
Abstract
Background:
This article describes a prospective cohort study trial which aims to determine what risk factors might be associated with increased levels of pain, disability and psychological distress following simple orthopaedic trauma.
Methods:
Patients were recruited from two large tertiary referral hospitals. Outcome measures were return to work, measurement of the visual analogue scale for pain and the SF 12 physical component score (PCS) and mental health component score.
Results:
Fifty-five participants were recruited. Overall, participants had significant improvement in their levels of pain, and all who were working before the injury returned to work. Those with a preexisting disease had a significantly lower (p = 0.007) initial PCS with no significant changes in either mental health component score or PCS.
Conclusions:
Differences in outcomes were observed in patients with and without preexisting disease.
Keywords
Introduction
Orthopaedic trauma is common and is considered to have a significant impact physically, psychologically and financially at an individual and society level. 8 According to the Australian Institute of Health and Welfare, 8 a fracture was recorded as a diagnosis for 156,450 episodes of inpatient hospital care in 2002; no updated figures are publicly available. Transport accidents in young and middle-aged people and falls in the elderly and the young accounted for 52% of these fractures. They are the most common cause of hospitalised trauma. Males make up 56% of these injuries.
An isolated limb fracture is not usually considered a high severity injury. On the injury severity scale (ISS) with a highest score of 75, a closed tibial fracture would score a 4. 9 An ISS of >15 is associated with increased mortality and >8 increased morbidity. 10 This highlights that although considerable force is required to break a healthy bone, associated morbidity should be low. A combination of the trauma and pain of the event itself, the treatment which may involve surgery and the recovery period are likely to be part of the explanation why recovery from these simple fractures is not always predictable.
Pain is a complex phenomenon, often divided into acute and chronic phases. There is increasing evidence that the perception of pain, even acutely, is not predictable and not related purely to the degree of damage sustained. 11 There is also evidence that the degree of initial pain reported by the patient has some correlation with their functional outcome. 5 Identifying those suffering high pain levels and managing them appropriately may be one way to improve outcomes.
Another phenomenon is the impact of the trauma on the person. This has been the subject of a Cochrane review. 12 Quantifying how the trauma itself may contribute to poorer outcomes may be harder to do. The use of simple tools such as the SF12, 13 a quick survey designed to assess mental and physical functioning, could give an early indication of those at risk of psychological distress.
The person themselves must be considered when analysing outcomes. Preexisting conditions such as diabetes are considered to have an impact on recovery from injury and surgery. 14 The preexisting diseases highlighted in orthopaedic literature are diabetes, smoking and use of steroids and anticoagulants. 15,16
The purpose of this study was to investigate the outcomes after orthopaedic trauma requiring at least 6 weeks of non–weightbearing (NWB), in terms of pain, return to work and physical and mental health and to answer the question, are they different in patients who identified as having a preexisting disease.
Methods
This was a prospective cohort trial, with level of evidence 2. Participants were recruited from the Orthopaedic Units at two acute hospitals. Participants who had sustained a lower limb trauma requiring a period of at least 6 weeks NWB were asked if they would be willing to complete a series of surveys. Over a 12- month period, all patients who presented were given this opportunity. This patient population was chosen to identify a group seen commonly in orthopaedic outpatient clinics that had to alter their lifestyle to accommodate their recovery. Use of crutches alters gait patterns and introduces a weight-bearing load to the upper limbs; it has also been associated with complaints of occurrence of new, upper or lower limb pain. 17
Recruitment was done either in Outpatients or in the ward, after definitive management of the fracture had occurred and at the beginning of their period of NWB. A period of NWB was used as inclusion criteria so that participants experienced a significant change in function. Potential participants were approached if they met the inclusion criteria of being over 16 years of age and having sustained an isolated lower limb injury requiring a period of at least 6 weeks NWB and were willing and able to provide informed consent and complete the questionnaires. Exclusion criterion was any other injury sustained by the patient. Ethics approval was sought and obtained from the Human Resource Ethics Committees at both institutions.
At the initial visit, participants filled several questionnaires. The first addressed demographics, medical history and presented a pain visual analogue scale (VAS) alongside a body chart. The VAS gives a score of 0–10 for pain, with 10 being the worst possible pain score. The body chart was for the participant to shade in or circle the areas in which they felt pain. This was important to determine their baseline areas of pain. The participant also completed an SF12, a short questionnaire designed to provide insight into their current level of physical and mental health. There are two scores for the SF12, which is a simpler version of the SF36, a physical component score (PCS) and a mental component score (MCS). Scores are between 0–100 with higher scores indicating better health. This has been validated for use in this population. 18 At the follow-up review, participants completed the VAS, the body chart and the SF12. In those patients reporting new pain areas at the follow-up review, a further phone call was made between 6 and 12 months post injury to determine their ultimate outcome regarding pain from the injury.
