
Abstract
Purpose:
To evaluate the use of Metaizeau technique in the treatment of radial neck fracture in adults.
Method:
A total of eight patients were treated with intramedullary pinning (Metaizeau technique) using titanium elastic nails. All the patients suffered isolated radial neck fracture. Fracture morphology in all the patients had angulation more than 30° and were displaced, tilted with the impacted articular fragment. All the patients had Mason’s type III or Judet’s type II or III fracture. The mean age of patients was 31.3 years, and all were operated within 7 days of suffering the injury. The mean follow-up was 9 months. For subjective evaluation, patients rated their satisfaction for elbow use on a scale of 1–6. Objective assessment includes Mayo elbow performance score, active range of motion of flexion and extension and forearm rotation.
Results:
The active ranges of motion and hand grip strength were comparable in both upper limbs. Similarly, the range of flexion–extension and pronation–supination were identical. In all cases, the titanium elastic nails had already been removed after 8 weeks with osseous healing of the radial neck. Patients rated their satisfaction for elbow function as very good in six cases and good in two cases.
Conclusions:
In the present case series, the results of the use Metaizeau technique in adults were promising. The proper selection of the patient and timing of surgery should be considered judiciously. Further large case series is required to ascertain the results.
Level of evidence:
Level IV.
Background
Radial neck fractures are uncommon injuries in adults and more often found in children where they account for 5–8.5% of elbow injuries. 1 In adults, isolated radial neck fractures are very rare with an incidence of 1% of all fractures. 2 They are usually the result of a fall onto an extended and supinated forearm, which leads to the radial neck fracture and leads to angulation of the radial head. The prognosis depends on the degree of displacement, the age of the patient, associated elbow injury and the method of treatment. Less than 30 degree of angulation is generally acceptable.[ 1,3 –5 ] Poor results are generally associated with more degree of angulations and displacement. Restoration of radial neck angulation and displacement is essential to restore the normal biomechanics and stability of the elbow. Most minimally displaced radial neck fractures are treated conservatively with early initiation of physical therapy. 6 Conservative treatment might result in secondary displacement, malunion and cubitus valgus, whereas open reduction and internal fixation (ORIF) is associated with nonunion, implant-related complications, reduced range of motion (ROM), posterior interosseous nerve palsy, heterotopic bone formation and avascular necrosis of the radial head. The standard procedure accepted for isolated radial neck in paediatric age group is centromedullary pinning (Metaizeau technique). We performed this procedure on eight adult patients. The purpose of this case series therefore was to evaluate the functional outcome of radial neck fractures treated by intramedullary pinning (Metaizeau technique) in adults.
Methods
Between January 2016 and November 2017, a total of eight patients (four females and four males) were treated with intramedullary pinning (Metaizeau technique) using titanium elastic nails (TENS). The mean age of patients was 31.3 years, and all were operated within 7 days of suffering the injury. The study involves radial neck fracture suffered in three dominant upper limb and in five nondominant upper limb. The most common mode of injury was fall from height. All the patients suffered from isolated radial neck fracture without elbow joint instability. Fracture morphology in all the patients had angulation more than 30° and were displaced, tilted with impacted articular segment [Figures 1 and 2]. All the patients had type III fracture according to Mason’s classification and Type II or III according to Judet classification. The mean follow-up was for the duration of 9 months.
