
Abstract
The purpose of the introduction of an automated laboratory system in one format or another is reducing the costs of the laboratory by cutting staff. Also speeding up the performance often is a goal. At the same time it is planned to increase the quality of the work done by using automated labelling and reading of documents. The use of vacuum tubes and the handling of these by the apparatus are raising the safety of the labwork.
In this paper many aspects of the daily routines when using a TLA system are discussed. The aspects are collected during the discussions before and after the implementation of the Roche CLAS system in our laboratory. Some consequences were foreseen, and others came unexpectedly. But still the subjects form a point of discussion around the TLA systems. The most important message to be picked up is that one really has to consider all possible problems that could arise from the implementation of TLA.
Keywords
Introduction
Nowadays every laboratory professional considers the introduction of automation of the activities in the laboratory. The reasons for doing this are the many possibilities to implement modern techniques into the laboratory, and the fact that the size of the laboratory isn't really any limit for implementation anymore. Nowadays profit can be reached within every lab using automation of a fitting format.
It must be kept in mind however that the automation of the laboratory is only the automation of a part of the process between the collecting of the blood, urine or any other material and the reporting of the results. In this whole process the most important steps like identifying the patient and labelling the material for the first time cannot be automated. They will take time and are prone to mistakes. Also the transport of the material can be a cause of delay in the process.
The industrial companies can supply automated equipment useful for every laboratory. The question remains whether the automation of the laboratory one way or another is influencing other work to be done in the hospital.
The industrial companies have developed a special linguistic expression to indicate what total lab automation is doing to the laboratory: It is said that the TLA integrates all phases of the laboratory work, meaning that the pre-analytical, the analytical and the post-analytical work are all integrated into one apparatus. But this apparatus also integrates all types of work of the laboratory, like the chemistry, immuno-chemistry, haematology, urinalysis. For one reason or another this integration is called consolidation (Latin: meaning “growing together to one piece, getter stronger”). Since the difference between these two types of integration is rather subtle, people are mixing up these words. I suggest that it is concluded that TLA brings about a two dimensional integration, one dimension being the phases of the labwork, and the other being the types of workspots.
THE DISCUSSION OF THE SUBJECT
Description of automated apparatus
In general the following parts can be recognized in the automated equipment: Computer Controller controlling a moving belt system along which instruments are placed taking care of:
Entrance and/or exit of tubes
Recognition of tube
Recognition of sample
Measuring the colour of the sample
Measuring the size of the sample
Centrifugation
Decapping
Aliquotting
Analytical activities
Production of secondary tubes
Selection of secondary tubes
Storage of tubes
It is not necessary to buy a complete system in one move. It is possible to decide to automate only the front-end (before analysis, pre-analytical) of the laboratory. Or just the sorting of the primary tubes (the tubes obtained at the patient). Or a combination of much labor demanding tests that need speeding up. There is also the possibility to extend the existing system in case of an increase in requests, or introduction of a new analysing machine. Of course, it is wise to consider these possibilities during the process of preparing for ordering an automated system. It is also wise to think about the real reason for acquiring an automated system: if shortening of the time between the collection of blood and the report of the results is the main, and may be the only, reason one should look after the whole process and not look at the work in the laboratory alone.
