
Abstract
Demographic research generally highlights growing elderly populations as a drain on pensions, healthcare and caregivers. This negative point of view reflects a society which has yet to recognise the potential of the situation and adapt. Alongside ongoing efforts to increase lifespan and improve life quality, society and individuals must work to realise the opportunities rather than the perils of demographic change. Specifically, this article advocates care and rehabilitation of the elderly, enabling them to lead independent lives and to be active in society.
Introduction
We live in an ageing world. Never before in Europe, or throughout the entire world, have so many people been able to live to such an advanced age. The enormous extension of the average lifespan is a direct result of progress in modern medicine and improvement in socio-economic living conditions. It is also influenced by lifestyle choices including nutrition, physical and mental activities and so on.
It is important not only to add years to life, but also to add life to years. Our life expectancy depends on our lifestyle. Life expectancy does not only mean length of life, but also quality of life. It takes into account not only how old one will grow, but also the manner in which one will grow old.
Ageing in Europe takes place differently in each country, and even within each region of a country. Ageing itself is not only a biological process, it is a process determined by a variety of biological, social and ecological factors. There are differences between people of the same chronological age within the same country.
Ageing has many faces: there is the competent and wise senior who is able to manage his or her own life, who is integrated into society and who enjoys a relatively high standard of living on the one hand; and there is the ill, helpless and dependent senior who needs help and support on the other hand. This means that chronological age is a very problematic criterion upon which to base political measures.
Scientists of all disciplines and faculties, as well as politicians, should discuss the issues surrounding longevity in conjunction with the notion of psycho-physical well-being. What can be done to assure healthy and competent ageing? What can be done to assure quality of life in old age? What can be done to prevent illness, diseases and dependency in old age?
The demographic shift
The demographic shift is caused by an increase in life expectancy and a decrease in birthrates: Europe is turning grey in the twenty-first century. The demographic trends in population change and their consequences will be discussed below under five aspects.
The rise of individual life expectancy (individual ageing)
The life expectancy of newborns in Europe is among the highest in the world: 74.9 years for males and 81.2 years for females. In Spain these numbers are higher: 75.5 for male and 82.7 for female newborns (together with France, Spain has the highest expectancy rates in European Union countries). In Germany, life expectancy for newborns is lower: 74.7 years for males and only 80.7 for females [2]. The difference between male and female life expectancy in other European countries ranges from 7.5 years in France and 7.3 years in Spain to only 3.6 years in Iceland (in Germany, 6 years). However, a 65-year-old woman may expect 20 more years and a 65-year-old man 16.1 years (in Germany, 19.2 more years for women and 15.5 more for men).
In most European countries, a 60-year-old person can expect to live for 20-23 more years. This means that after retirement, a person will have about 20-25 more years–-one-fourth of his or her life! Many people today are not prepared for such a long period in a post-occupational–-and post-parental–-stage.
In Germany, the period of youth or adolescence is also prolonged: until age 35 one is considered a ‘youth’, but at 45 one is a ‘mature worker’, and when one becomes unemployed at age 50 one is ‘too old’ to get a new job. Thus Germans are spending nearly half of their lives as ‘senior citizens’.
Collective ageing: the greying society
One hundred years ago the percentage of people 60 years and older in Germany was 5%, in 1950 it was 14% and today it is 23.2%. In 2025 it will be 33.2% and in 2050 it will reach 38.1%. In Spain, there has been a greater increase in the percentage of the elderly: in 1950 only 10.9% of the population was 60 years and over, in 1975 it was 14%, in 2000 it was 21.8%; in 2025 Spain can expect 31.4% of its population to be 60 and over, and the projection for 2050 is 44.1%, much higher than in any other European state (in Germany, 38.1%; Italy, 42.3%; Austria, 41%; Switzerland, 38.9%; and France, only 32.7%) (Fig. 1).
