
Abstract
Objective/Background
The prevalence of depression in women is two times as much as that in men. However, the rehabilitation programme for return to work for patients with depression in Japan mainly focuses on male individuals. Japanese working women usually have the central role in housework in addition to paid work. Therefore, we hypothesized that Japanese working women with depression need a support programme for housework as well as paid work. The purpose of this study was to investigate the stress factors relevant to the existence of depression, in both paid work and housework, among working women.
Methods
This study recruited 35 women with depression and 35 women without depression. We carried out a cross-sectional investigation with two questionnaires having the same structure: The National Institute for Occupational Safety and Health (NIOSH) Generic Job Stress Questionnaire (for paid work) and the NIOSH Generic Housekeeping Labor Stress Questionnaire (for housework). We extracted the stress factors contributing to the existence of depression using logistic regression.
Results
Three stress factors were found–-two in housework, and one in paid work. In housework, variance in workload and underutilization of abilities were associated with the presence of depression. In paid work, interpersonal conflict was an associated factor.
Conclusion
Rehabilitation programmes involving variance in workload and under self-evaluation in housework, and interpersonal conflict in paid work must be adequately addressed to support working women with depression.
Introduction
In Japan, rehabilitation programmes of return to work for patients with depression began to draw attention in the early 2000s (
From another viewpoint, we would like to consider women's labour in terms of housework. In
As for the housework itself, some studies have investigated the relationship between housework and mental health, and developed some models to address the problem, such as the spillover—crossover model (
It is thus necessary to equally take into consideration both paid work and housework to construct an adequate support system for women with depression. Therefore, in this study, we aimed to clarify stress factors relevant to the existence of depression in working women (in both paid work and housework), to find out the possible factors that might be targets for providing support to working women.
Methods
We conducted an investigation using a self-reported questionnaire on the stress factors and depressive states of women engaged in both paid work and housework. We then extracted stress factors strongly related to the presence of depression using logistic regression analyses.
Participants
There were two groups of participants: 35 women with depression and 35 women without depression. We call the former the depression group and the latter the healthy group in this study. All participants were (a) aged from 30 years to 60 years, (b) living in Japan with more than one family member, (c) working for a salary for > 16 hours a week, and (d) doing housework for > 5 hours a week.
In this study, paid work meant all paid jobs including part-time jobs, and housework meant the labour to maintain daily life including care for family members. These definitions were precisely explained to all the participants.
Depression group
Participants with depression were recruited from 15 private psychiatric clinics in Aichi Prefecture, Japan. They were: (a) diagnosed with major depression by the attending psychiatrist based on the Diagnostic and Statistical Manual of Mental Disorders-IV Text Revision (
The CES-D is a self-reported questionnaire with 20 items on a 4-point scale, designed to quantify the level of depressive symptoms during the past week, with a cut-off point of 16 to discriminate the depressive state.
Healthy group
We randomly recruited individuals living in Aichi Prefecture or Tokyo. Individuals with a history of mental disorder or with a score over 16 points on the CES-D Scale were excluded from this group.
All procedures were approved by the Research Ethics Committee of the Graduate School of Medicine, Nagoya University, Nagoya, Japan (Authorization Number 2012–0007), and all the participants provided informed written consent.
Measures
Job stress questionnaire
The self-reported questionnaire about job stress used in this study was the National Institute for Occupational Safety and Health Generic Job Stress Questionnaire (NIOSH GJSQ), Japanese version, which was developed by the NIOSH. The Japanese version of this questionnaire has been evaluated for its reliability and validity (
Housework stress questionnaire
To investigate housework stress and buffers, we used the NIOSH Generic Housekeeping Labor Stress Questionnaire (NIOSH-HK), a self-reported questionnaire about housekeeping. To evaluate stress in the housekeeping activity from the same viewpoint as the NIOSH GJSQ, we established the NIOSH-HK, which was modified from the NIOSH GJSQ. We confirmed the modification of wordings in the NIOSH-HK, which changed the fundamental viewpoint of NIOSH GJSQ in a preliminary investigation of 30 healthy persons. We have carried out some investigations using both NIOSH GJSQ and NIOSH-HK in previous studies (
Our previous studies have shown that the NIOSH-HK has the same structure as the NIOSH GJSQ, but the number of questions in NIOSH-HK was different from those in the NIOSH GJSQ, because we had deleted some questions unrelated to housework in developing the NIOSH-HK.
Properties of the NIOSH GJSQ and NIOSH-HK Questionnaires Used in This Study.