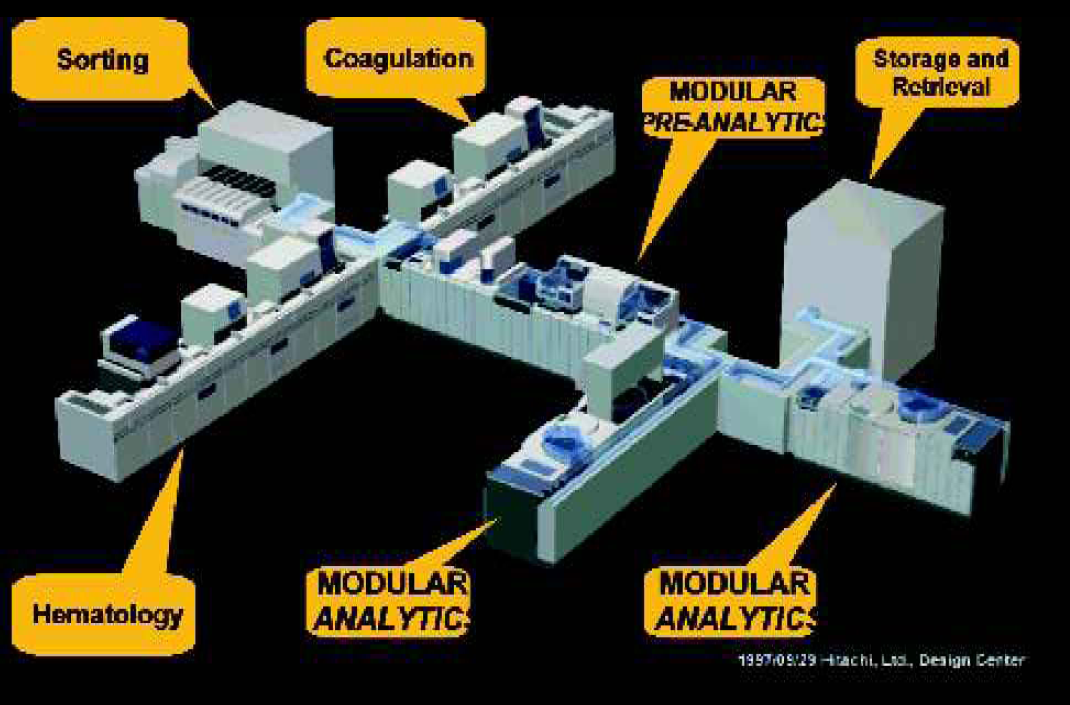
An example of a TLA system integrating laboratory activities.

Example of a pre-analytical module (Olympus) that can be used to sort and decap different sample tubes. This module can be a part of the TLA system Olympus 2500.
Introducing automation into the laboratory is big business. Not only because of the money involved, but also because of the impact the automation will have in the laboratory and the hospital in total, and is expected to have. Most of the time, if not always, the automation is used to stop further increases in labour costs. This is a well-accepted goal to be reached. Indeed lots of the users of TLA report a diminishing of those costs. But besides the planned goals of the lab automation other consequences will be encountered. And it is good to consider those on beforehand.
TOTAL LAB AUTOMATION AND THE STAFF IN THE LABORATORY AND THE HOSPITAL
The technicians in the laboratory are the people who are going to work with the equipment. It is important that they will feel at ease using the instruments. A well-organised instruction is needed before they have to work with the equipment. There is a lot of time needed to get everybody well trained, especially when the TLA is going to be used during nightshifts. It must be remembered however that the best way to learn to handle the instruments is by using them. A good method to instruct the technicians is to start with a small group, which is willing and capable of instructing their colleagues while working with the system.
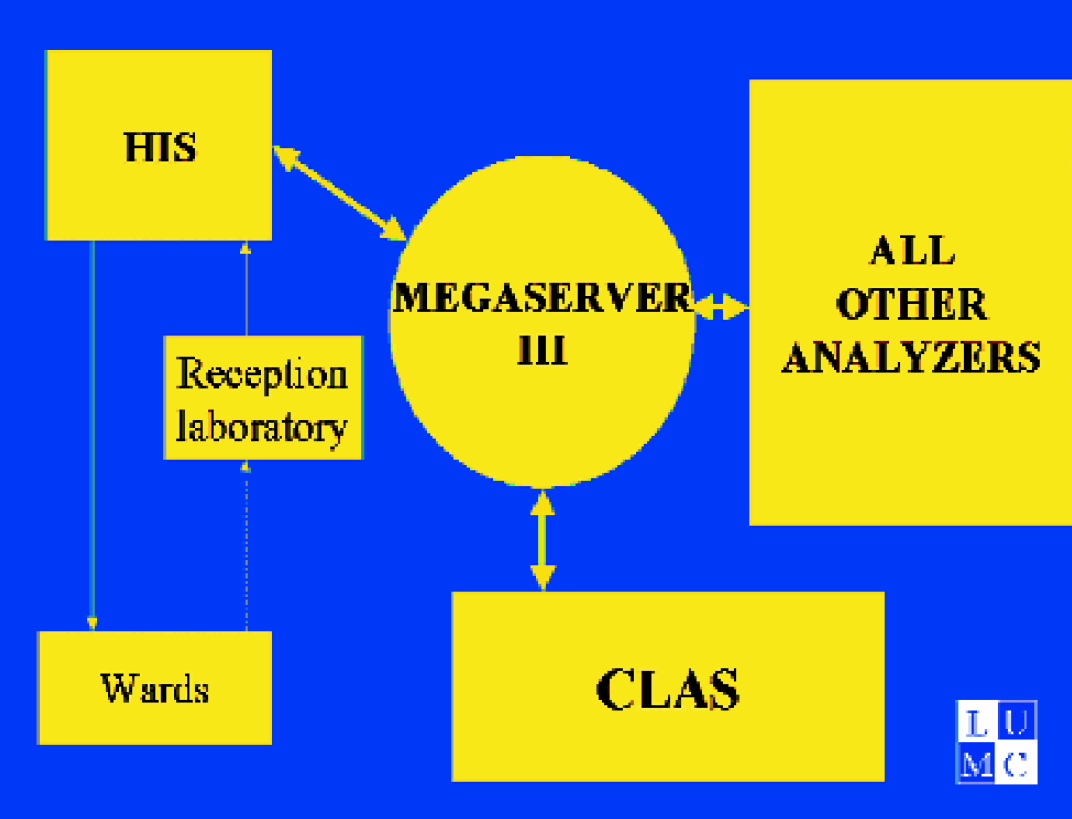
Scheme of the computerconnections using TLA in the Leiden University Medical Center. HIS= Hospital Information System; Megaserver III= server connecting all laboratory equipment to HIS; CLAS= Clinical Laboratory System (Roche, Hitachi). Note a. only one connection between laboratory and hospital system; b. all automated equipment is connected to Megaserver.

Example of a moving belt connection between different components of the CLAS (Leiden University Medical Center).
TOTAL LAB AUTOMATION SYSTEM NEEDS SPACE