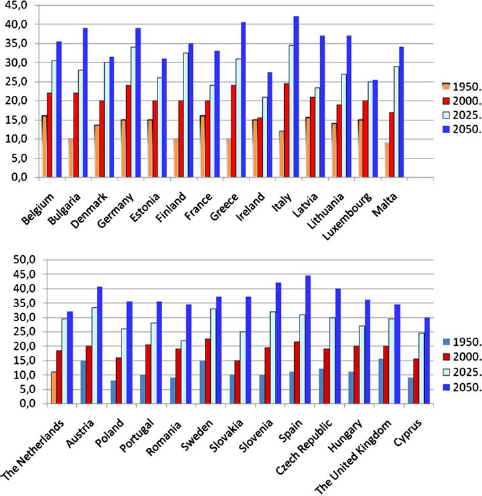
Percentage of people 60 and older (UN 2002)
Population figures for Europe in 1995/1996 showed that 15.5% were older than 65. In 2000 this age group in Germany constituted 16.4%; in Spain, 17%; in Italy, 18.1%; and in France 16% (UN 2002). The lowest proportion was in Finland, with only 10.3%; in Iceland it was 11.3% and in Ireland, 11.5%. These countries have higher birth rates. However, in all European countries the demographic profile has developed from a pyramid into a mushroom.
We also have an increase in the group of 80-, 90- and 100-year-old people. Today, only 3.6% of the population in Germany and 3.9% in Spain are 80 years and older, but in 2050 it will be 13.2% in Germany, and 13.4% in Spain will be 80 years and older (see Fig. 2).
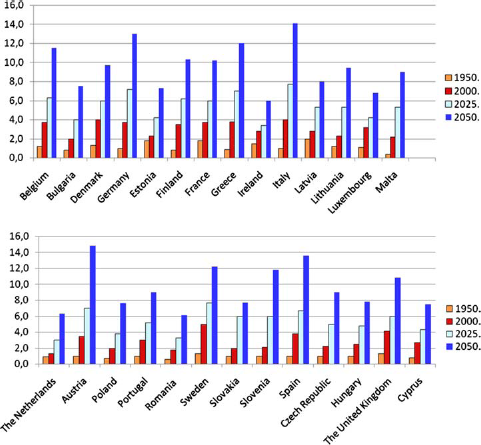
Percentage of people 80 and older
We also have an increase in the group of centenarians: 40 years ago there were only 265 centenarians in Germany, while by 2000 there were 7,200. In 2025 we can expect 44,200 centenarians in Germany, and in 2050 around 114,700 (out of a total population today of 82 million, and about 70 million in 2050). In Spain today there are only 5,000 centenarians, but this will increase to 8,800 centenarians by the year 2025 and to 33,700 centenarians in 2050 (out of a total population today of 40 million, and 31 million in 2050) (UN 2002,
The demographic change has two important causes: increased life expectancy on the one hand, and a lower birth rate on the other hand, found in all the European countries. The average number of births in EU countries is 1.53 per woman [2]; Ireland has the highest fertility rate at 1.89, followed by Greece (1.30), Austria (1.32) and Germany (1.34). Italy and Spain have the lowest rates at 1.25 and 1.22, respectively (see Fig. 3). It cannot be expected that fertility rates will increase very much in European countries during the coming years.
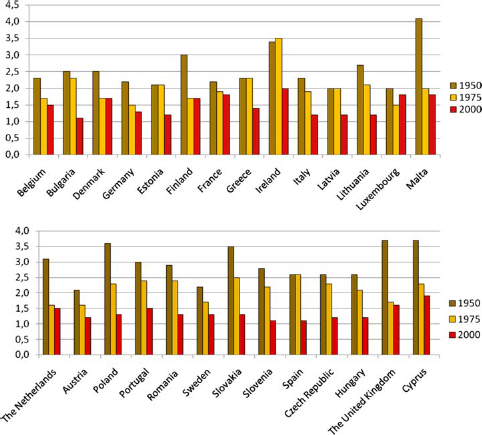
Fertility rates (number of births per woman)
Relationship between different age groups
One hundred and twenty years ago, the proportion of people older than 75 years to those younger than 75 was 1:79 in Germany; in 1925 the ratio was 1:67; in 1936, 1:45; in 1950, 1:35; in 1970, 1:25; in 1994, 1:14.8; and in 2000, it was 1:12.8. In 2007 it was 1:10.4, and by 2040 it will be 1:6.2.