IBM SPSS, version 22, was used for the statistical analysis with the significance level set at 0.05. Differences between the participants who had a preexisting medical condition at the time of diagnosis and those who did not have were compared using a Pearson’s Chi-square test (or a Fisher’s exact test) for categorical variables and a Mann–Whitney U test for continuous variables. Nonparametric tests were chosen because of the small sample size in each group. The null hypothesis was that there would be no difference in any of the variables between the groups. Comparison over time between SF12 MCS, SF12 PCS and VAS pain scores were analysed using Wilcoxon signed-rank test.
Results
A total of 55 patients were enrolled in the study after review in an orthopaedic outpatient clinic for a significant lower limb injury. All patients sustained an injury below the level of the knee joint. Five patients were unable to be contacted for the follow-up questionnaire and subsequently lost to follow-up. Demographic data for these patients are presented in Table 1 and demonstrate no statistically significant difference between the cohort of patients who completed the study and those who were lost to follow-up. Of the remaining 50 patients, 30 were male (60%) and 20 were female (40%) with the median age of the cohort being 45 (interquartile range = 28.00).
Demographics of patients who were lost to follow-up compared to study participants.

Of the 50 patients, 17 patients reported a preexisting medical condition at the time of injury. The questionnaire specifically asked about diabetes, regular corticosteroid use, anticoagulation and smoking. These are factors that have been identified as likely to contribute to reduced recovery following orthopaedic trauma. 14 There was no significant difference in gender, age, body mass index, injury type and management of the injury between the two groups (Table 2).
Comparison of demographics of patients with preexisting medical conditions.
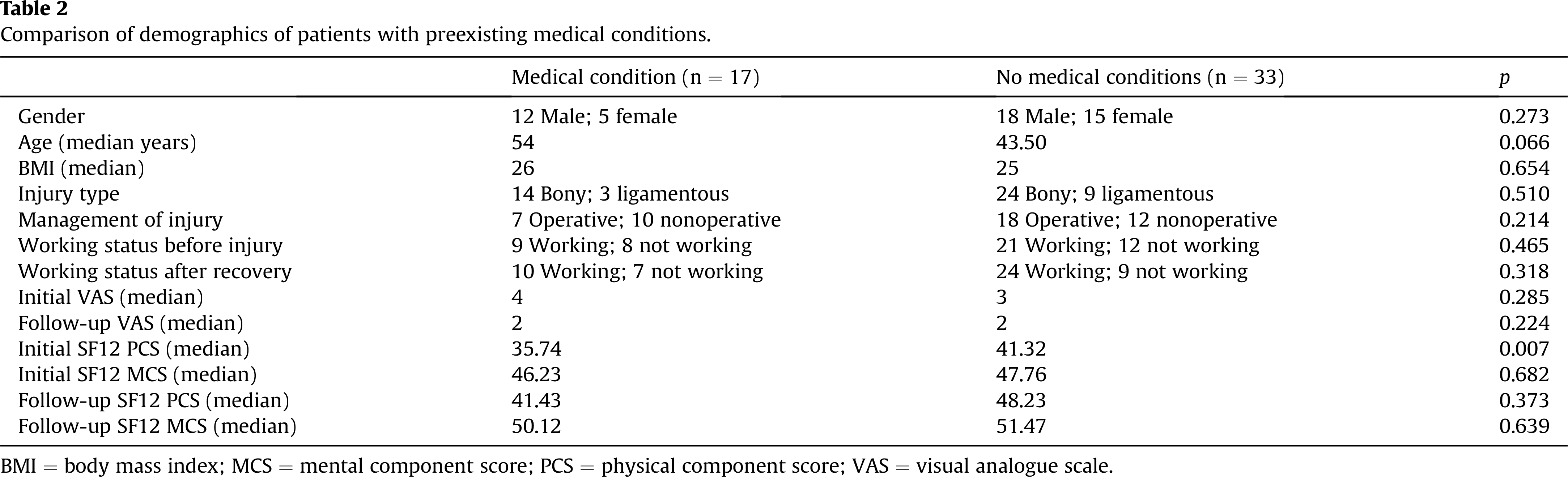
BMI = body mass index; MCS = mental component score; PCS = physical component score; VAS = visual analogue scale.