Automation of the laboratory needs space. Depending on the size of the equipment, room must be reserved and prepared before the instrument can be placed. Most of the time the equipment, once installed, cannot be moved again easily. So it is wise to inspect the floor before, and to repair the worn out parts. There is also the tubing for water supply, and for air, and electricity. The cables and tubes form together a very big bundle of unwanted material on the floor, so a good solution to hide these from sight and pathways will be necessary. Some companies provide cable containers connected and built in the apparatus, and LabLink has the speciality to offer cable gutters above the apparatus. The Thermo Clinical labsystems (Finland) moving belt system has an architecture making it possible to install the total system in a very short time. Also changes can easily be made. This is accomplished by the installation of parts of the moving belt-track on the backside of the module. The weights of the module secure the moving belt, and the outlining is rather simple to perform.
COMPUTER CONNECTIONS
The automated equipment has its own computer system, the Controller. This system controls the apparatus and signals to the operator the functioning of the system. This computer must be connected to the information system of the laboratory (LIS) or the information system of the hospital (HIS). It must be kept in mind that the software of the controller has to be easily understandable for the technicians in the laboratory. The software is the connection of the system with the operators.
INTRODUCTION OF PATIENT DATA
Automation of the laboratory starts with the automated introduction of patient data and requests from the LIS or HIS into the Controller. In some situations the physician will be introducing the data directly via a PC into the HIS or LIS. Mostly, however, the data introduction of the requests from a paper form into LIS or HIS will be done using forms with Optical Mark Reading OMR, or Optical Character Reading OCR, or barcode readings, or combinations of these techniques. Of course the transfer of request data can be done manually, but this is a lot of work and a source of mistakes. At this moment the possibilities of the 2-dimensional barcodes are in full development, OMR can be very well combined with barcode readings. However OCR technique is not capable of reading all handwritings, and using this technique will cause frequent correction of the readings to be necessary. Whatever the method that will be chosen it is very important that the requests can be introduced into the Controller very quickly. The sample and the form belonging together must have been labelled with the same barcode number.