This situation means that everything must be done to promote healthy and competent ageing! Physical activity, mental activity and social activity, as well as good nutrition, are all necessary for healthy ageing. But the onus is not only on the individual; it rests on society too. The city, the state, the country–-and also industry–-must all realise the great demographic change presented by the greying world. Urban planning and traffic services, for instance, will have to take into account the high percentage of elderly people.
The industrial sector needs to realise that society is ageing and change some of its products. Many older people are able and competent to drive a car (many of whom have difficulties walking), but the design of many cars is not well suited to them and causes them difficulties entering and exiting. Very often there are confusing and unnecessary electronic features that will never be needed. In the future, gas stations will have to offer more help to the elderly, and the same holds true for supermarkets. There will also be a greater need for portions and products designed for single-person households.
There is another point to mention: older people are also experiencing an important change in the structure of households. There is a trend away from the three-generation and two-generation household towards the one-generation household–-and from here to the one-person household. In Germany, only 1.1% of a total of 37 million households are three-generation households. In 1900, only 7% of all households were one-person households, while today these make up nearly 40%. In 1900, 44.4% of all households had five or more people, while today less than 5% of households are made up of five or more people. In the group of people 65 years and older, nearly 40% live in one-person households, and in the 75-plus age group, 68% of the women and 26% of the men live in one-person households. In Spain and other Southern and Eastern European countries the situation is much better: in Spain only 12% of the elderly live in a one-person household; in Portugal, 16.2% and in Greece, 18.6%. But arrangements in which the elderly live together with their children will decrease in the future, while the number of two- and one-person households will increase. This has consequences for potential caregivers. Therefore, more ambulant services for the aged will be required.
It should be remembered, however, that according to studies conducted in many European countries, this change in household structure should not be identified with loneliness or the isolation of the elderly, as frequent intergenerational contacts are reported to be independent of household structure. For those European countries in which the elderly have the highest number of contacts with family members–-such as Greece, Portugal and Italy–-studies by Walker and Maltby [4] found the highest percentage of individuals reporting loneliness (36% in Greece, over 20% in Portugal and 15-19% in Italy). However, in Denmark, where most of the elderly do not live together with their family, less than 5% reported feelings of loneliness (in Germany, the Netherlands and UK, 5-9%; in Belgium, France, Ireland, Luxembourg and Spain, 10-14%). The family integration of the elderly is quite different in each European country. While most of the elderly prefer ‘intimate relations at a distance’ (‘innere Nahe bei äuBerer Distanz’) as the ideal situation–-particularly in Denmark, the Netherlands and England, where less than 20% reported daily contact–-daily contact within the family structure in Italy, Greece, Portugal and Spain is much more common, reported by 60-70%.
There is also a trend away from the three-generation family to the four- or five-generation family. In former times a newborn child very seldom had the opportunity to know its four grandparents. Today a child very frequently comes to know all four grandparents and very often two great-grandparents as well. People in their 60s and older with greatgrandchildren are quite common, as well as people 60 years and older who care for their own parents. In our Interdisciplinary Longitudinal Study of Adulthood and Ageing, 36% of participants in their mid-sixties (born 1930-1932) reported having living parents or parents-in-law. The grandparent generation of today is the ‘sandwich generation’, helping children and grandchildren while also helping and caring for their own parents [1].
