
Abstract
Extramedullary haematopoesis (EMH) in thalassaemic patients to result in spinal cord compression is a rare phenomenon. EMH occurs as compensatory sequelae in those with chronic anaemia such as thalassaemia, other congenital haemolytic anaemia, haemoglobinopathies, and myelofibrosis. Common sites of EMH include liver, spleen, kidneys and lymph nodes, but rarely the paravertebral and spinal cord regions. In our literature review, it was found that only case reports and case series have been published. We present a case of recurrent thoracic spinal cord compression caused by EMH in a 32-year-old thalassaemic Chinese man treated with surgical decompression and spinal stabilisation. The key to successful treatment is prompt diagnosis with early clinical suspicion, magnetic resonance imaging and individualised treatment for each patient. Surgical decompression provides immediate neural decompression while subsequent anaemia management may reduce the risk of recurrence. In the present case, a combination therapy of blood transfusion, surgical decompression and radiotherapy has been shown to deliver successful outcomes in such cases.
Introduction
Extramedullary haematopoiesis (EMH) occurs as compensatory sequelae in patients with chronic anaemia such as thalassaemia, congenital haemolytic anaemia, haemoglobinopathies and myelofibrosis. Common sites of occurrence are liver, spleen, kidneys and lymph nodes but rarely the paravertebral region of the thorax and spinal canal. Thoracic cord compression secondary to EMH is a true rarity. In our literature review, we found that only a handful of case reports and case series had been published since 1954. Early suspicion, prompt radiological investigations and multimodal therapy of blood transfusion, decompression surgery and radiotherapy are essential to maximise patients’ neurological recoveries.
Case report
A 32-year-old Chinese man with a background of thalassaemia intermedia was presented with gait instability for 5 months. He had a history of thoracic spine EMH with cord compression treated with laminectomy and adjuvant radiotherapy 15 years ago and a splenectomy performed at 24 years of age. He was initially treated with complete T6 laminectomy and partial T5 and T7 laminectomy with the excision of the EMH mass. Postoperatively, he received conformal radiotherapy of 20 Gy in 10 fractions. He regained full neurological recovery after the initial operation. Subsequently, he was under the care of a haematologist. Regular blood transfusion was offered to prevent recurrence; however, he refused with the fear of complications relating to iron overload. This time, he complained of bilateral lower numbness and gait instability. No back pain, upper limb neurological symptoms or sphincter disturbances were reported. Despite the gait instability, he was managing his activities of daily living and continued to work as an accountant.
On physical examination, a roundish thoracic kyphotic deformity was observed, and no tenderness at the thoracolumbar spine was found. Lower limb neurology examination revealed decreased light touch sensation in both the legs, hyperreflexia in both the knees and ankle jerks. His lower limb power was full, and no clonus was illustrated bilaterally.
Magnetic resonance imaging (MRI) of the thoracolumbar spine as shown in Figures 1, 2A and 2B demonstrated multiple bilateral paravertebral masses seen at T7–T11 levels and an extradural mass at the posterior part of the thecal sac ranging from T2 to T10 levels. Both masses are isointense on T1-weighted (T1W) images and hypointense on T2-weighted (T2W) images with contrast enhancement. The thoracic cord at T4-5 and T8-10 are compressed with increased cord signals at T4-5 and T9-10, suggesting myelopathy. Surgery was offered for symptomatic relief and prevention of further neurological deterioration.