Illustration of the kind of tubes in use in the hospital
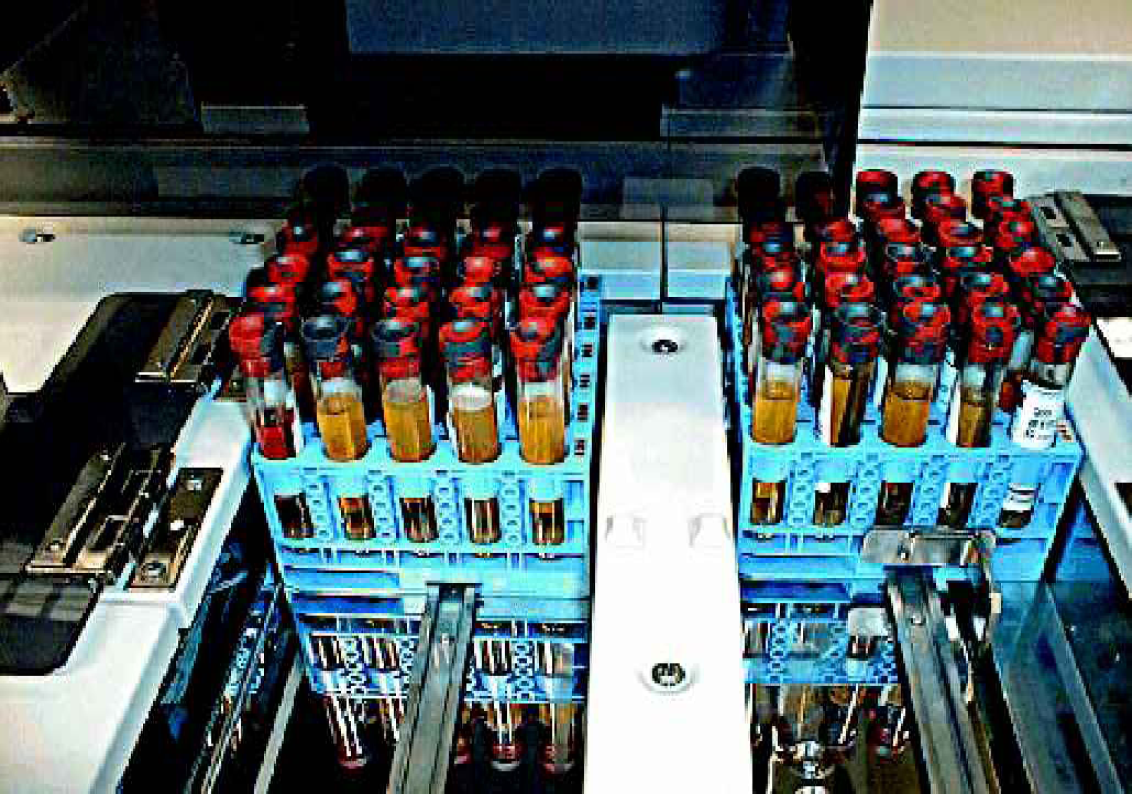
The Roche-Hitachi 5 sample Racks as they are in use in the Roche-Hitachi automated systems.
LAB AUTOMATION AND THE MOVING BELT
Looking at the construction of the lab automation systems some aspects are very different between the products delivered. Most eye-catching is the presence of a moving transport belt transporting the samples along the different components of the system. The presence of this belt can make the control of a big well-functioning automated system really a one-person job. If the belt is not present, staff are needed to bring the samples from one instrument to the other. Of course, this is not a difficult job, but it can really save time when the transport is automated since the belt is always there to move things when necessary and possible. The belt can also be used to transport samples during an automated reflex testing procedure, or after a dilution of the sample. Sometimes the costs of the belt can be a problem, or people are argue that the belt is a weaker component.
The belt in the Bayer Advia systems transports the samples round in a circle line. When an analyser is ready to handle requests the tube is picked up from the belt while passing by. Another layout is that the sample is moved from the entrance to the storage of treated samples. And, when necessary, the sample can automatically be picked up from the storage and be analysed again. The belt layout and possibilities like picking up the samples determine strongly the efficiency of the sample handling in the laboratory. Each feature however will generate extra costs, like extension of the belt and fitting of the software.
THE USE OF TLA IN NIGHTSHIFTS
During nightshifts the number of samples, again depending on the local situation, probably will diminish strongly. The question is whether it is efficient to keep the “big system” running for that small amount of samples? Or should a small STAT-laboratory be kept available? The advantages of keeping the TLA system in the air is that the staff of the laboratory can perform all tests available on the system also during the nightshifts without much a-do. There will be no, or only a small amount of tests left over for the morning group. Everything is finished during the nightshift, and without extra staff! A minor, but not unimportant point, is that the staff working at nightshifts will get used to working with the system. The fear that the bigger system would have a break down during the night shift, should be answered by giving good and extensive instruction to the technicians of the nightshifts. The change of meeting problems is in no way bigger on the TLA than at the smaller equipment.

Tube carrier with sample tube in the Thermo Clinical labsystems. The white block in which the tube is placed contains an embedded microchip (Radio Frequency-tag).