From the three-generation contract to the five-generation contract
The three-generation contract was introduced by Bismark, who created the pension system in Germany nearly 120 years ago. The idea of the three-generation contract is that people in the labour force have to provide (via insurance contributions and taxes) for those who are not yet working and for those who have finished working and are retired. Around the turn of the last century, the labour market consisted of 15- to 70-year-olds, who provided for those under 15 and over 70. But at this time only 2% of the population was 70 years and older. Today young people in Germany are beginning their occupational life at an average age of 25 years, and–-due to the the labour force situation and the high unemployment rate–-people in Germany are ending their occupational life when they are 59-60 years old (we have many special laws for early retirement). This situation is different in other countries: in Germany, of the 55-65 age group, only 43% of the men are in the labour force and 15% of the women; whereas in Spain, 54% of the men in this age group and 16% of the women are working; in Switzerland, 77% of the men and 59% of the women; and in Norway, 72% of the men and 59% of the women.
This early retirement age creates many problems both in the retirement system and in health insurance. The group of employed people between 25 and 59-60 years of age has to provide for those who are not yet working (and in some cases there are two generations of them, because some 30-year-old students have their own children in kindergarten) and for those who have already finished their occupational work–-and these make up 26% of the population, often two generations. This has consequences for the pension system: the employed have to pay about 20% of their earnings into pension savings. Today about three people in the labour force are needed to support one retired person; in 2040 the ratio will be one to one.
But once again, the problem is not primarily one of extended lifespans, but of the economic situation, because many of those 55 years and older are able to work, are healthy and willing, but the critical situation in the labour force makes it impossible.
Today the economic situation of the elderly in our country is still fine. Only 1.5-2% of the elderly are living beneath the poverty level (mostly women 80 years and older) and need social welfare support. In Germany it is quite unusual for grown-up children to give financial and material support to their parents. Very often it is parents and grandparents who are supporting their children and grandchildren from their pension. But this will change in the future.
Ageing does not necessarily mean becoming frail and dependent
Most older people, including those over 80, are competent and able to manage their daily life. Ageing is in no way identical to dependency. In the 60- to 74-year-old age group only 3-4% are dependent and in need of help. In the 75- to 80-year-old age group only 10% are dependent. In the 80- to 85-year-old group 19% need help or care; this figure rises to 36% for those who are 85-90 years old and to 60% for those 90 years and older.
But the number of people over the age of 80 will rise in all European countries. The number of people needing help and care could increase, although it is expected that dependency and helplessness will start at a later age. According to research findings the aged of today are in much better health than the aged of 15 or 20 years ago. The estimated number of people needing care in the future could be lower if the increase in life expectancy is caused by longer-lasting health, fostered by a healthier lifestyle, prevention and rehabilitation.
Today in Germany, 60-70% of caregivers for frail and aged people are family members. But this will change in the near future; family care has its limitations. Summarising the research findings on family care, we can state the following:
The age at which people become frail and dependent is rising; this will result in the age of potential caregivers rising as well.
The decrease in the number of children means that care for elderly dependent parents cannot be shared among several siblings.
Very often these one or two children live far away from their parents–-a necessity in industrial societies and a globalised labour market.
Family care is considered daughter care, but the daughter is very often a grandmother herself. This can lead to adverse effects on these women's personality development and to a negative geroprophylaxis. In short, they will have more difficulties preparing themselves for their own ageing. Very often the daughter has to take over the care of her parents at an age which offers her the final opportunity to re-enter the labour force or to take over roles in social or political organisations, churches, communities and so on.
More and more women are in the labour force, which does not allow intensive care for a dependent family member.
Because of the demographic change in many European countries, there is a growing number of single elderly people who do not have children.
There are also some indications that many elderly people are not too enthusiastic about living in a three-generation household.
The rate of divorce is increasing in many European countries (and women will not take care of their ex-mother-in-law).
In some cases it is better for elderly dependents to live in a nursing home where they can receive adequate medical treatment.
Any policy for the aged should keep in mind the demographic trends, mentioned above, which call into question the feasibility of family care as the only solution for frail elderly dependents. In their survey, Walker and Maltby [4] found that 70% of the population aged 60 and over in Europe agreed to the following statement: ‘Families are less willing to care for older relatives than they used to be’ (in Spain and Portugal this figure was 84 and 83%, respectively; in Germany, 64%; and in Ireland only 55%–-there the acceptance of family care stands at 44%, the highest in Europe: in Spain the figure is only 17%, in Germany 37%–-see Fig. 4).
