
Abstract
Objective/Background
The purpose of this pilot study was to examine the effectiveness of standard earmuffs and noise-cancelling (NC) headphones in controlling behavioural problems related to hyper-reactivity to auditory stimuli in children with autism spectrum disorder (ASD).
Methods
Twenty-one children with ASD aged 4–16 years (16 boys and 5 girls), after a 2-week nonwearing baseline period, were asked to use standard earmuffs and NC headphones for 2 weeks, in a random order. Parents or teachers rated participants’ behaviours that were related to their reaction to auditory stimuli.
Results
Four participants refused to wear either the earmuffs or the NC headphones. It was found that the T-score on the Goal Attainment Scaling was significantly higher during the earmuff period than that in the baseline period (Z = 2.726, p = .006). The behaviours of 5 children with ASD improved during the NC headphone period as compared with those in the baseline period; there were no differences in the T-scores on the Goal Attainment Scaling between the NC headphone period and the baseline period (Z = 1.689, p = .091) and between the earmuff and NC headphone periods (Z = −0.451, p = .678).
Conclusion
This study demonstrated the effectiveness of standard earmuffs and NC headphones in helping children with ASD to cope with problem behaviours related to hyperreactivity to auditory stimuli, therefore, children with ASD could use earmuffs to help to deal with unpleasant sensory auditory stimuli.
Introduction
Hyper-reactivity to auditory stimuli is a common problem in children with autistic spectrum disorder (ASD).
Children with ASD who have auditory hyper-reactivity (ASD-AH) are bothered by auditory stimuli that they find intolerable, therefore, it is very important to find a way to manage auditory stimuli in daily life. Earmuffs, earplugs, and noise-cancelling headphones (NC headphones) are examples of equipment designed to protect individuals from harmful auditory stimuli. Some authors suggested earmuffs, earplugs, or headphones to parents or practitioners working with children with ASD (
The purpose of this study was to examine the effectiveness of earmuffs and NC headphones in controlling behaviours related to hyper-reactivity to auditory stimuli in children with ASD. To the best of our knowledge, this was the first study that examined the effectiveness of these devices in controlling behavioural and emotional problems in children with ASD-AH.
Methods
Participants
Participants were recruited from 220 families who were members of the Autism Society of Nagasaki, Japan, from April 2013 to September 2014. We informed the parents about our plan to hold workshops on sensory problems in children with ASD, then two workshops were run during the study period. In the workshops, after explaining the study methods and inclusion criteria, we invited 65 parents (mothers or fathers) who were present in these workshops to participate in the study with their verbal and written consent. The same procedure was repeated for eight families who were not present at these workshops. Inclusion criteria were: (1) the child was diagnosed with autistic disorder; (2) Asperger's disorder; (3) pervasive developmental disorder not otherwise specified; (4) was aged between 3 years to 17 years; and (5) had hyper-reactivity to auditory stimuli. Parents of 25 children with ASD who met the inclusion criteria (age range 4—16 years, mean age 8 years 2 months ± 36 months; 19 boys and 6 girls) expressed their willingness to participate in this study. All participants had already been diagnosed by paediatricians based on Diagnostic and Statistical Manual of Mental Disorders-IV criteria (
This study received prior approval from the Human Investigation Committee of the Nagasaki University Graduate School of Biomedical Sciences (Number 08091132).
Equipment
Earmuffs (
Outcome measure
Goal Attainment Scaling
To evaluate changes in behaviour during the baseline control period, earmuff period, and NC headphone period, Goal Attainment Scaling (GAS) was used. The GAS provides a standardised means to capture the diversity of meaningful functional outcomes (
The attainment levels for the chosen personal goals were then combined in a single aggregated T-score by applying the recommended formula which accounts for variable numbers of goals, inter-correlation of goal areas, and variable weighting (
where w i = weight assigned to the ith goal and x i = the score of the ith goal.