THE SAMPLES TUBES
Sample tubes are the one and only connection between the laboratory and the patient. So demands on the size of the tube, or handling of the tubes will have consequences for the patients: Decisions about the type of tube, presence of gel, handling of small samples, making one, more or none secondary tubes are related to the use of the tube by the system. On the other hand to moments of blood collections in the hospital and the moments of arrival of the tubes in the lab have a strong influence on the use of the TLA system.
The samples are collected from the patients. Of course the collector has to identify the patient and has to be sure that the sample taken is correctly labelled. The blood collection is almost the only spot in the automated analytical process where mixing up can occur. The other moment of a possible mixing-up of samples is the moment when the patient ID put on the tube by the nursing staff, is going to be replaced by the sample number used by the laboratory. Sticking barcode labels on the tubes does identify the tubes. These can be one or two-dimensional barcodes. The latter are capable of containing much more information than the one-dimensional labels. Furthermore the two dimensional label can be smaller, and is less sensitive for damage.
The label on the tube must correlate with the information fed into the LIS or HIS while introducing the data of the request.
THE ARRIVAL OF TUBES INTO THE LABORATORY
An important point to be considered is the effect of peaks in the arrival of tubes into the laboratory. Depending on the organization of the hospital and laboratory it can be expected that either all tubes will arrive at a certain moment in the lab; or, that during the day the samples will arrive nicely spread out over all working hours without causing a rush-hour peak in the lab. It is important to consider this point before one implements the TLA. If the system cannot cooperate with the local situation, it could be that this situation has to be reconsidered and changed, or that a different TLA-system must be chosen.
ENTRANCE OF TUBES
Before the tubes can be entered into the automated system the Controller must be fed with the data of the request. This means that at least the sample number on the tube and the tests to be performed must have been introduced into the controller. The tubes are placed in the containers of the system, so called racks. This can be a container for one tube or a rack for more tubes, mostly five tubes (Roche, Abbott). Of the single tube container several models exist. There is the model of LabInterlink. In it all sizes of tubes will fit and the route of the tubes through the system is determined by the information from the sample number on the tube. So several times during the passage of the tubes the bar code has to be read. Also the Coulter system uses a single tube container but of a slightly different size. Again all kinds of tubes will fit, and again the bar code on the tube is essential to steer the tube through the system. Another approach to single tube containers is that of Thermo Clinical Labsystems. This company uses a container fitted with a disk containing the routing information of the tube placed in the container. The barcode on the tube is used at the analysers for knowing what tests have to be done. Again this container can use all kinds of tubes. In this system the covers of the track are tightly screwed on so it is almost impossible to remove the tube from the container uncontrolled by the system. The five-tube rack developed by Roche and by Abbott fits into all their systems. So it is easy to bring the racks from one apparatus to another. With Roche the information about the tests to be performed is connected to the place of the tube in a specific rack. The automated system will recognize the tube from the number of the rack and the position of the tube in the rack. The system will read the sample number once and relate that sample number to the rack number and the place in the rack. This is very convenient when secondary tubes are made by the system. The secondary tubes have to get a label fixed on them, and during a certain amount of time when the label is not fixed yet, the system will recognize the tube from the number of the rack and the position of the tube. If the printing of secondary labels is interrupted by machine failure the rack containing the secondary tubes can be removed from the system, and after the problem has been solved the system will recognize the rack and the still unlabeled tubes in it. The labels will produced then and put on the tubes. When no rack is used the only recognition of the tubes is the barcode fixed on the tube. Unlabeled tubes cannot be handled by the system.

Example of an aliquotermodule. This module takes secondary samples from primary tubes in a TLA system. (Thermo Clinical Labsystems, Kone, Finland).
STAT-TESTS
Sometimes it is argued that the use of racks diminishes the possibilities of the system to speed up when one of the tubes is a Stat test. However, most systems have the possibility to enter the stat sample into the system with a priority mode offering the rack and sample the fastest way to move through the system. The possibilities of the layout of the track system to offer bypasses are more important than the use of a single tube container, or a multitube rack. Here the influence of the staff is important: if the system does not organize priority for a sample by itself, but the system offer the possibility to enter a STAT sample in a different faster way into the system, the staff should use that possibility to obtain the highest speed.
