
Abstract
Vascular complications from orthopaedic surgery can be devastating. Arteriovenous fistula (AVF) and pseudoaneurysm formation are possible from orthopaedic injuries as well as orthopaedic surgery. Limbthreatening complications of vascular malformation include ischaemia, ulceration, haemorrhage, and gangrene potentially requiring amputation. Although rare, these vascular malformations should remain on the differential diagnosis for any patient not following the typical postoperative course. When presented with these case, and repair is recommended, it should be coordinated between orthopaedic and vascular surgeons. Review of the literature indicates that the risk of AVF and pseudoaneurysm formation remains underappreciated, particularly in the subacute and chronic setting. Theoretically, minimally invasive procedures with drilling near vessels increases the chances of vascular injury that goes unnoticed during the index procedure. This report of two cases discusses diagnosis and repair of pseudoaneurysm and AVF. It is a cautionary warning to consider these vascular injuries as late-presenting, limbthreatening complications of orthopaedic surgery.
Introduction
Vascular complications from orthopaedic surgery have some of the most devastating shortand long-term consequences and are potentially limb threatening. Acute vascular injuries are often recognised immediately and repaired appropriately; however, delayed vascular complications can be more difficult to diagnose. Two common types of vascular malformation are arteriovenous fistulas (AVFs) and pseudoaneurysms.
Pseudoaneurysms form when blood leaks through a breach in the vessel wall but is contained by the adventitia or surrounding perivascular soft tissue. Pseudoaneurysms differ from true aneurysms in that they do not contain all the layers of an artery. 1 A pseudoaneurysm evolves into a haematoma if blood passes through the adventitia and collects in the surrounding tissue external to the three vessel layers. Damage occurs due to partial division and erosion of the pulsating arterial wall, often by the projection of metallic screws or hardware. This can be from acute trauma as well as a myriad of orthopaedic procedures. 2,3 Persistent blood supply via the afferent artery can lead to aneurysm growth with potential rupture of the lesion resulting in massive blood loss. 4 Signs of pseudoaneurysm include continuous filling of a wound drain (if ruptured), hard and painful swelling of the lower leg or a pulsatile mass in the region of the affected joint. 5 Definitive confirmation of the diagnosis can be achieved by sonography and angiography. Traditional treatment includes stenting, surgical ligation with or without bypass or endovascular embolisation of the supplying vessel with evacuation of the surrounding haematoma.
An AVF forms due to concurrent lacerations of an adjacent vein and artery. 6 Symptoms of AVF include oedema, venous hypertension and varicosity, increased skin temperature as well as skin pigment changes. 7 Auscultation at the site of AVF formation commonly reveals a continuous bruit. A pulsatile mass, as well as digital ischaemia, with distal development of gangrene is also indicative of an AVF. 6 Duplex Doppler and computed tomography angiography have been recommended as diagnostic tools to aid in detecting AVF. 5,6 Traditional treatment is excision and ligation.
Vascular malformations including AVF and pseudoaneurysm are underappreciated complications of orthopaedic surgery and can have delayed presentation and unique pathology. Both can occur during routine orthopaedic surgery due to vessel trauma, which may not be immediately recognised. The two cases outlined in the following describe the presentation, diagnosis and surgical management of these two rare but potentially dangerous complications, including an AVF associated with tibial screw placement which presented 10 years after the initial anterior cruciate ligament (ACL) reconstruction. Finally, we review the literature to detail the examination findings that warrant further investigation.
Case Reports
Case 1
A 64-year-old male with no past vascular history presented 2 months status after the placement of a short cephalomedullary nail for a right-side intertrochanteric femoral fracture. He was initially discharged on postoperative day 3. He was readmitted approximately 1 week later with thigh swelling and diagnosed with a deep vein thrombosis. He was started on anticoagulation at that time. Sometime during the ensuing weeks, he was readmitted for thigh swelling, and advanced imaging was obtained. He did require a packed red blood cell transfusion for anaemia. At that time, the patient was diagnosed with a thigh haematoma, and his anticoagulation was stopped. He was discharged with the recommendation to wear compression stockings. He presented for a second opinion approximately 2 months after the index procedure.
Physical examination revealed a cool and firm operative thigh with an increased circumference to approximately three times the size of the left side. The remainder of the lower extremity was grossly oedematous. He had no palpable posterior tibialis or dorsalis pedis pulses, but both were biphasic by Doppler. A computed tomography angiography with contrast identified a pseudoaneurysm (3.1 cm × 2.8 cm) (Figure 1) arising from the distal right profunda femoral artery, which measured 4 cm in craniocaudal dimension. Adjacent to this was a large medial anterior thigh haematoma (15 × 21 × 31 cm), resulting in mass effect on the superficial femoral artery. In addition, the patient required a wheelchair because of a persistent external rotation deformity at the fracture site. An outside-hospital computed tomography performed 1 month postoperatively showed delayed union, malreduction and rotation of the fracture.