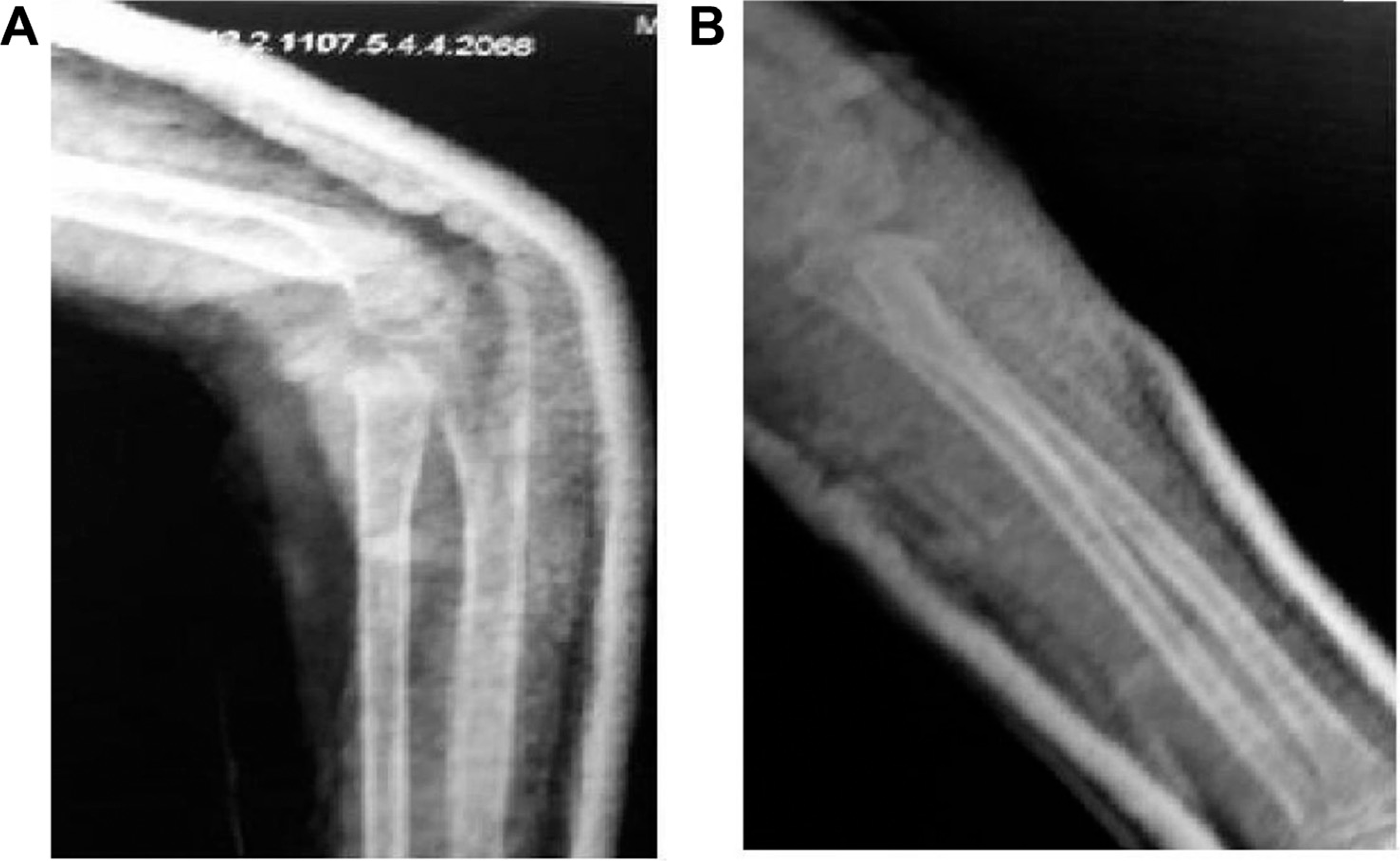
(A) Preoperative lateral view. (B) Preoperative AP view. AP = anteroposterior.