SMALL SAMPLES, PAEDIATRIC SAMPLES
An important feature of modern analysers is the capability to handle very small samples. Tests can be performed using less than five microliters per test. This is quite a difference with the automated equipment of former days when the sample volume could easily go up to 1 mL. It would be a shame when “the small sample feature” would be lost because of using totally automated equipment. Therefore several solutions have come up to solve this problem. Most of the systems can handle put-on small containers placed on, or inside, the regular tubes. Sometimes care must be taken to by-pass a decapper. The pick-up systems on the analysers will recognize the put-on sample by the level-sensing device, or by information from the Controller. However, the introduction of the small samples into a system will take extra time and care by the laboratory staff. It must be a point of consideration when thinking about acquiring an automated system, but certainly it must not be considered as a negative item.
THE USE OF PLASTIC GEL CONTAINING TUBES
The automated systems are handling the tubes by lifting them, centrifuging them, and moving them along the track to the apparatus connected. Sometimes the forces used on the tubes can be rather strong and to prevent damage to the system because of damaged tubes the use of plastic tubes is advised.
The analysers will take a sample from the tubes. Some sample taking systems will follow the level of the material in the tube downwards while sucking up the material. To prevent the clot to be sucked up precautions are taken by the system: the size of the available sample is estimated and compared with the sample to be taken. For this purpose the tube has to be recognized by the system and after centrifugation the upper and lower level of the sample in the tube have to be sensed. From these data the size of the available material can be estimated. It is recommended to use gel-containing tubes to obtain a flat surface after centrifugation. The use of gel containing tubes offers the possibility to speed up the braking rate of the centrifuge. However when plasma tubes are used, and if the braking rate of the centrifuge is not especially raised, there is no necessity to use the gel containing tubes. The disadvantage of using gel-containing tubes is that some drugs are extracted from the serum and absorbed in the gel during centrifugation. So, to be able to measure drugs it should be ordered not to use gel-containing tubes, and one has to take an extra sample from the patient. This was not the intention of the introduction of the automated system. And it must be a point of consideration. If the TLA is not equipped with this feature, level sensing will be used and the risk of sucking up some clotting material is there. But by using gel-containing tubes the sample taking system will stop its action as soon as the gel is felt. It is said that the gel protects the serum/plasma of contamination by the contents of the clot underneath the gel. We found out however that the gel is protecting for a short period of time, about two days. After that a raise in the potassium and LDH content is seen above the gel layer. If one wants to store material for later tests a secondary sample should be taken from the serum/plasma, and that can be stored.
CENTRIFUGATION
A TLA system will contain an automated centrifuge system. Sometimes it is questioned whether this device is useful and cost worthy. It is a typical example of making the system independent of the staff of the laboratory. Without having the intention of insulting the lab workers it is beyond doubt that the centrifugation step by the system will run faster than when handled by the staff: the system is not distracted by other activities. This is especially true when it is the intention to let the TLA be served by the smallest amount of people possible: one person. The centrifuges mostly handle 60 samples per run, while a run takes about 10 minutes inclusive loading and unloading.
THE DECAPPING AND RECAPPING OF THE TUBES
In some machines the tubes will be opened to collect a sample of material; in others the tubes must be opened on forehand. And for the haematological tests the needle of the instrument will pierce the caps. It is one of the main features of an automated system to minimize the handling of the tube by the staff of the laboratory in order to raise the safety. There are different ways the tubes are stoppered by the different manufacturers: a rubber stopper can be pushed on the tube; or a rubber stopper covered by a plastic cap can be fixed on the tube using a screw inside the cap; and a thin metallic lid with a piece of rubber in the middle can be fixed on the tube. All these different stoppers appear in different sizes and on different heights in the total labautomation system. The decapper is the device that has to handle these. Today's decappers get more and more sophisticated in handling all sizes of tubes and stoppers. Just before the decapper the size of the tube is measured and the result is transported to the decapper. And the action of the decappers doesn't have to be a reason for a change or adaptation of the choices of tubes. As long as the tubes are of a well-recognized size and the stopper and cap are of a well-recognized type the decappers will be able to handle them. In most systems the stopper will be removed in smoothly turning motion. It is important to realize that the decapping process should be performed smoothly. A sudden removal of the stopper will produce a shockwave of air into the tube, resulting in a splashing around of the material from the tube. This, of course is an unwanted situation. One should keep in mind that the air in side the space of the decappers is contaminated with aerosols from all tubes that have passed. So, if this contamination could be influencing the result of the test to be performed this test-tube should by-pass the decapper, or should not be opened. The tube can be sorted to be taken out of the system. After the decapper all tubes are open and the tracks should be covered to minimise contamination of the surrounding laboratory air. The analysers will take samples from the tubes, and after the analysing step is done it must be decided what to do with the samples. The primary samples without gel layer cannot be stored because there is no protection of the serum/plasma from the contents of the clot. After a short while the samples cannot be used. The primary tubes containing a gel layer can be stored for a few days before the gel layer is starting to leak.