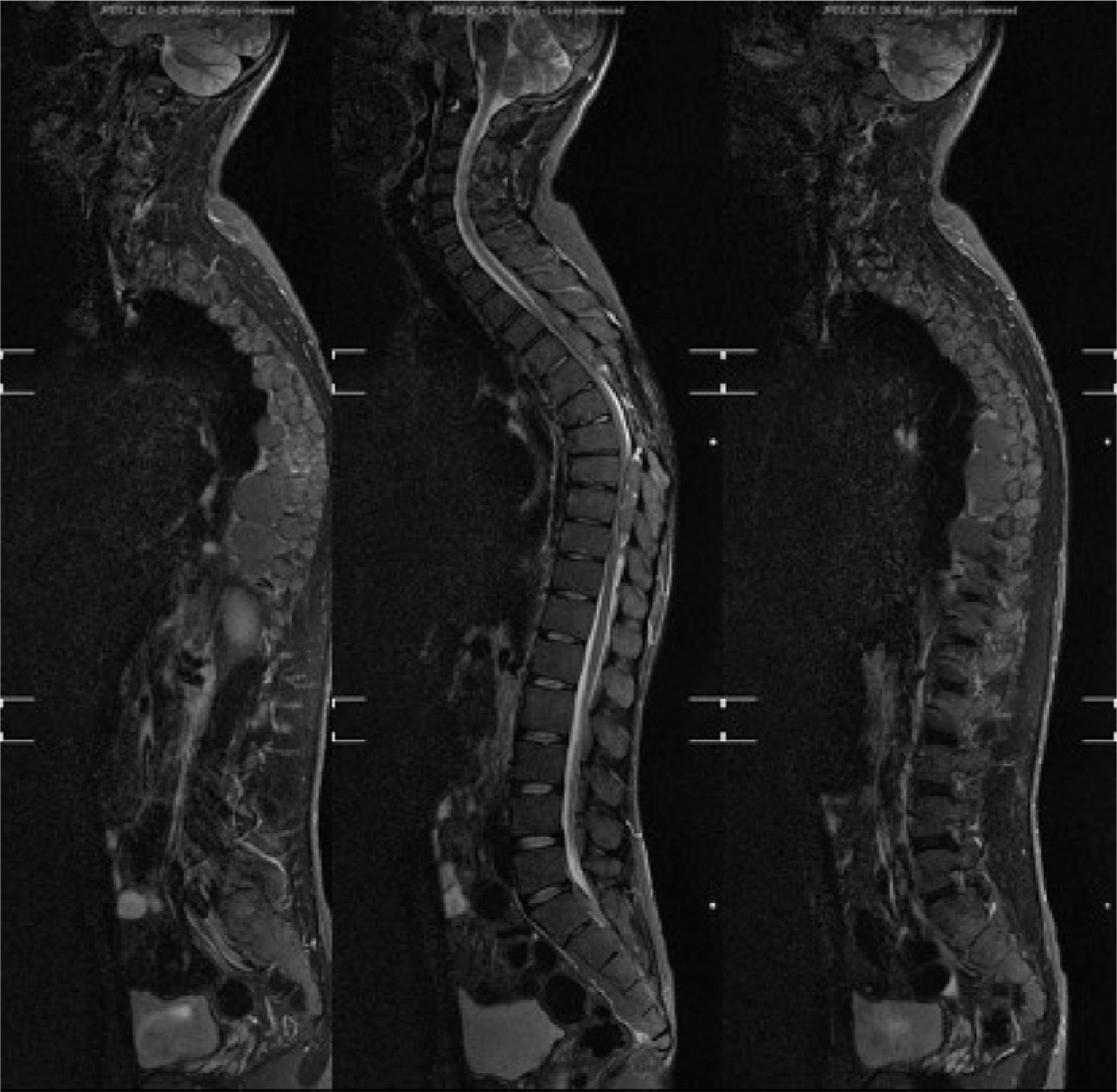
Preoperative MRI T2W whole spine sagittal view.