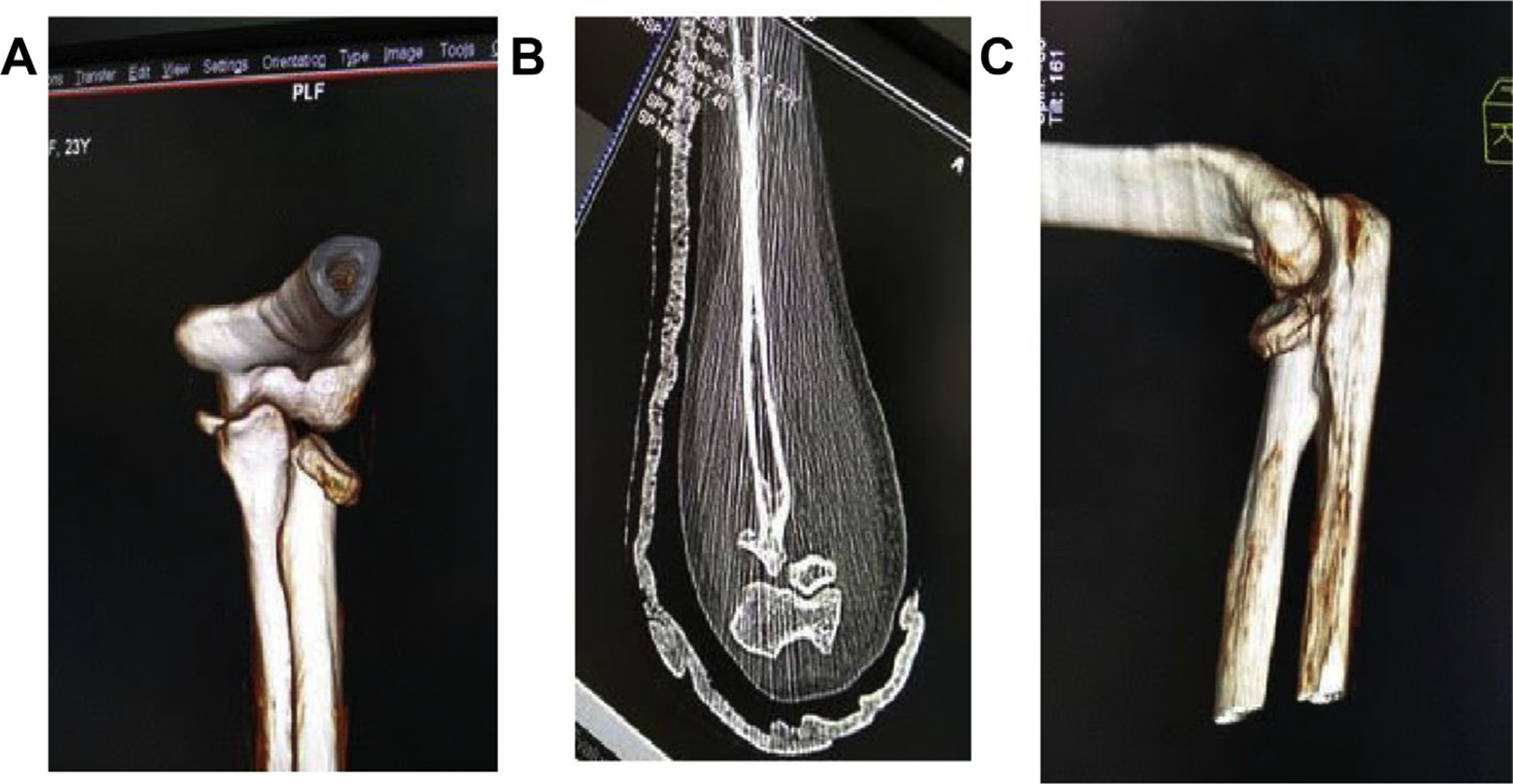
(A) 3D CT Reconstruction of elbow depicting the radial head angulation in AP view. (B) Coronal section of the CT Scan depicting fracture morphology. (C) 3D CT Reconstruction of elbow depicting the radial head angulation in lateral view. CT = computed tomography.
Surgical technique
The surgeries were performed by the technique described by Metaizeau, using intramedullary pinning. In all cases, the patient was placed supine with the injured arm on a radiolucent table under general anaesthesia. Before skin incision, fluoroscopy was performed to confirm joint stability. The metaphyseal area of styloid process of the distal radial styloid was marked with the help of an image intensifier. This serves as an entry point for the TENS. A 0.5-cm skin incision is given, and superficial branch of radial nerve was dissected, visualised and retracted carefully. The lateral radial cortex was exposed and perforated using a drill with a diameter of 2.5 mm. The TEN was introduced into the intramedullary canal. The nail was carefully advanced with the help of an image intensifier. Until the tip of the TEN reached the fracture site, it was carefully rotated to engage the proximal fracture fragment. Simultaneous digital pressure was applied with thumb to enable engagement of the tip of the nail and the fracture fragment. Gentle traction and varus forces help in manipulation of the proximal fragment. Once the tip got engaged with the proximal fragment, it was gradually rotated back in its place and confirmed with the image intensifier.