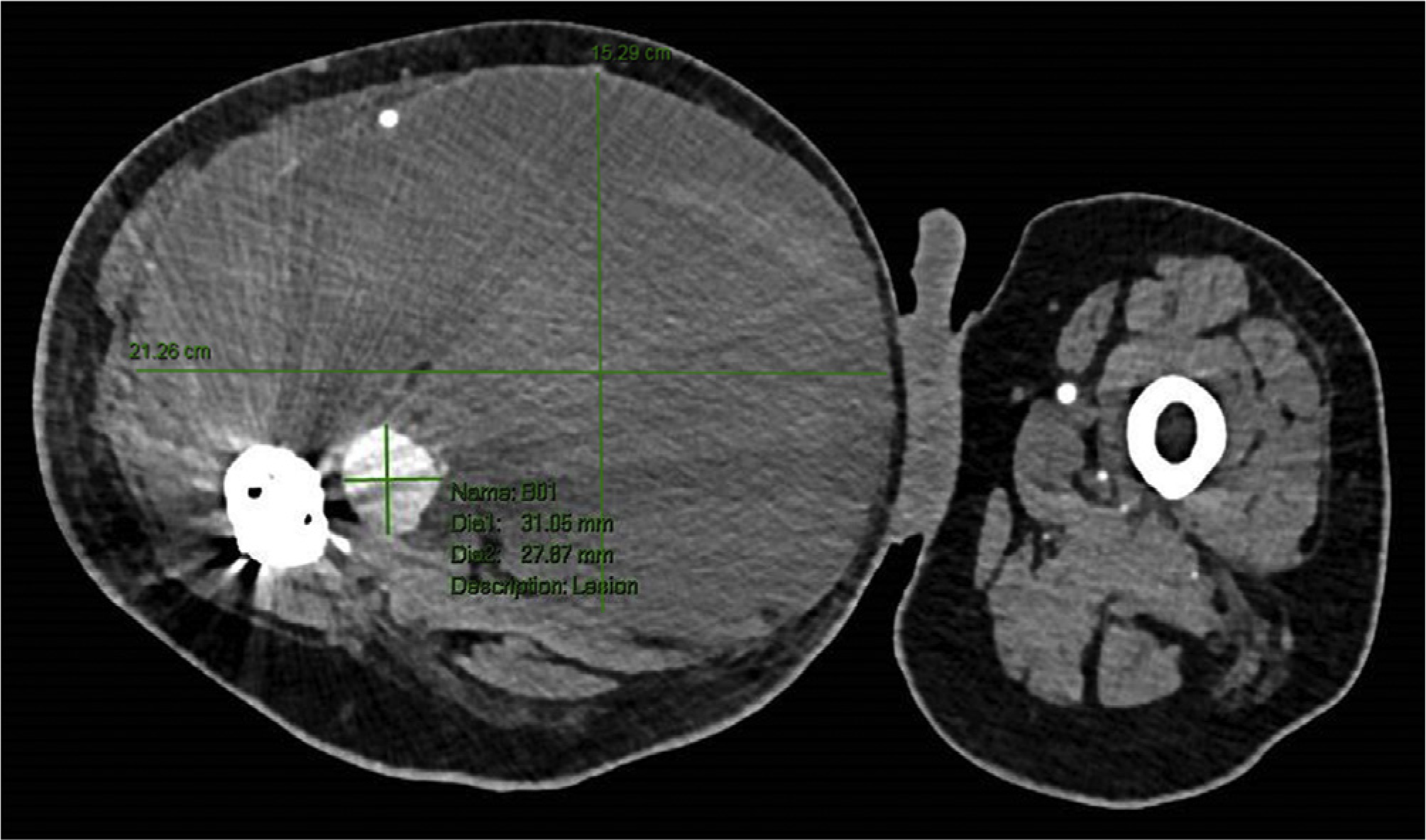
Axial lower extremity CTA showing Case 1 pseudoaneurysm with adjacent haematoma. The screw measured approximately 10 mm beyond the cortex on CT scan 2 months after the index procedure.