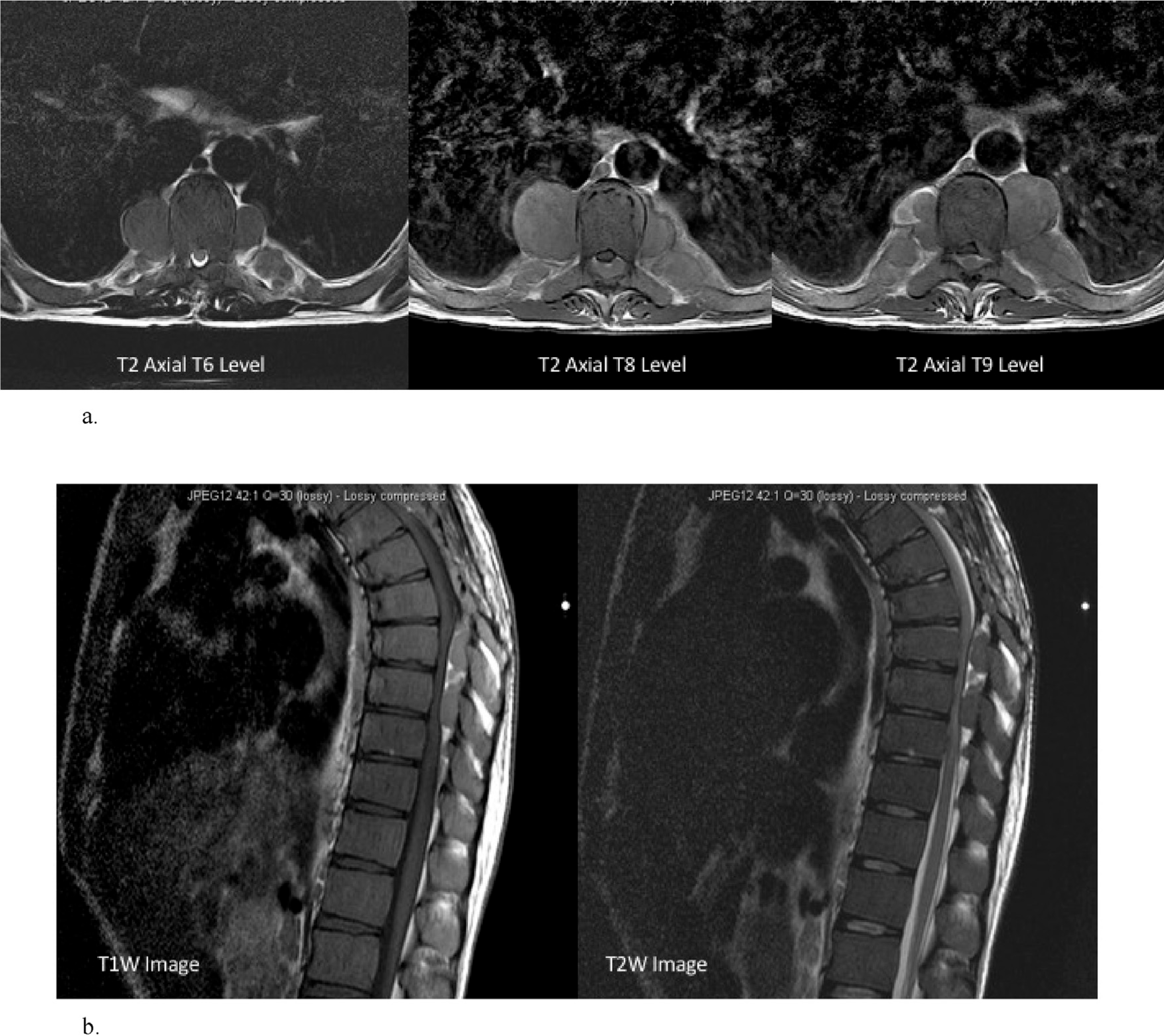
(A) MRI T2W axial T6, T8 and T9 levels. (B) MRI T1W and T2W thoracic spine sagittal view.