Procedure
Participants were randomly assigned to one of two experimental schedules that consisted of a sequence of a 2-week control period followed by 2 weeks of earmuff use and 2 weeks of NC headphone use, or a sequence of a 2-week control period followed by 2 weeks of NC headphone use and 2 weeks of earmuff use. Randomisation of the experimental schedule was done using the RAND and SORT functions in MS Excel (Microsoft Excel 2013) by the third author. Each participant had to decide whether to use earmuffs or NC headphones for the whole day or part time, however, the parents and teachers had to record the total time of using earmuffs or NC headphones per day.
Because it was necessary to observe the children's behaviour at all time, the children's GAS rating was checked by the teacher at school and by the parent at home.
Statistical analysis
The GAS T-scores for each period were calculated for each participant. The T-scores of all the participants were compared between the control period, the NC headphone period, and the earmuff period. The Shapiro—-Wilk test indicated that the T-scores in the baseline period were not normally distributed (W = 0.826, p = .021), therefore, we used the Wilcoxon rank sum test, which is used for nonparametric comparisons. If there were missing values due to participants refusing to wear earmuffs or NC headphones or not encountering disliked auditory stimuli during the assessment period, the data were excluded from the analysis.
Sample size calculations were performed using the G-Power software version 3.1 (
Results
Medians and quartiles of the GAS scores in each period are presented in Figure 1.
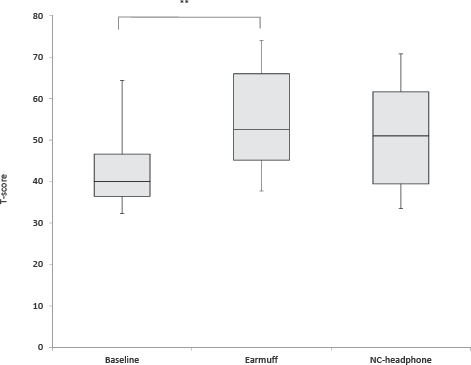
Medians and quartiles of T-scores on the Goal Attainment Scaling in each period. The Wilcoxon rank sum test revealed significant differences between the control period, earmuff period, and noise-cancelling (NC) headphone period. **: p < 0.01.
Four participants (3 boys and 1 girl) refused to wear either the earmuffs or NC headphones. Their mothers reported that their children disliked the tactile impression or pressure. No children wore earmuffs or NC headphones continuously during waking hours. Among the participants who used the earmuffs and NC headphones, the use time per day ranged from 65 minutes to 360 minutes (mean = 136.9 minutes, standard deviation = 69.4 minutes) for earmuffs and from 30 minutes to 360 minutes (mean = 94.6 minutes, standard deviation = 50.6 minutes) for NC headphones according to the parents' and teachers' reports. Three participants (Cases A, K, and M) used them at school only. Five participants (Cases C, F, H, I, and J) used them at home only. Other participants used them both at home and at school.
Table 1 shows the age and sex of each participant, the auditory stimuli that induce behaviour problems, and problem behaviours induced by auditory stimuli in each child, excluding participants who had refused to wear either earmuffs or NC headphones. One to four goals were prepared for each child.
Participant Characteristics, Auditory Stimuli that Induced Behavioural problems, Behaviour after sounds, and Goal Attainment Scaling (GAS) Scores.