SECONDARY TUBES AND ALIQUOTING THE SAMPLES
Before ordering and installing the TLA system it should be considered whether there would be need for the production of secondary samples by the system. If there is a tradition in the hospital to “divide at the patient side” meaning that there are taken from the patient as many tubes as different work spots that are needed to perform all requested tests, an aliquoter seems to be unnecessary. However, one could consider breaking with this tradition unless a severe reason is inhibiting this. For the patient comfort it is best to collect a minimal amount of blood. And to try to use this blood as intensively as possible. Of course for the laboratory it seems easy and cheap not to consider aliquoting. The question is whether this is true. Suppose that from each patient there are taken samples for haematology, chemistry, immunoassays, allergy, manual techniques and spare sample. The last five techniques need all the same material: plasma or serum. The consequence will be that without aliquoting the primary tube the staff of the lab will have to handle 6/2 times more tubes accurately than when an aliquoting system is used. All those tubes have to get the correct label and have to be sorted. When an aliquoting system is used from the fewer primary tubes, secondary tubes will be produced by the system. The secondary tubes will be labelled and sorted by the system without change on mixing up of the samples.
ANALYSING THE SAMPLE
In general all available analysers can be connected to each other in a TLA system. Of course, it will be easier to connect analysers of the same brand as the TLA system to the moving belt system, and the controlling computer. But, no vendor will say that it is impossible to connect specific analysers to his TLA. However, it can be very costly to get some types of analysers connected to a moving belt system. Abbott, not selling a moving belt system, puts analysers together to form a big analyser.
TRACKING AND LOGGING THE SAMPLE DURING AND AFTER THE ANALYSERS
When a sample has been introduced into an automated system the technicians often have a problem wanting to know how long the completion of the analysis still will take. Or they want to take an aliquot of the sample in the system because they need that at another location, or need it suddenly in case of STAT requirements. And most of the time, of course the sample in the system cannot be reached, and the time to completion is unknown. The newly developed software for the system of Thermo Clinical Lab automation-system answers the question about the time needed towards the completion of the analysis. Also the movements of the system are logged in detail, so every sample is traced to find what has happened at what time. And of course this logging can be printed. This information will provide an important part of the quality control to be used on the system. Abbott has solved the problem of the “unreachable sample during analysis” by a construction of the sample racks on the outside of the analysers (Architect series) and the software indicating that the requested sample can be taken out of the rack.
STORAGE OF SAMPLES: THE SPARE SAMPLE, LEFT OVER
As discussed earlier a spare sample cannot be the left over of the primary tube because of the presence of the clot in the tube. It is unthinkable that decanting of the primary tube could be a fine way to obtain a spare sample. Therefore the automated system should take an aliquot from the primary tube to produce a secondary tube as the spare sample. Of course it is of the utmost importance that the location of the spare sample is very well known. It must be easy to find the specific spare sample between all the other spares. The automated storage module of TLA is rather costly. But, it could be because of the frequency of using it, that the investment is worthwhile. Nevertheless, the storage of the secondary tubes should be well organized. And in the software of the system a feature should be present to be able to register and find the location of the spare tubes.
EVALUATION OF THE RESULTS
Without any doubt it is necessary to evaluate the results produced from an automated system. The risk is high that the results reach the physician automatically without any technician having had a look at them. In the laboratory protocol it must be one of the important tasks of the technician to look after the results and to make certain that the controls were satisfying, and to make sure that the combination of the results of the requested tests fit to each other. In the case of finding results passing the limits set on forehand, the sample has to bee handled according to an existing protocol to ensure the correctness of the results. There are some evaluation software programs that automatically perform probability estimations on the results (e.g. VALAB).
Conclusion
Implementation of a system of Total Lab Automation is a very big step for a laboratory. The consequences have to be considered extremely well to prevent unpleasant and costly measures to be taken afterwards. There is a great variety of possibilities while implementing a Total Lab Automation system. The right choice is depending clearly on local circumstances.