Initial and follow-up pain scores and initial and follow-up SF12 MCS also demonstrated no significant difference (Table 2); however, a significant difference was noted in initial SF12 PCS scores with patients with preexisting medical conditions scoring significantly lower than the rest of the cohort (p = 0.007) (Table 2).
Pain scores, SF12 PCS and SF12 MCS scores were compared from initial injury diagnosis and then again at the end of the NWB period. Patients who had preexisting medical conditions had a significant improvement in their VAS (p = 0.028) and no significant change in their SF12 PCS and SF12 MCS scores (Table 3), whereas patients who had no medical conditions showed a significant change in their VAS (p = 0.003) and SF12 PCS scores (p = 0.016) and no significant change in their SF12 MCS scores (p = 0.481) (Table 3). Essentially, they returned to premorbid levels.
Change in pain, SF12 PCS and MCS scores in the cohort.

MCS = mental component score; PCS = physical component score; VAS = visual analogue scale.
Discussion
This study has shown a significant difference in the initial PCS of the SF12 and a failure to significantly improve in the PCS following lower limb injury in patients with preexisting disease when compared to those without preexisting disease. It also showed that, in this cohort, return to work and resolution of pain were better than those generally reported in the literature. 1 –3,5 All those working initially did return to work and there was a significant improvement in pain VAS in all participants.
The heterogeneous nature of injuries in study participants added to the generalisability of the outcomes. The aim was to identify a group of patients who had undergone simple limb trauma requiring similar management and included at least 6 weeks of change in life activities, ie use of crutches, and obtain simple, easily reproducible outcome measures. Most of the patients sustained bony trauma, and those with ligamentous injury had comparable management strategies; so it was concluded we could analyse their data together. From this sample, those who were identified as having a preexisting disease were compared to those who did not.
The PCS is a measure of physical function. Our questionnaire included details regarding injury factors, premorbid mobility level and review by a physiotherapist to prescribe the use of crutches. There were no differences between groups, yet the preexisting disease group reported a lower level of initial function and a failure to significantly improve after cessation of the NWB period. There could be many factors contributing to this. One might be the perception of physical function being different in those with preexisting conditions. Another might be they have less physical reserve so that similar impairments cause bigger functional problems. Diabetes, one of the specific premorbid conditions asked about in the questionnaire has been associated with poorer outcome following ankle trauma. 16,19 Our sample size precludes a separate analysis of these diseases; however, future research should include a focus on defining preexisting disease and the impact that individual diseases have on simple orthopaedic trauma.
There is some evidence that people with preexisting disease have a predisposition to suffer pain and disability. 5,20 This, plus the exposure to the traumatic event, may cause disruption to the hypothalamic pituitary axis leading to impairment of cortisol production thus impacting all body systems. 20 It is conceivable this could lead to outcomes such as delayed healing, produce tissue of poorer quality, and even change the perception of pain.
This study found that participants, overall, had good outcomes from trauma. It is possible that some psychological intervention was enacted in the simple application of a questionnaire, which was then followed up. A recent Cochrane review found some evidence that identifying, targeting and monitoring patients at risk of poor outcome following a traumatic injury may reduce secondary disability. 12
The primary limitation of this study was in participant numbers. Higher numbers would have enabled the study to analyse outcomes based on different premorbid conditions. The prospective nature of our study helped minimise selection bias, and the high number of follow-up surveys completed minimises transfer bias.
Conclusion
This prospective cohort study has shown a difference in the impact and outcome of simple orthopaedic trauma on patients with preexisting disease when compared to those without. It highlights that the poor outcomes reported in the literature from simple trauma may be related to risk factors such as premorbid conditions. Future research should be directed towards larger prospective studies aiming to identify what these risk factors are and how different diseases interact with recovery from simple orthopaedic trauma and to evaluate the impact that simple interventions, such as questionnaires and offering simple psychological support, may have on residual pain and disability.
Footnotes
Funding
Rachele received a UQ Research Scholarship while in undergraduate study in 2014 to begin this work.
Conflicts of interest
The authors have no conflicts of interest relevant to this article.
Acknowledgements
The authors would like to acknowledge Dr Lisa Major for helping with initial data entry and Dr Diana Kennedy for assisting with initial study format.