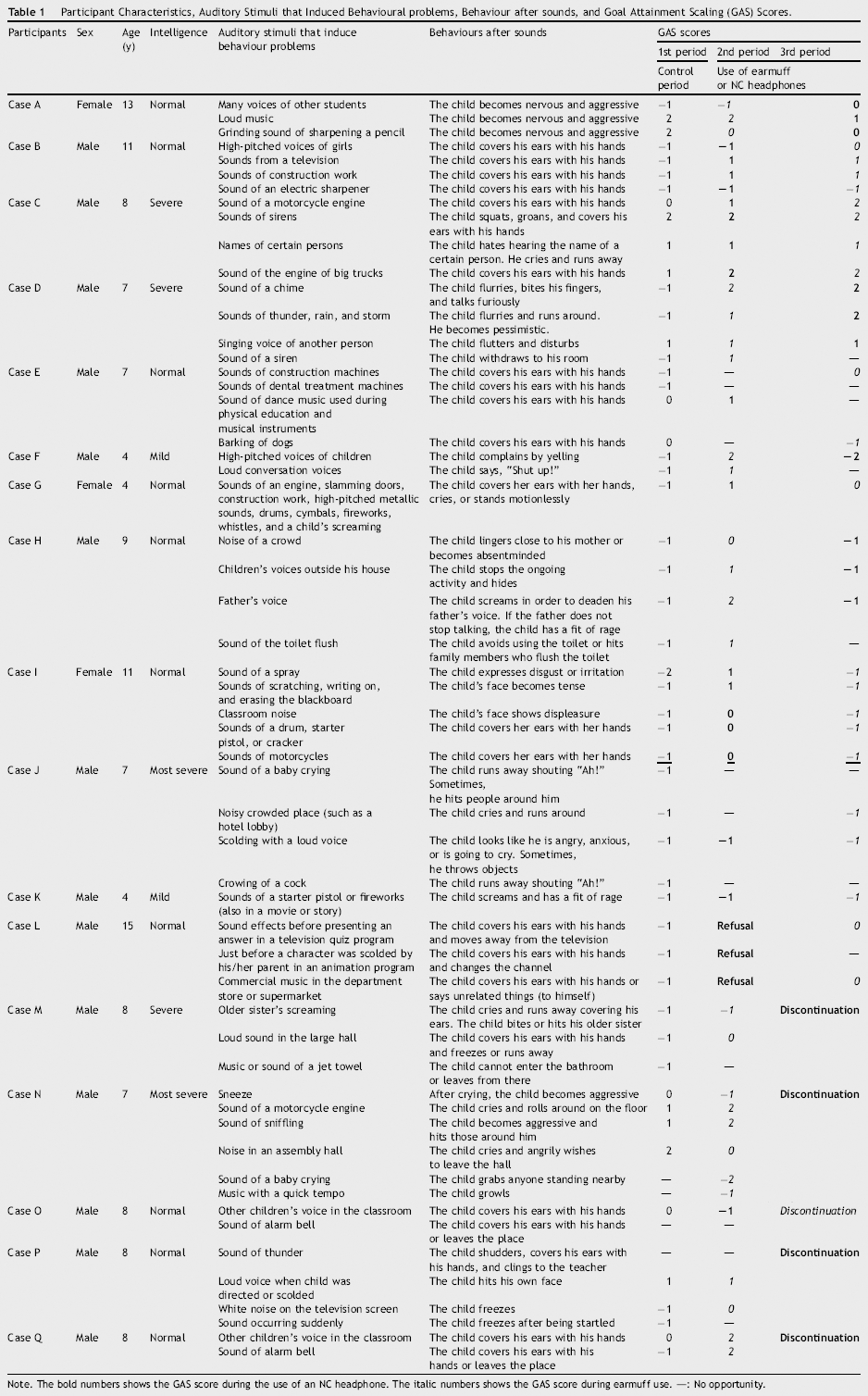
Note. The bold numbers shows the GAS score during the use of an NC headphone. The italic numbers shows the GAS score during earmuff use. —: No opportunity.
One child refused to wear earmuffs because he disliked the pressure they exerted. Five children refused or discontinued to wear NC headphones because they could hear human voices better and disliked other students' voices. As a result, we compared the T-scores between the baseline control and earmuff use period in 16 children with ASD, and between the baseline control and NC headphone period in 12 children with ASD.
Fifty-six behaviours induced by auditory stimuli were evaluated using the GAS. Since most of the participants exhibited some problem behaviours induced by auditory stimuli, the GAS T-score for each participant was calculated from the GAS scores in each period.