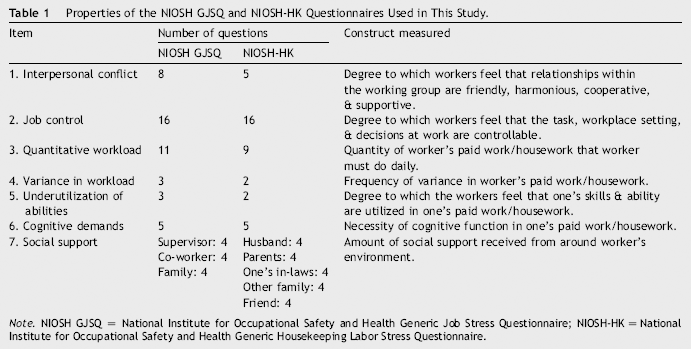
Note. NIOSH GJSQ = National Institute for Occupational Safety and Health Generic Job Stress Questionnaire; NIOSH-HK = National Institute for Occupational Safety and Health Generic Housekeeping Labor Stress Questionnaire.
Statistical analysis
We measured the odds ratio to predict the existence of depression leading from each stress factor and buffer, using forward stepwise logistic regression analyses. The presence or absence of depression (coded as 1 or 0) was set as the dependent variable, while every score of stressor and buffer in the NIOSH and the NIOSH-HK was defined as an independent variable. Variables were analyzed in a multivariate analysis with a logistic regression and forward stepwise selection, and the odds ratio and 95% confidence intervals were calculated for all variables. The Hosmer—Lemeshow goodness-of-fit was used to assess the model fit. Statistical significance was set at p < .05. All analyses were performed using SPSS version 21 for Windows (IBM Corp., Armonk, NY, USA).
Results
Age, Working Hours (Paid Work/Housework), and Scores of CES-D.
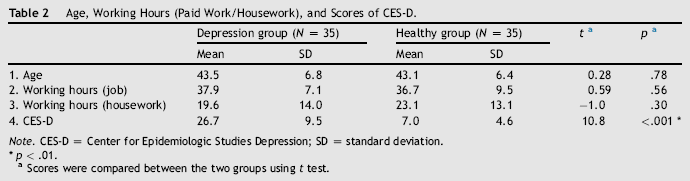
Note. CES-D = Center for Epidemiologic Studies Depression; SD = standard deviation.
p < .01.
Scores were compared between the two groups using t test.
NIOSH GJSQ and NIOSH-HK Scores in the Two Groups.
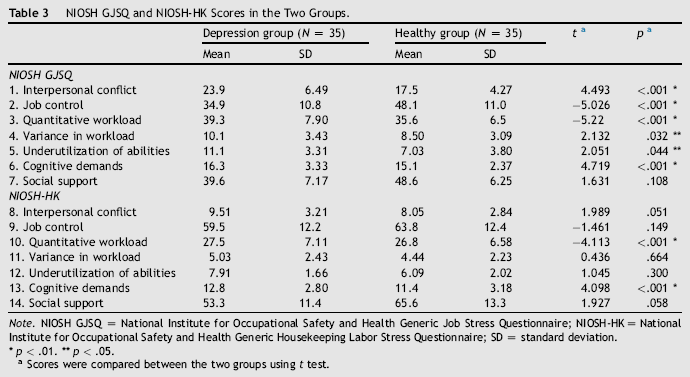
Note. NIOSH GJSQ = National Institute for Occupational Safety and Health Generic Job Stress Questionnaire; NIOSH-HK = National Institute for Occupational Safety and Health Generic Housekeeping Labor Stress Questionnaire; SD = standard deviation.
p < .01.
p < .05.
Scores were compared between the two groups using t test.
Results of Logistic Regression Analyses to Detect the Presence of Depression and Stress Factors in the NIOSH GJSQ and NIOSH-HK Questionnaires.
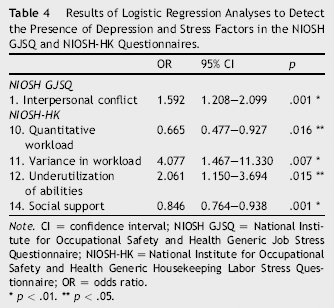
Note. CI = confidence interval; NIOSH GJSQ = National Institute for Occupational Safety and Health Generic Job Stress Questionnaire; NIOSH-HK = National Institute for Occupational Safety and Health Generic Housekeeping Labor Stress Questionnaire; OR = odds ratio.
p < .01.
p < .05.
Logistic regression analyses indicated five factors that significantly contributed to the presence of depression. Among those five factors, the odds ratios of variance in workload and underutilization abilities in the NIOSH-HK, and interpersonal conflict in the NIOSH GJSQ were higher than 1.0. Therefore, we considered these three factors to contribute to the presence of depression, and they have high possibility to become targets of intervention in women with depression.
Discussion
The purpose of this study was to identify stress factors related to the presence of depression, which could eventually be used as targets of intervention in women with depression. The findings from our study indicated that variance in workload, underutilization of abilities in housework, and interpersonal conflict in paid work were significantly related to the presence of depression and had possibilities to be targets of interventions.
“Variance in Workload” in Housework
One factor, variance in workload, involved the following three questions: (a) How often is there a marked increase in your workload? (b) How often is there a marked increase in the amount of concentration required in your housework? (c) How often is there a marked increase in how fast you have to think? That is to say, variance in workload reflected the stress caused not merely by quantitative increase of workload, but by sudden fluctuations of workload caused by some unexpected circumstances in housework.