The other end of the nail was bent and cut near the wrist joint for easy removal after 8 weeks. According to the width of the intramedullary canal, one TEN with appropriate thickness was used for closed intramedullary pinning in all patients. All operations were performed with a mean interval from injury to surgery of 4 days (range 1–7 days). No additional surgical procedures were required in any case, except TENS removal. All patients were immobilised postoperatively with a plaster cast for 2 days for pain relief and subsidence of swelling [Figure 3]. Elbow hinge braces were given to all the patients. Active assisted ROM was allowed under physiotherapeutical control after 2 weeks. The TEN was removed after fracture healing, around 8 weeks, and elbow hinge braces were removed. There was progression in the ROM of elbow and strength of hand over 3 months. All patients were back to their respective profession with good function of elbow after 6 months of surgery [Figure 5].
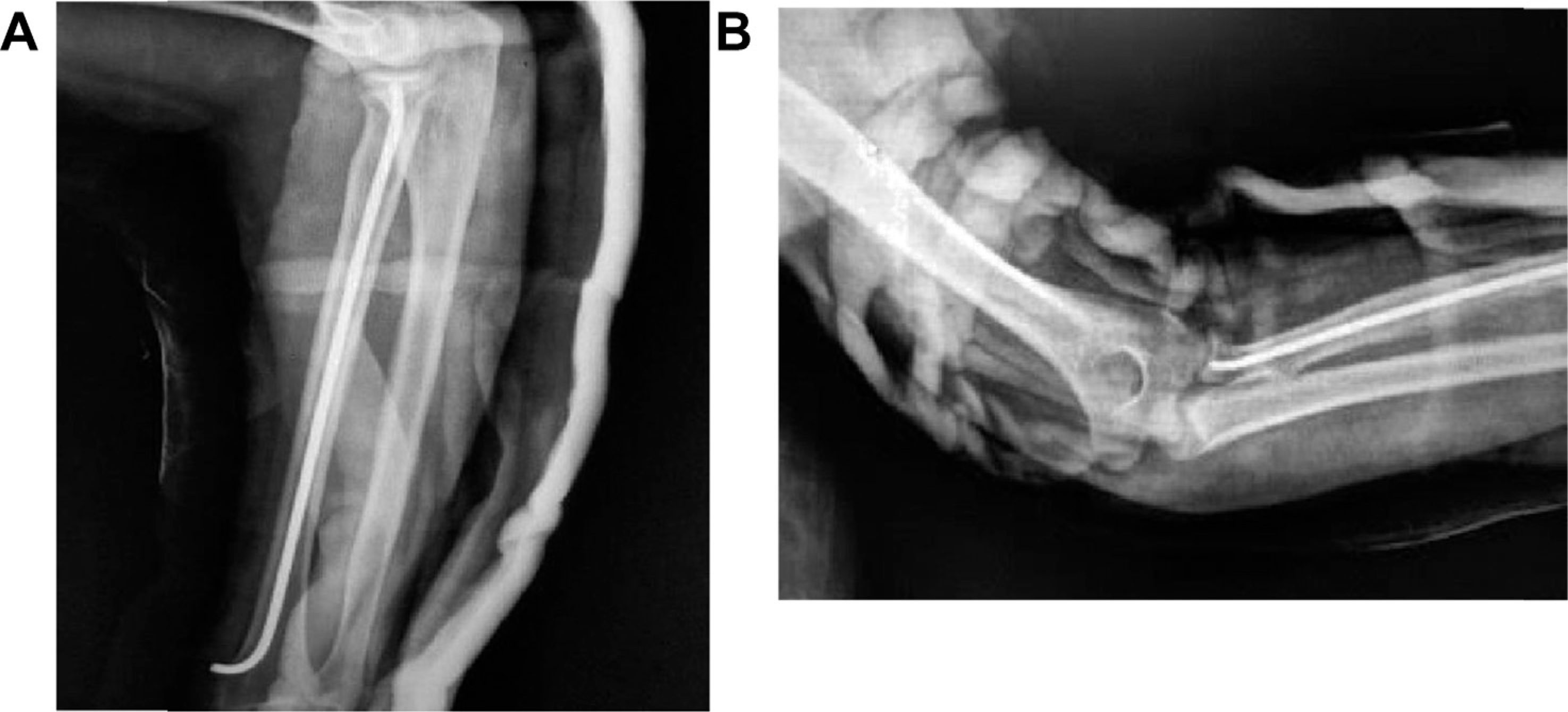
(A) Postoperative lateral view. (B) Postoperative AP view. AP = anteroposterior.
