imaging.
Although the purulent-looking left hip joint fluid and blood culture did not grow any microorganisms, after open drainage, his fever and left hip pain resolved rapidly with a downtrend of haematological levels of inflammatory markers. On discharge, he was given 4 more weeks of oral penicillin V to complete the course.
Four months after the operation, an MRI showed resolving septic arthritis and no features of chronic osteomyelitis. At a follow-up evaluation 5 months after the initial onset, there was a complete resolution of symptoms with a full range of hip motion regained.
Discussion
Septic arthritis in an immunocompetent patient is uncommon. Although this occurrence is rare, several case reports and case series in which septic arthritis has developed in previously healthy individuals have been documented. 4 –6 Risk factors predisposing to this condition include diabetes mellitus, rheumatoid arthritis, renal disease, malignancies, intravenous drug and cytotoxic chemotherapy. 1,2 The rarity of our case is further highlighted when such a severe infection involving haematogenous spread is seen in a previously healthy child, with no known risk factors.
It is not infrequent for joint aspirate to yield negative bacteria cultures from various locations, in the presence of overt clinical signs of an infected joint. A positive joint fluid culture was reported in only 55% of patients, and bacteria were isolated in any one of blood, joint fluid pus or bone culture in 70% of patients. 2 Owing to the significant figure of patients who will return with no bacterial culture growth, it is pertinent to monitor patients clinically and investigate further with an MRI in this case which confirms the progression of the condition.
Even with treatment started, an 11% mortality rate has been reported for monoarticular involvement, with a significant increase in the figure to 50% in polyarticular cases. 7 A delay in drainage of hip joint abscess raises the likelihood of permanent damage because increased intraarticular pressure can compromise blood supply, resulting in avascular necrosis of the femoral head. Muscle spasms may also occur, predisposing to hip dislocation. 8 Hence, a low threshold for imaging of suspected joint infections and subsequent drainage of such joints is advocated to reduce disability. Distant sites of infection can be inconspicuous and, if ignored, will lead to disabling sequelae. We advocate vigilance, especially of hip and shoulder joints, which are hidden inside muscular planes. Prompt diagnosis with the use of an MRI and early operative treatment is necessary to reduce disability and other serious outcomes. In this case, the appropriate treatment with antibiotics did not prevent progression of septic arthritis which settled after surgical drainage.
A common aetiology is haematogenous dissemination in a bacteraemic episode, and it is frequently associated with acute haematogenous osteomyelitis. 1,2 This was likely in our case with orbital subperiosteal abscess and paranasal sinusitis as the primary source of infection complicated by septic arthritis of the hip. This is further supported as S. pneumoniae, a typical bacteria causing sinusitis, is the causative agent of our case. 4 In addition, a study by de Greef in 2016 found that induced pneumococcus bacteraemia could lead to septic arthritis in a porcine model. 9 H. influenza septic arthritis had also been associated with sinusitis in 7% of patients in a review of 29 cases. 3 In the extensive review by Borenstein on H. influenza–induced septic arthritis, two cases were septic arthritis of the hip. One had no extraarticular involvement, and there was predisposing factor of trauma. In another case, the extraarticular condition was cellulitis, and this patient had predisposing factor of systemic lupus erythema. The three H. influenza septic arthritis associated with sinusitis all affected the knees and elbow, two of those patients had predisposing factor of rheumatoid arthritis, splenectomy and alcoholism. We therefore had not found reports of sinusitis associated with septic arthritis of the hip in a normal patient.
In pneumococcus septic arthritis, a review of 190 cases revealed none of which had concurrent sinusitis or orbital subperiosteal abscess. In five cases (7%) with extraarticular infection in children, they were either meningitis or pneumonia. 10
In conclusion, uncommon associated sites of infections exist. We highlight the significance of screening for distant sites of infection, despite the presence of a frank infection in an otherwise healthy adolescent. Repeated clinical assessment and timely use of the MRI are essential to confirm diagnosis. Early surgical drainage is still an important part of the management of septic arthritis in addition to antibiotics treatment.
Footnotes
Conflicts of interest
All authors do not have any conflicts of interest to declare.
Funding/support statement
None declared.