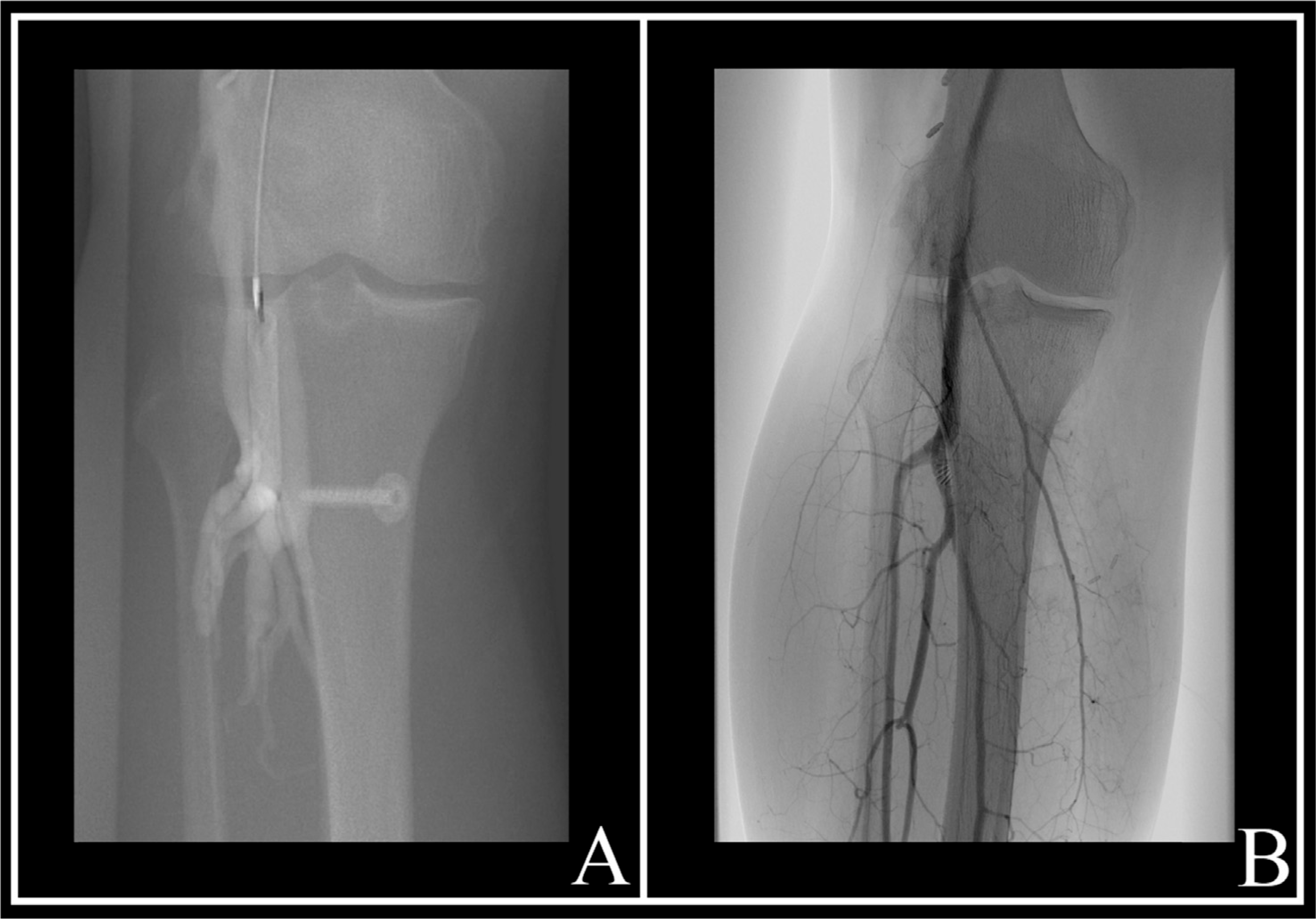
He underwent a staged procedure with interventional radiology coil-embolizing the pseudoaneurysm arising from the muscular branch of the right profunda femoral artery. Two days later, vascular surgery performed a haematoma evacuation of his right medial thigh, removing approximately 3 litres (Figure 2).

Arteriogram after successful coil embolisation of Case 1 pseudoaneurysm, showing proximity of distal femoral interlocking screw.
During the haematoma evacuation, the orthopaedic surgical team visualised and removed the distal interlocking screw adjacent to the pseudoaneurysm. The external rotation deformity was assessed; however, a deformity of this severity would have required a significant revision procedure, so given the large size of the haematoma that had been evacuated and the concern for potential infection, the surgical team did not revise the deformity at that time.