His haemoglobin (Hb) had been static between 8.5–10 g/dL, with haematocrit level of 23 and ferritin level of 2200. Supportive transfusions were given to reach a Hb level of >11 g/L preoperatively. This was also an attempt to reduce the EMH drive and to slow the growth of the mass. Preoperative embolisation was considered; however, it was not advised by the radiologists due to the extent of the lesion. The excision of extradural tumour, laminectomy of T3-5, T7-10 and posterior spinal fusion with instrumentation (T3-10) were performed. The operation was uneventful, and only a total of 350 mL of blood loss was recorded intraoperatively. Postoperative radiographs are illustrated in Figure 3. Histology of the excised tissue at T4 and T9 confirmed to be extramedullary haemopoietic tissue. Postoperatively, the patient reported minimal back pain with full lower limb power, the return of normal sensation and normal deep tendon reflexes. Upon discharge, he was fully ambulatory. Postoperative radiotherapy of 12 Gy 16Fr was given. His Hb level was between 8.8–9.2 g/L. Again, regular blood transfusion was offered by the haematology team, but the patient had again declined this treatment.
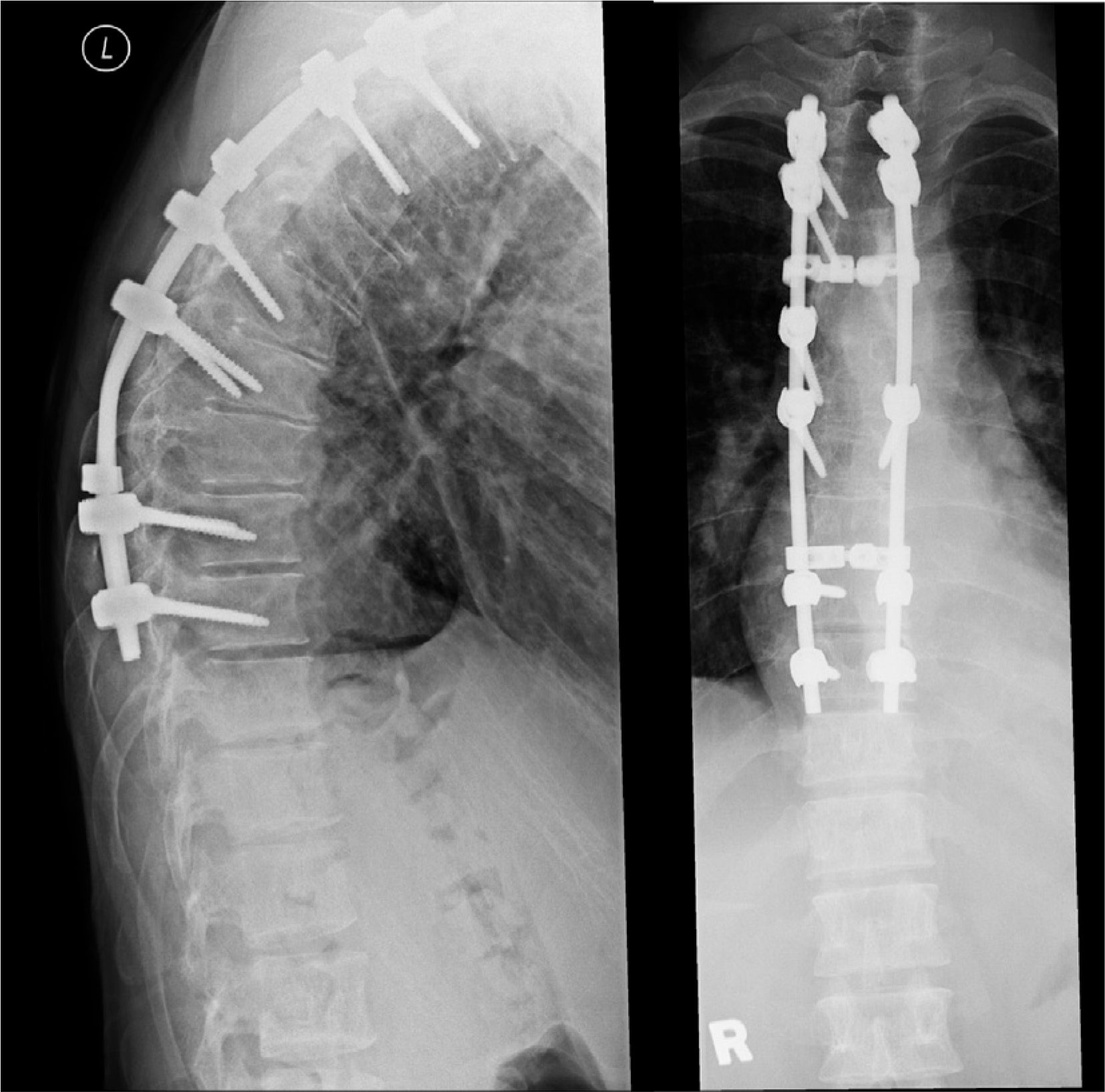
Postoperative X-ray thoracic spine.