In paid work, treating depressed persons by reducing or eliminating their workload is said to be crucial, at least during the early stage of depression. In this study, participants had been under treatment for at least 6 months. Therefore, it is highly possible that they had already been relieved from heavy workload in their paid work. Under such circumstances, it was straightforward to assume that they would avoid an abrupt increase in their workload or the outbreak of unanticipated workload in their paid work. Hence, it is convincing that variance in workload in the NIOSH GJSQ was not a significant predictor of depression.
As with paid work, it is common for therapists to try to reduce patients’ house workload during their treatment. For example, therapists encourage family members to share housework with depressed women, or recommend that patients stay in their parent's homes where they might easily obtain the support of their mothers. Nevertheless, for housekeeping, it is not easy to exempt patients from doing that work completely, because the number of family members who can do housework are limited. Patients must cope with housework demands, for example, when a family member suddenly becomes sick, one of the children has an entrance examination, or there is some important ceremony or family occasion. In these cases, fluctuation of burden is common and depends very much on the living conditions of the woman's family at that time. Therefore, despite the effort of therapists to reduce patient's workload, it might still be difficult to change the situation.
Difficulties of this kind can be interpreted from the viewpoint of cognitive functions. Whenever the workload of housekeeping is suddenly changed for some reason, individuals are required to increasingly use their executive function or attention. However, some studies have reported that depression would lead to the decline of basic cognitive functions (
To assist houseworkers who have depression, the quantity of support must change along with fluctuations in housework. Moreover, the support systems are required to be tailor-made according to the patient's situation, and to cope with sudden fluctuations. For example, it may be important to develop systems to offer services such as looking after children or elderly persons temporarily.
“Underutilization of Abilities” in Housekeeping
Regarding this factor, participants were asked if they could use the abilities they had acquired before. Example of questions were How often are you given a chance to do the things you do best?, How often can you use skills from your previous experience and training? From the answer to these questions, it was obvious that women with depression did not have a chance to use their acquired abilities adequately in their housework.
In line with the basic concept of this questionnaire, this result should be interpreted to mean that women with depression experience dissatisfaction in situations in which they cannot make adequate use of their abilities. Therefore, one can imagine that women who tend to be dissatisfied about utilization of their housework abilities might be prone to depression.
However, from the viewpoint of the pathology of depression, this finding might also indicate that women with depression who regard their abilities as less than before tend to feel that they cannot use their real capabilities in housekeeping. That is to say, we should suppose that they answered the questions not from their viewpoint that they underutilized their possible abilities, but from their viewpoint that their abilities had deteriorated in comparison with their past abilities.
The participants in this study had already suffered from depression for over 6 months, and their CES-D scores were over 16, that is, they had considerable depressive symptoms. It is possible that this result reflected the actual picture of the pathology of depression.
One can say that housework consists of responses to the personal needs of individual family members, and that those demands are influenced by family situations. For example, in cooking, a woman is required to prepare meals according to the preferences of her family members within a given budget and a certain amount of time. Therefore, it is difficult to standardize and generalize the abilities required in housework. In addition, women cannot estimate their abilities by comparing themselves with other people because housekeeping is an art usually done alone or with a limited number of family members. For that reason, women tend to subjectively estimate their abilities in housekeeping.
“Interpersonal Conflict” in Paid Work
In paid work, interpersonal conflict has been significantly related to the presence of depression, and this result supports the result of some preceding studies.
In a large-scale survey in 1997, The Ministry of Labour of Japan investigated stress factors among 12,000 employees in the workplace, and reported that for both men (40.6%) and women (56.9%), the highest stress factor was human relations in the workplace (
Today in Japan, support systems in facilitating employees to work are developing gradually through some practices. The guide to reinstatement support of a worker with mental health problems (
The results of our study, however, showed that stress specific to women with depression had more to do with interpersonal conflicts than the workload itself. It was certainly possible that the amount of work in women with depression might have already been managed at the start of this study, because they had already taken temporary leave of absence from their job. However, even in such situations, women with depression might significantly be more stressful due to interpersonal conflict than healthy women. Hence, we should conclude that to support them adequately, it is crucial to prepare some guidelines regarding management of interpersonal conflict in the workplace.
Limitations
There were several limitations in this cross-sectional study. First, we could not determine clearly whether the stress factors investigated were direct causes or results of depression.
The participants of study had been under treatment for some time and had taken leaves of absence or were given reduced working hours because of depression. This implied that they had already received some psychosocial support. Although the amount of support varied for each participant, the support they received must have had some influence over their feedback in the questionnaire survey.
The sample size was not large enough, and this might have been a bias in the results, which suggested low stress factor in work. A future study with a larger sample is therefore suggested.
Footnotes
Acknowledgements
The authors are deeply grateful to all the psychiatrists for their generous assistance with the recruitment of participants. We would also like to offer special thanks to all the participants for providing the data.