Two months later, the patient underwent revision of the rotational deformity. This involved removal of hardware, subtrochanteric osteotomy and insertion of a long cephalomedullary nail. Since that procedure, the patient has been progressing well with physical therapy and has regained considerable strength in his leg. His haematoma has resolved, and his pain is significantly reduced.
Case 2
A 44-year-old male with no past vascular history presented to the vascular surgery clinic approximately 10 years status after ACL reconstruction with a history of chronic progressive erythema of his right lateral calf, as well as daily pruritus and localised oedema in his right anterior shin. Unfortunately, there is minimal history available during the intervening years since his ACL reconstruction and his presentation to our institution. Physical examination was significant for a mild rash with a few telangiectatic veins apparent on the anterior lower leg just distal to the knee. A palpable thrill and loud bruit were present over this area.
An arteriogram was completed and revealed an AVF originating from either the most distal portion of the popliteal artery or the origin of the anterior tibial artery. The tibial screw was visible at the level of the fistula. The decision was made to complete an open AVF repair with the vascular surgery team and screw removal by the orthopaedic surgery team.
The patient underwent a combined orthopaedic and vascular procedure. The vascular surgeon decided on an open approach because of the proximity of the arteriovenous malformation to the anterior tibial bifurcation and the orthopaedic tibial screw. A marginal incision was made in the right medial superior calf, just posterior to the medial tibial plateau and running parallel to the tibia. Vascular surgery explored the distal popliteal artery, anterior tibial artery and tibioperoneal trunk. The AVF was repaired with suture ligature and vessel clips at the level of the anterior tibial artery branch point, between the anterior tibial artery and two grossly dilated venae comitantes.
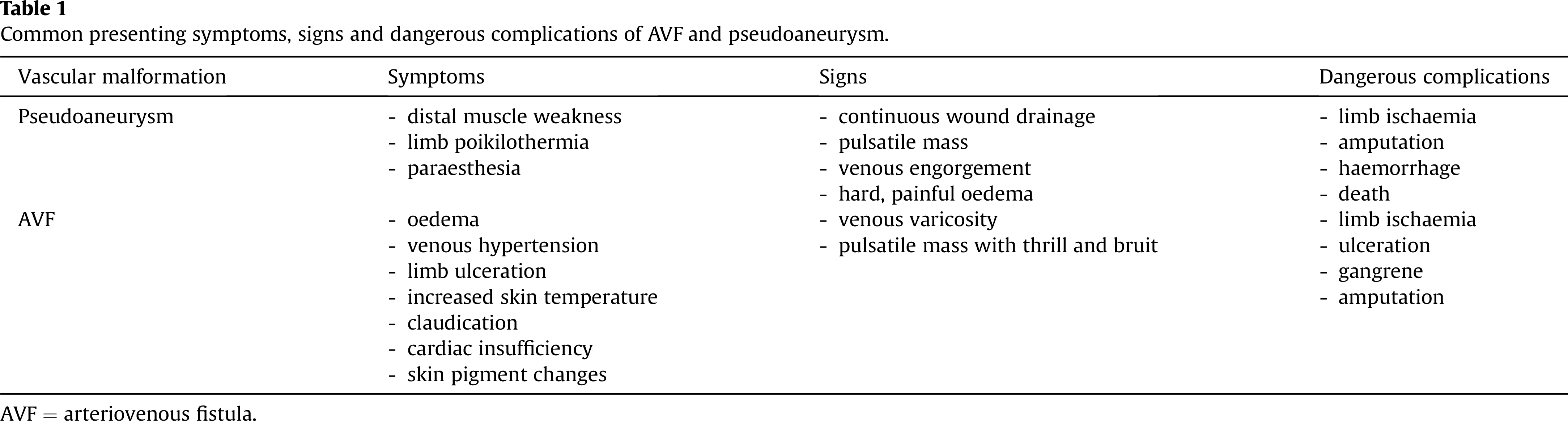
Once the vascular procedure was complete, the orthopaedic surgeon made a small incision overlying the anterior tibial tuberosity. The screw and washer were identified and removed. An intraoperative duplex ultrasound was performed on skin after the closure of the surgical incision. The popliteal and tibioperoneal arteries were evaluated with good velocities and without significantly decreased velocity between the two. All of the surgically involved veins were evaluated, and none were found to have evidence of arterial flow within them. A right lower extremity arteriogram was performed the next day and showed no residual AVF in the right calf (Figure 3).
(A) The before arteriagram from Case 2; (B) the after arteriogram from Case 2. There was no orthogonal or cross-sectional imaging available with the screw in place to measure penetration.