Evaluation
All patients gave written informed consent before being included to the study.
Personal interviews and Mayo elbow performance scoring were carried out for each patient.
For subjective evaluation, patients rated their satisfaction for elbow use on a scale of 1–6 (1—very good; 2—good; 3—satisfied; 4—sufficient; 5—insufficient and 6—poor). Objective assessment includes active ROM for flexion and extension and forearm rotation in both the elbows. Postoperative X-rays were evaluated immediately postoperatively [Figure 3] and 6 months later [Figure 4] to assess radiocapitellar joint, bone healing and heterotopic ossification.

(A) Xray lateral view at 6 months. (B) Xray AP view at 6 months.
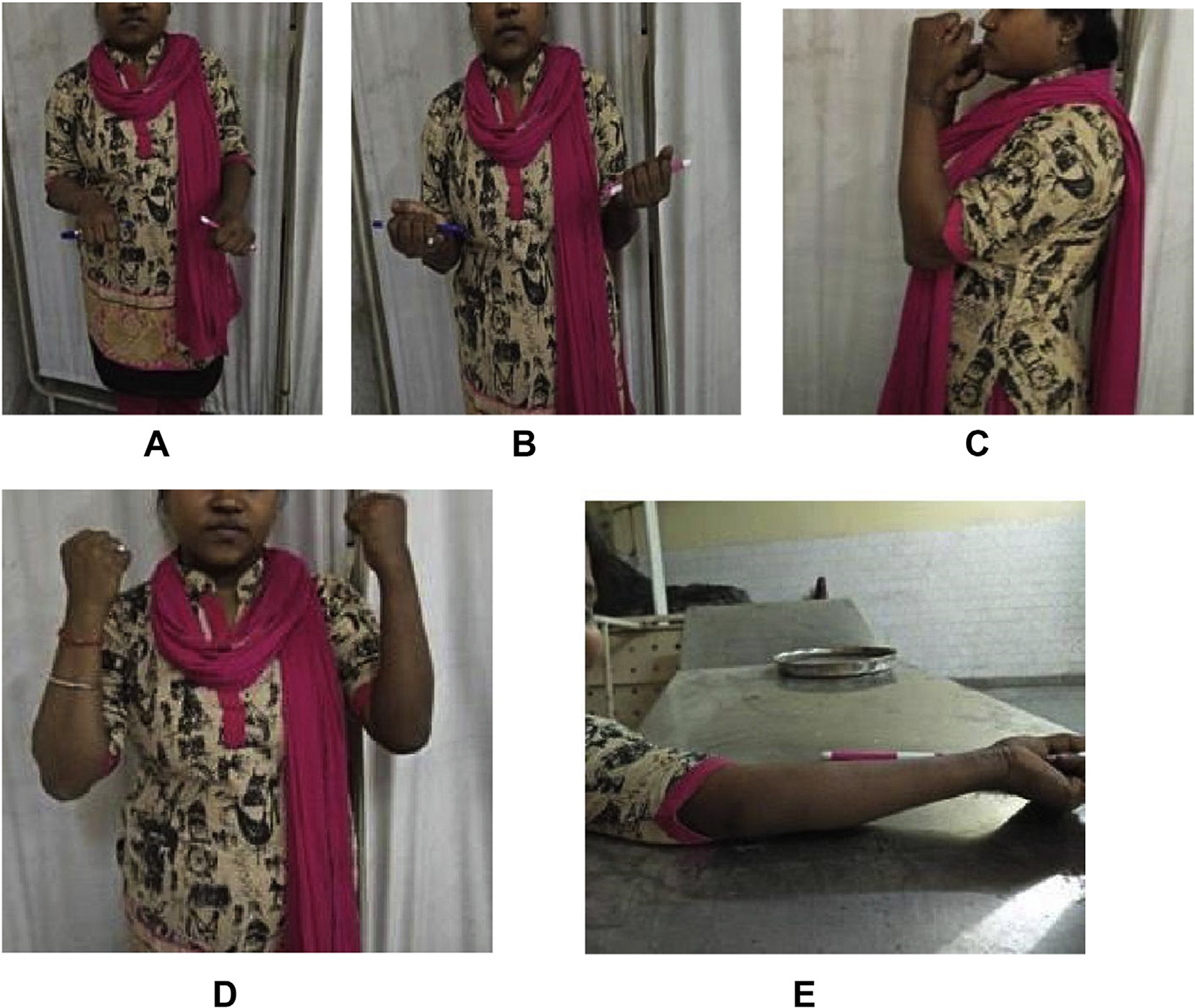
(A) Pronation of both forearms. (B) Supination of both forearms. (C) Flexion of elbows- lateral view. (D) Flexion of elbows- AP view. (E) Extension of elbow.
Results