The GAS T-score was significantly higher for the earmuff period than that for the control period (Z = 2.726, p = .006). There were no significant differences in the GAS T-scores between the NC headphone period and the control period (Z = 1.689, p = .091) and between the earmuff period and NC headphone period (Z = −0.451, p = .678). Although there were no significant differences between the NC headphone period and control period, the GAS T-scores of five children improved during the NC headphone period.
Parents of participants whose GAS T-scores during the NC headphone period were better than those during the earmuff period reported the following: “He was pleased by the diminished sound of the piano,” “He could tolerate noise from the big trucks,” “He disliked the pressure of the earmuffs, but he tolerated the NC headphones.” Parents of participants whose GAS T-scores were better during the earmuff period than those during the NC headphone period reported the following: “If he wore earmuffs, he could enter the bathroom” (this participant disliked the sound of water flushing), “He could tolerate the noise of the air towel,” “He may have felt stressed when he wore the NC headphones because he could hear human voices clearly when the other noises diminished.”
Discussion
Development of treatment or support for individuals with ASD-AH is an important issue; however, evidence supporting therapies such as auditory integration therapy and sound therapy for children with ASD has not been reported (
Special education directors reported that occupational therapists provide relatively more service in assistive technology consultation (30.3%) and task or environment modification (25.8%) to improve student performance (
To adapt earmuffs and NC headphones for use in children with ASD-AH, treatment evidence is necessary. To date, a few researchers have reported the benefits of earmuffs and earplugs for children with central auditory processing disorders who have difficulty concentrating and processing auditory input in busy environments (
Our results showed improvement of GAS T-scores during earmuff use, therefore, earmuffs can have a positive effect for coping with behavioural problems related to hyperreactivity to auditory sensory stimuli in children with ASD. Since earmuffs reduce auditory stimuli from the environment, they might reduce the stress or anxiety caused by auditory stimuli.
Although an improvement in the GAS T-scores was observed in some participants, there was no effect of NC headphones on behavioural problems related with hyperreactivity to auditory sensory stimuli. The parents of participants whose GAS T-scores during the earmuff period were better than those during the NC headphone period suggested that earmuffs improved hyper-reactivity behaviour to air towels and flushing water. One mother complained that her child felt stressed when he wore NC headphones because he could hear human voices clearly when other noises diminished. Since NC headphones cannot eliminate auditory stimuli except for low frequency noises, human voices and some other sounds might not be reduced. Therefore, NC headphones may not be effective for participants who have auditory sensitivity to human voices. Interestingly, our study found that behaviours of five children with ASD (Cases C, D, E, G, and I) improved during the NC headphone period as compared with those in the baseline control period, and that the intolerable sounds related with the behaviours of these five participants were not voices but were “noisy sounds in the classroom.” Thus, NC headphones might not be effective in coping with behavioural problems caused by human voices. Occupational therapists should consider the specific sounds related to hyper-reactivity when recommending earmuffs or NC headphones to individuals with ASD who exhibit hyperreactivity to auditory stimuli.
This study has some limitations. One of them is the small number of participants. Since four participants refused to wear either earmuffs or NC headphones, and another five refused NC headphones, the behavioural data from the NC headphone period were limited. Further study should be conducted with larger samples. Additionally, we did not examine adverse and long-term effects of earmuff and NC headphone use. Habitual use of sound isolators may actually exacerbate sound sensitivity over time, as suggested in tinnitus patients (
Conclusion
This was a pilot study, and although there were some limitations in this study, the usefulness of earmuffs for children with ASD-AH, even for such a short period of wearing time, was demonstrated. Although the effectiveness of NC headphones was not statistically significant, we concluded that earmuffs that block sound might be useful for children with ASD-AH, and that NC headphones, which reduce ambient sounds, might also be useful for children with ASD-AH who are not affected by human voices.