At 4 months postoperatively, the patient reported persistent numbness over his right anterior shin and medial malleolus with ipsilateral toe flexor weakness. An electromyography (EMG) test was consistent with a mild right tibial neuropathy, with his anterior shin sensory deficit supporting saphenous neuropathy as well. This could have been the result of inadvertent damage either with mild traction or from a compressive pathology given that he had oedema after the surgery. Yet another explanation could be vascular insufficiency to his saphenous nerve given the altered haemodynamics after AVF repair.
Slight weakness in toe flexion remained at his most recent follow-up, 8 months postoperatively. The patient denied pain that would indicate vascular claudication but stated that he had swelling in his right lower leg at the end of the day, which was likely due to mild venous insufficiency given good flow and absence of deep venous thrombosis on venous duplex. The patient wears compression socks for the swelling, and his pruritus and erythema have otherwise resolved.
Discussion
Vascular malformations can be caused by routine orthopaedic surgeries, and this report describes the rare complications of AVF and pseudoaneurysm. The pseudoaneurysm patient’s presenting signs and symptoms included oedema, subacute limb ischaemia, poikilothermia and hardening. The AVF patient’s presenting symptoms and signs included a prolonged history of erythema and oedema, pruritus and telangiectasias, as well as a palpable thrill and loud bruit. Although eventually recognised, each patient may have dealt with these complications for longer than necessary. As an orthopaedic surgeon, it is important to recognise the presenting signs and symptoms of vascular malformations (Table 1).
Common presenting symptoms, signs and dangerous complications of AVF and pseudoaneurysm.
AVF = arteriovenous fistula.
Pseudoaneurysms are a more common occurrence after orthopaedic procedures. Pseudoaneurysm of the femoral artery after internal fixation of a trochanteric fracture is caused primarily by overpenetration of the drill bit or screws. Yang described a case of pseudoaneurysm of the superficial femoral artery, likely caused by adduction and internal rotation of the involved limb placing the superficial femoral artery in close proximity to the medial femur while inserting the distal interlocking screws of a short cephalomedullary femoral nail. 8 A recommendation for avoiding this complication involves placing the limb in a neutral position during placement of the distal interlocking screws for short nails. In the reported case, overpenetration of the screw or predrilling likely caused the pseudoaneurysm. As seen in Figure 2, the screw was too long. This complication was recognised in the weeks following the index procedure when dramatic examination findings due to the massive haematoma caused increased concern. If not for those findings, the pseudoaneurysm may have gone unnoticed much longer.
The AVF patient was symptomatic for more than 8 years before undergoing AVF repair surgery, 10 years after his initial ACL operation. Given the low occurrence of AVF complications after ACL reconstruction, it is possible that the patient’s subtle symptoms were overlooked, and AVF may not have been considered in the years after his ACL reconstruction. AVF lesions are rarely seen after orthopaedic surgery and are most frequently caused by penetrating injury such as flying fragments, stab or gunshot wounds. 6 While studying potential neurovascular risks during ACL reconstruction, Post et al placed tibial tunnels arthroscopically in 10 cadaveric knees using standard tibial drill guides. 9 The popliteal artery and vein, and also the anterior tibial vein, were determined to be at greatest risk. Although tibial screws can be safely placed, Post et al noted that variations in anatomy and surgical technique could lead to vascular injury. In considering the dangerous potential complications of AVF, Pal et al conducted a case series and found one case of popliteal AVF complication in a review of 3,913 total knee replacements. 10 This postoperative patient, who had a previous history of bilateral venous ulcers, presented just 2 weeks after the index right knee replacement with ulceration leading to gangrene of the operative leg. Arteriography showed a right popliteal AVF, and the patient subsequently required amputation. This dangerous complication makes it imperative that surgeons be able to recognise the subtle symptoms of postoperative AVF.
Acute vascular injuries that result in delayed vascular malformations are rare but serious complications of orthopaedic procedures. When a drill bit or depth gauge overpenetrates, it places vascular structures on the contralateral side of the bone at risk. This is possible in most orthopaedic procedures, including ACL reconstruction and femoral fracture repair, as presented previously. Because the structures are distant to the operative field and the presentation is often delayed, it is possible that significant vascular injury initially goes unnoticed. This makes it imperative that surgeons recognise the presentation of delayed vascular malformations (Table 1). Identification of subtle symptoms can aid in the evaluation, diagnosis and early treatment to reduce limb-threatening long-term morbidity.
Footnotes
Conflicts of interest
The authors have no conflicts of interest with respect to the authorship and/or publication of this article.
Funding/support statement
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors, and no material support of any kind was received.