The active ROM was comparable in both operated and nonoperated sides. Similarly, the strength for flexion–extension and pronation–supination was identical in both the upper limbs in all operated patients. None of the patient was an active sportsperson.
At the time of follow-up evaluation, in all cases, the TEN had already been removed with osseous healing of the radial neck after 8 weeks. None of the patient suffered from heterotopic ossifications or avascular radial head necrosis. Follow-up radiographs showed a congruent radiocapitellar joint in all cases without any secondary loss of reduction or secondary displacement of the radial head.
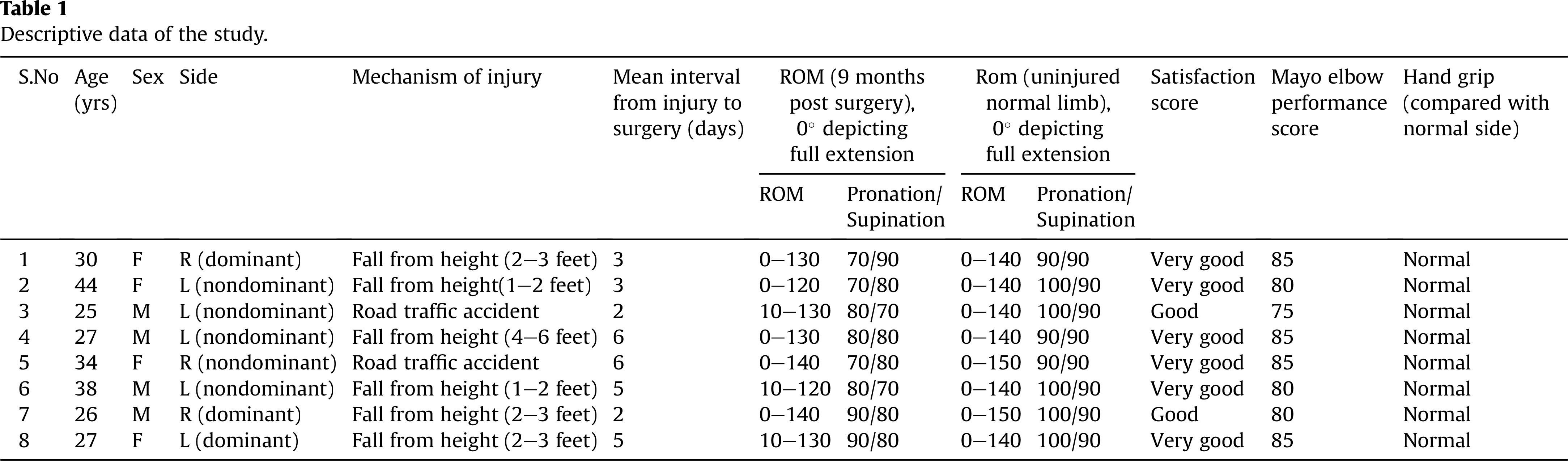
All results are summarised in Table 1. At the time of follow-up, patients rated their satisfaction for elbow function as very good in six cases and good in two cases. Average Mayo performance score was 81.8. Hand grip strength was found to be comparable with that of normal uninjured limb.