Upon follow-up at 4 months, the patient was walking unaided with a normal gait without complaint of back pain. Clinical examination demonstrated normal lower limb power, sensation and reflexes. He was managing both his activities of daily living (ADL) and work without problem.
Discussion
EMH occurs as compensatory sequelae in patients with chronic anaemia such as thalassaemia, congenital haemolytic anaemia, haemoglobinopathies and myelofibrosis. Common sites of EMH formation include liver, spleen, kidneys and lymph nodes but rarely the paravertebral region of the thoracic spine. The clinical features are dependent on the site of formation of the haematopoietic tissue.
Spinal cord compression secondary to EMH is a rare condition. In our literature review, it was found that only case reports and case series have been published. In 1992, Singal et al 1 compiled a review of 37 cases, diagnosed by myelogram, from 1954–1988 in Table 1.
Reported cases of extramedullary haematopoiesis compressing the spinal cord in thalassaemia.
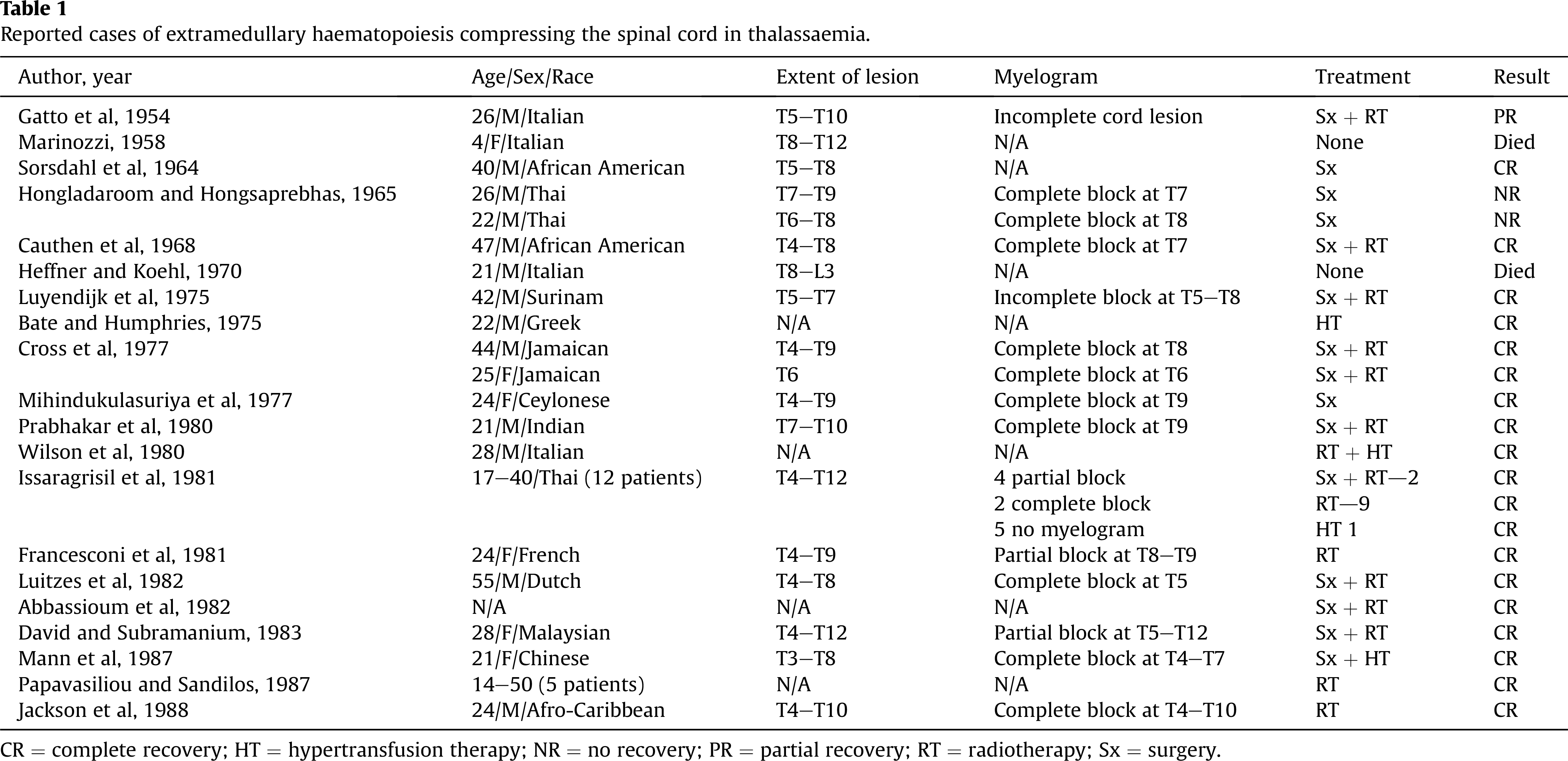
CR = complete recovery; HT = hypertransfusion therapy; NR = no recovery; PR = partial recovery; RT = radiotherapy; Sx = surgery.
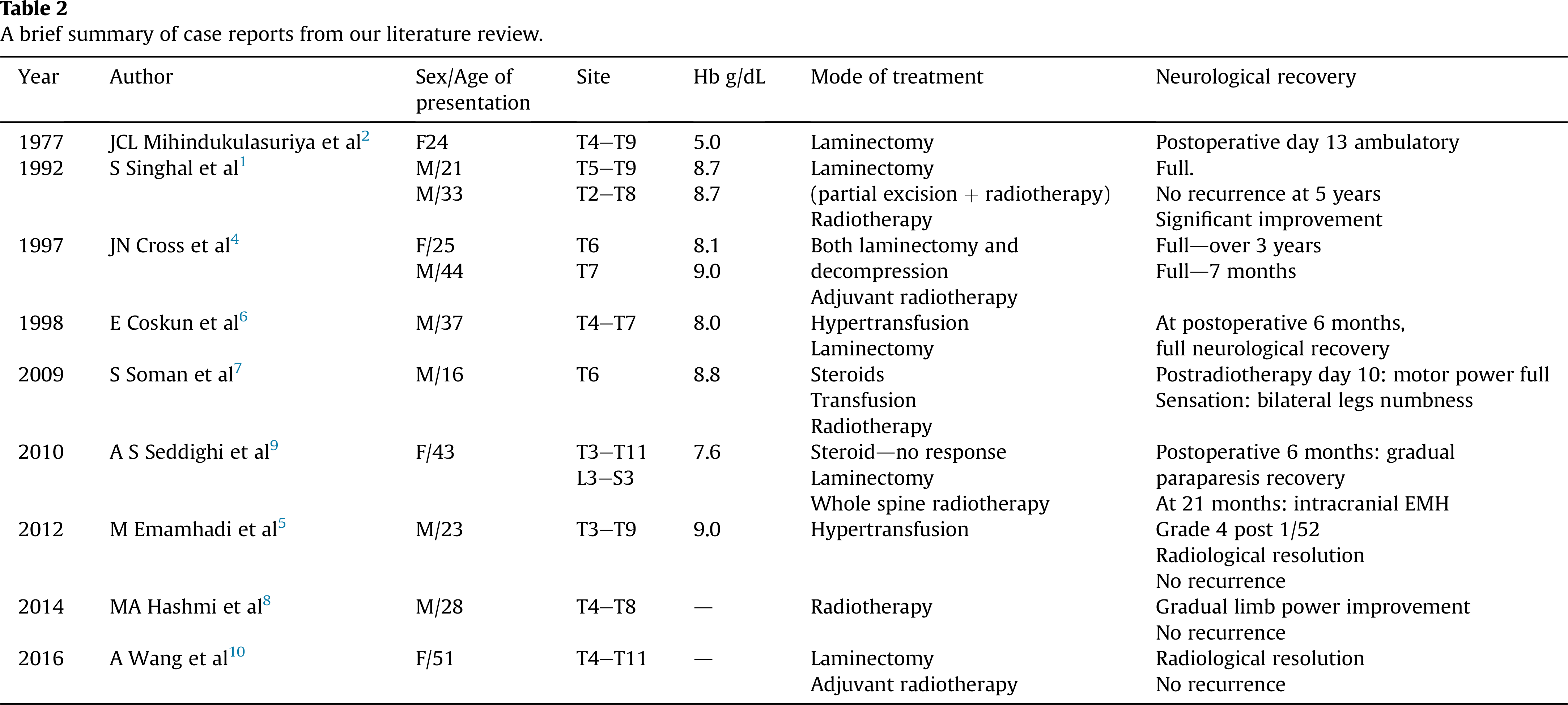
