
Abstract
C-Reactive protein assays with low end accuracy and reproducibility allow for use in risk stratification. We describe the K-ASSAY CRP-2 (Kamiya Biochemical Company, Seattle, WA) on the Roche Cobas Mira (Roche Diagnostics, Indianapolis, IN). Using an immunoturbidimetric principle, turbidity is compared to a stored calibration curve. Calibration stability is at least four weeks. Serum, EDTA-plasma and heparin-plasma provide comparable results. Intra- and inter-assay CV's are <2.55%. The regression equation against hs-CRP calibrators (Dade Behring, Deerfield, IL) is y = 1.11(x) − 0.18; r = 0.999. Quintiles from volunteer blood donors are provided.
Keywords
INTRODUCTION:
C-reactive protein (CRP) is a roughly 130 kd glycoprotein produced by the liver, which is a nonspecific but sensitive marker for inflammation, infection, and tissue damage, hence its designation as an acute phase reactant. 1 It has been largely used in the setting of infection/inflammation, such as an aid in the setting of possible appendicitis and more recently neonatal infections. 2 As the concept of inflammation playing a role in the initiation and progression of an atherosclerotic plaque became accepted, researchers turned their attention to the acute phase reactants as possible markers of atherosclerosis. 3 –5 Using standard assays for CRP, levels were previously shown to be elevated in acute myocardial ischemia or myocardial infarction (MI), and found to predict recurrent ischemia in patients with unstable angina. 3 These standard assays were unable to identify those patients at risk for MI (those with coronary artery disease) as they lacked sufficient low-end sensitivity. This prompted the development of assays capable of accurate measurement of CRP with concentrations as low as 0.05 mg/L. These are referred to as high sensitive (hs) or ultra sensitive (us) CRP assays, similar to third generation TSH assays. As these assays became available, the value of CRP as a risk marker in cardiovascular disease has been recognized, discussed, and generally accepted. 3 –6 As anti-CRP antibodies and a well-established World Health Organization (WHO) CRP reference standard are available, a wide variety of assays for high/ultra sensitive CRP have been released, some of which are adaptable to different platforms. 5 We describe the performance characteristics of such a commercially available hs-CRP kit (K-ASSAY CRP-2; Kamiya Biochemical Company) using the Roche Cobas Mira (Roche Diagnostics) automated analyzer.
MATERIALS AND METHODS:
The Roche Cobas Mira is operated according to the manufacturer's recommendations.
With the Kamiya hs-CRP kit, latex particles coated with antibody specific to human CRP aggregate in the presence of CRP in the sample forming immune complexes. The immune complexes cause an increase in light scattering, which is proportional to the concentration of CRP in the sample. The light scattering is measured by reading turbidity at 550 nm. The sample CRP concentration is determined versus dilutions of a CRP standard of known concentration. Instrument parameters for the hs-CRP assay are as noted in Figure 1.
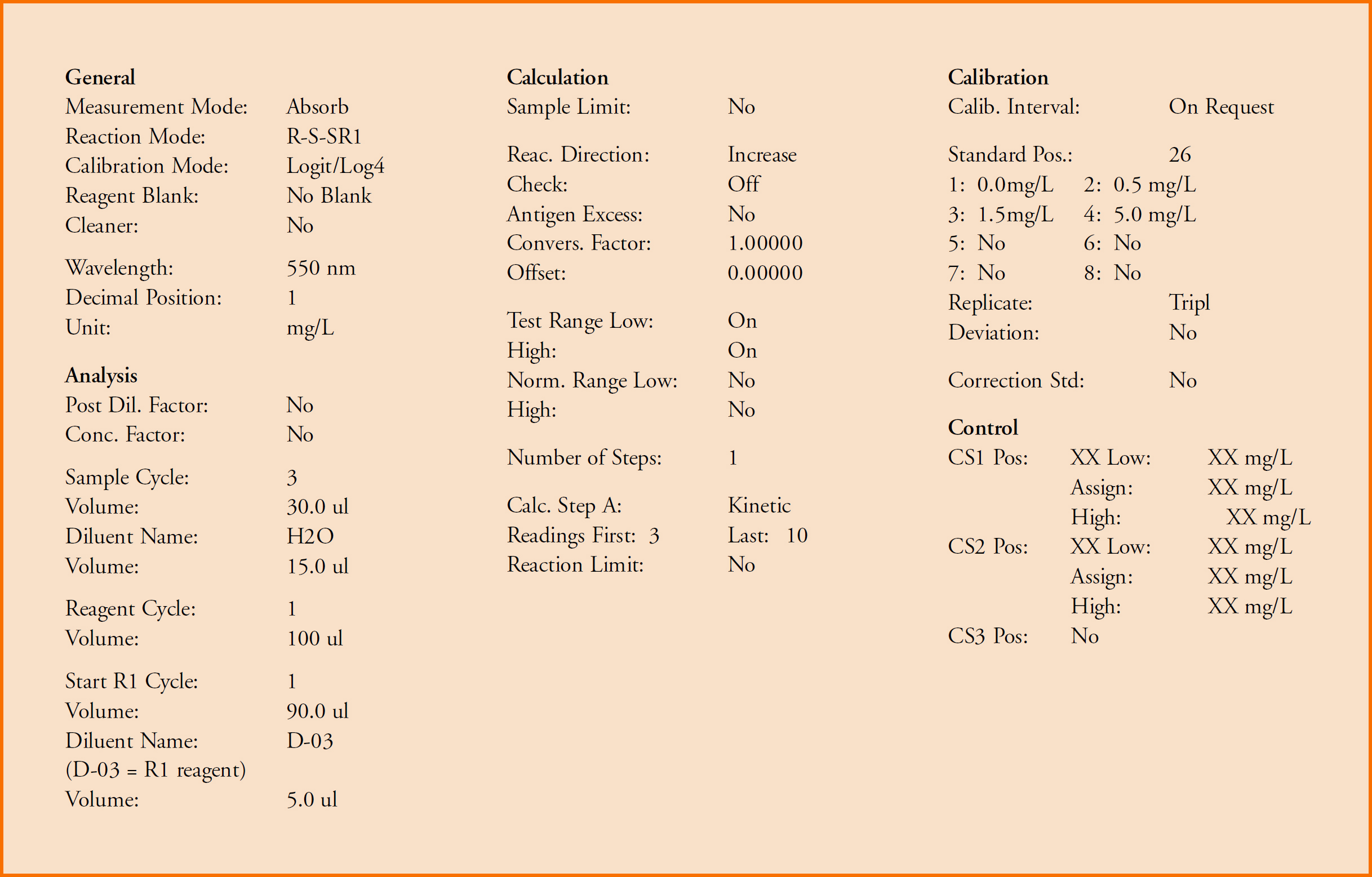
Hs-CRP Parameters on the Roche Cobas Mira