Descriptive data of the study.
Discussion
Radial neck fractures are rare fractures more common in children than in adults. Radial neck fracture in adult poses a unique set of problems compared with that in children. The reduction of fracture with manipulation is difficult. Various surgical procedures have been described for fixation of fracture of radial neck in adults. Most surgical procedures include ORIF using various types of plates. The bone-healing potential of adults is less than that of children, and soft tissue and periosteum stripping while placing plates further hampers it. Metaizeau technique does not hamper the fracture-healing milieu. Undisplaced or minimally displaced radial neck fractures (angulation < 30°) are managed conservatively by immobilisation in slab/cast for 4–6 weeks. In children, for displaced radial neck fracture (Judet III and IV type), closed reduction and intramedullary pinning technique (Metaizeau technique) are considered the treatment of choice. 7 –9
The advantage of this minimal invasive technique includes avoidance of implant-related complications such as screw dislocation or perforation affecting the proximal radioulnar joint. The ORIF is associated with a higher rate of avascular necrosis, 10,11 proximal synostosis, 12 heterotopic ossifications, 13 infection, posterior interosseous nerve palsy and loss of ROM, 14 especially in those cases where the plate has to be positioned out of the safe zone because of fracture pattern. 15 There is no surgical scar near the elbow or disruption of internal milieu of the elbow leading to stiffness of the joint.
In this study, we extended this technique which is considered safe in children for displaced radial neck fracture in adults. This technique can be used in a unique set of radial neck fractures in adults. The pattern and displacement of fracture which cannot be managed conservatively yet can be reduced by manipulation requiring stabilisation by intramedullary pinning are perfect candidates for this surgical technique. For such fractures, ORIF using plates might be an overzealous approach. The reduction manoeuvres are done under fluoroscopic guidance by manipulation through closed reduction or using K wires percutaneously. 16 The fracture should be reduced within 7 days of injury in adults. Later on, fracture reduction will not be possible because of fibrosis and fracture healing.
The study carried out by Serbest S et al 17 initially used the technique in a single case. The results were suggestive of success of this surgical approach in adults. But, further studies were needed because of the small patient number.
The study carried out by Sandmann GH et al 18 also depicted the successful treatment performed for radial neck fracture in eight adults by Metaizeau technique.
Our study depicts excellent functional results of this technique in isolated displaced radial neck fractures in adults. Nevertheless, this technique has some fallacies. The disadvantage of this technique includes affection of superficial radial nerve leading to hyperaesthesia of supplied area of skin. Second surgery is required to remove TENs. Single TEN may not be sufficient to prevent rotation of the radial neck.
Nevertheless, this case series advocates the use of the Metaizeau technique in adults. It has to be clearly mentioned that in mature patients, the intramedullary procedure should be performed within the first week after trauma to obtain anatomical reduction of the displaced radial head. The reduction of displaced radial head is utmost important in maintaining the congruity and stability of the elbow joint. Nevertheless, this study was not the first to advocate this result, but it reinforces the support for this procedure as advocated. Owing to rarity of this fracture pattern, a multicentric randomised controlled trial with long follow-up is required to formulate the guidelines for radial neck fractures in adults.
Conclusions
In the present case series, the results of the use Metaizeau technique in adults were promising. The proper selection of the patient and timing of surgery should be considered judiciously. This minimal invasive technique, which is the treatment modality of choice for displaced radial neck fractures in children, can serve as an alternative for adults also. Furthermore, long follow-up and large case series are required to inculcate this procedure as surgical standard of management for radial neck fracture in adults.
Footnotes
Conflicts of interest
The authors declare that there are no conflicts of interest.
Appendix A. Supplementary data
Supplementary data related to this article can be found at https://doi.org/10.1016/j.jotr.2018.03.005.