From our literature review, it was found that the paraspinal involvement of EMH occurs most commonly at the thoracic spine. Table 2 is a summary of all the cases reviewed in our literature review. In all the cases reported in the reviews, the cord compression from the EMH tissues were from the posterior aspect. No cases of anterior compression of the cord had been reported so far. The age of onset for these cases ranges between late adolescent years to the fourth decade. Nearly all cases presented with insidious disturbances of gait without loss of sphincter control.
A brief summary of case reports from our literature review.
Various schools of thought have been proposed for the origin of EMH in the thoracic spine. Most authors suggested that the haematopoietic tumour is a direct extension from the trabecular bone of the adjacent vertebral bone marrow or the proximal rib ends. Some authors postulated that the EMH mass occurs when remnant primitive tissue in the epidural space is stimulated in the event of chronic anaemia, whereas others proposed that the mass had developed from branches of the intercostal veins. The most common site of cord compression secondary to an EMH mass formation was the thoracic spine. This could be accounted by the narrow diameter of the spinal canal at the thoracic region. 2,3
Clinical suspicion is paramount for early diagnosis. On simple radiographs, the EMH mass may appear as well-confined, lobulated masses in the paraspinal region. 4 Apart from the secondary malignant metastasis, one important differential diagnosis is transverse myelopathy due to cord ischaemia from microcirculatory obstruction during haemolytic crisis. 4 Nowadays, MRI of the spine is relatively available compared to the times where myelography was used. It is the modality of choice for diagnosis and follow-up evaluation as it clearly delineates the extent of involvement from the soft tissue masses and the status of the spinal cord. Active lesions are hyperintense in both T1W and T2W MR images to the adjacent vertebral bone marrow and spinal cord. In inactive lesions, signals in both T1W and T2W images are either hyperintense because of fatty infiltration or hypointense because of iron deposition. When considering alternative differential diagnosis, tissue diagnosis remains the gold standard investigation. Computed tomography–guided biopsy may be used; however, one must bear in mind that EMH tissue is hypervascular. Uncontrolled, massive haemorrhage after biopsy may occur, leading to further cord compression with an epidural haematoma. Regretfully, there had been no suggestions concerning the actual site of biopsy from previous literature review.