Forty-two paired serum, EDTA-plasma, and lithium heparin-plasma samples were collected from blood donors to see if anticoagulant type influenced results. Two levels of quality control material were used to evaluate inter-assay and intra-assay imprecision. For intra-assay imprecision, both levels were run 20 times. For inter-assay imprecision, each level was run 10 times for five consecutive workdays. Comparison was made with another method (Dade) by running commercially available hs-CRP calibrators as patients and comparing obtained results with the stated values. Blood samples (collected in Lavender EDTA tubes) were collected from 143 donors at a regional blood bank with hs-CRP values measured. Results were divided into quintiles.
RESULTS:
Using calibrators supplied with the test kit, linearity was confirmed from the lowest calibrator (0.5 mg/L) through the highest calibrator (7.0 mg/L). It should be noted that this might vary from kit to kit. The instrument held linearity during an entire four-week period at which time we elected to recalibrate. To allow comparison with another published and established method, commercially available Dade hs-CRP calibrators (Dade Behring, Deerfield, IL) were assayed as patients. These calibrators represented a range of 0.7 to 4.1 mg/L. A regression equation of y = 1.11(x) − 0.18; r = 0.999 was generated with these results. The method also demonstrated excellent reproducibility both within run and day-to-day. The within run imprecision was <0.10% for the low control and 2.14 % for the high control. Inter-assay imprecision was <0.10% and 2.55% for the same controls. There was no statistical difference in results obtained from serum, EDTA-plasma and lithium heparin plasma. (p=0.981) This allows for greater flexibility when it comes to samples and specimen collection. EDTA-plasma is our preferred sample as this is the primary sample for most of our testing. After measurement of hs-CRP in 143 volunteer blood donors (EDTA-plasma) results were divided into quintiles. The upper value for each quintile (listed from high to low) was 4.6, 2.1, 1.3, 0.6, and 0.3 mg/L. These are comparable to results previously published.
DISCUSSION:
With the recognition that inflammation plays a role in atherosclerosis came the realization that markers of inflammation can also be markers of atherosclerosis. Assays were then developed that were capable of measuring these markers with functional sensitivities that allowed for risk stratification. No longer was it sufficient to identify a patient with increased risk, but now one could apply labels such as “low to high risk” 6 or even “1.0 to 2.9 times the relative or standard risk,” 3 depending on the study design reviewed.
In the Physician Health Study, hs-CRP was shown to have predictive value for stroke, first myocardial infarction, and peripheral vascular disease among individuals without other major cardiovascular risk factors. Importantly, the use of aspirin, an anti-inflammatory agent, was shown to significantly reduce the risk of first myocardial infarction. Those with the higher baseline levels of hs-CRP derived the most benefit. 3
The availability of anti-CRP antibodies and a well-established WHO CRP reference standard has allowed for numerous methods to be marketed for the measurement of CRP. Todays analyzers are capable of operating with the precision required to yield functional sensitivities that are low enough for meaningful risk stratification. We have shown that the combination of the Kamiya hs-CRP kit and the Roche Cobas Mira results in a robust assay system with high intra-assay and inter-assay precision. Analysis may be performed on serum, EDTA-plasma or lithium heparin-plasma. This combination has more than satisfactorily been performed on over 150 samples during the past 14 months.