Several treatment modalities have been used to treat EMH masses: hypertransfusion, surgical decompression and radiotherapy. Emamhadi and Alizadeh reported that their patient had rapid neurological recovery within days and complete resolution of the EMH mass on MRI within 1 week after being treated solely with hypertransfusion. However, the definition of hypertransfusion was unclear, and the authors failed to mention the amount of blood transfused and the subsequent level of Hb reached after hypertransfusion. 5 In Coskun et al’s report, it was mentioned that the patient received a total of 1200 mL of whole blood over a period of 2 days. After this, the patient had rapid worsening of his neurologic functions: paraplegia and sphincter dysfunction. Urgent laminectomy was performed with marked neurological improvement and return of sphincter functions postoperatively. 6 In summary, there is no consensus in the current literature in suggesting the ideal Hb level for treatment with hypertransfusion. Most literature reported that common reasons for noncompliance to transfusion therapies had been complications from iron overload and transfusion reaction. No recurrence rate with transfusion therapy alone had been mentioned in the literature review. Nevertheless, it has been suggested that clinical and radiological improvement with transfusion therapy is slow and temporary, hence repeated transfusion. The aim of medical therapy is to prevent progression. 3
Radiotherapy has been reported to be an excellent monotherapy and adjuvant or neoadjuvant therapy compared to surgery in patients with EMH mass. Haematopoetic tissue is highly radiosensitive, and in one case, it has been reported that the mass volume decreases by 16.4%. 3 In our literature review, many cases were treated with radiotherapy; however it is not without risks. First, recurrence rate is high, with rates up to 10–37%. 3 In, many cases, patients required further radiotherapy or surgical decompression. Second, during radiotherapy, the patients’ neurologic functions could further deteriorate from tissue oedema. Finally, the radiotoxicity could cause postoperative wound complications, further spinal cord injury and bone marrow suppression, exacerbating erythrogenesis in an anaemic patient. Clinicians must bear these considerations in mind and monitor the patient’s neurology and general condition closely during radiotherapy.
Surgical decompression is indicated for cases with acute cord compression or those for whom conservative treatment with radiotherapy or hypertransfusion has failed. Laminectomy and excision of the EMH mass provide immediate relief to the compressed cord, thus improving neurological recovery. At the same time, histology can be obtained. On the other hand, the possible risks and complications include major bleeding from the mass, incomplete excision of the mass in those multilevel involvement and instability of the spine from multiple levels of laminectomy. In our case, posterior spinal fusion with instrumentation from T3-10 was performed to prevent further deterioration of the preexisting kyphotic deformity postoperatively. Furthermore, Haider et al proposed that another drawback of complete excision of the EMH mass may cause haemodynamic and haematological deterioration and decompensation in the patient. 3 This is because the large, diffused EMH mass played a crucial role in maintaining a stable Hb level for the patient preoperatively. We recommend that these patients’ haemodynamic status and organ functions should be closely monitored in the intensive care setting in the initial postoperative period.
Our case was the first case of recurrence reported after decompression surgery, which could have been accounted by his refusal to blood transfusion. Vigilant monitoring of the anaemia condition and regular blood transfusion play a key role in eliminating the chance of recurrence.
In summary, EMH resulting in spinal cord compression in patients with thalassaemia is a rare occurrence. The key to a successful treatment is early detection and diagnosis of the disease with MR imaging and individualising the available treatments for each patient. A multimodal therapy comprising hypertransfusion, surgical decompression and radiotherapy has been shown to be effective in the literature review with low rates of recurrences. Regular, four to six monthly outpatient reviews with clinical examination, serological monitoring and follow-up MR imaging are recommended for early detection of recurrence of the EMH mass to prevent disabling neurological impairments.
Footnotes
Conflict of interest
None declared.