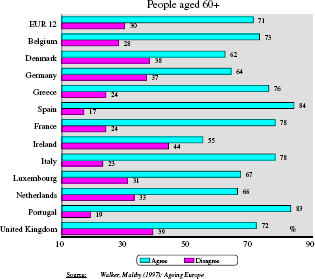
Families are less willing to care for older relatives than they used to be
While it is true that families who care for an aged person and keep him or her out of nursing homes should be supported by society, it is problematic to rely on family care as the only and best solution. As valuable and helpful as caring for a dependent and frail parent or grandparent may be for all family members, and as much as this may contribute to an increase in intergenerational understanding and the enrichment of the younger generation, there is no doubt that the same situation may lead to many problems within the family, especially for women. This means that we need a highly differentiated support system that can be adapted to specific demographic, regional and ecological situations from time to time. In the future we will have an increased need for highly qualified professional help and ambulatory services.
A policy for healthy ageing–-a challenge in our time
But first we have to do everything we can to promote healthy ageing. We know that life expectancy and quality of life do not depend only on physical or biological conditions. Social, psychological and environmental factors are also important. It is not only the state of curative medicine that affects life expectancy but also–-and to a much greater degree–- knowledge and compliance with preventive measures. Therefore, much more attention should be paid to prevention and rehabilitation. As people live longer, in fact, it becomes a task for every individual, as well as for society, to do everything possible to prolong the period of active, healthy living rather than simply delay the time of death. The importance of physical and mental activity must be made clear from childhood on. It is also necessary to maintain a high degree of physical, social and mental activity in men and women during adulthood.
There are many studies which demonstrate that physical activity is a prerequisite for successful ageing. Age-determined physical changes–-such as functional impairment of the organs, changes in the motor and muscular systems, as well as changes in the respiratory organs (which, of course, depending on the individual, can appear at any age)–-are similar to the effects of lack of exercise. The young, physically inactive individual seems old, just as the old but active individual seems young. Physical activity affects psychological well-being by promoting mental abilities, subjective well-being, social skills and self-image.
Mental activity is also a prerequisite of successful ageing. Many studies have found that individuals who are more mentally active, who have a higher range of interests, a better long-range perspective and a greater number of social contacts reach old age with greater feelings of psycho-physical well-being. It has been established that cognitive activity is essential for healthy ageing. An older person must be given mental tasks; she or he must be stimulated with (new) information and challenged to mental activity. A reduction in mental activity can speed ageing. This can also work in reverse: mental challenges can result in older people behaving spontaneously, as one would expect only from younger people.
Today a policy for the elderly must be more than a policy for pension systems and care. It must include other aspects than financial ones. In order to cope with the challenges of a greying world the following three issues should be stressed:
Maintaining and increasing the competence of the elderly in order to prevent dependency, to secure healthy ageing with a high degree of quality of life.
Extending and improving rehabilitation measures in order to re-enable the elderly to lead an independent life. It is quite necessary to promote rehabilitation programmes for the aged and to train medical doctors and nurses in geriatric medicine and gerontology.
Finding a solution to the problem of the dependent and frail elderly, and the problem of providing adequate care for them.
A policy for the aged is a policy for healthy ageing combined with a state of psycho-physical well-being. We know that ageing is affected by biological heredity as well as by individual behaviour and a wide range of social, environmental, cultural and political factors. Healthy ageing is the result of a life-long process.
Therefore, it is necessary to optimise the development of the individual. We know that a variety of influences in early childhood, adolescence, and early and middle adulthood, as well as in the present life situation of the aged, determine the process of ageing and well-being in old age. Interdisciplinary cooperation is needed, to which the biology of ageing, geriatrics and the behavioural as well as social sciences should contribute. Healthy ageing is a challenge for all gerontologists and geriatricians, a challenge for scientists of many disciplines–-a challenge for politicians and a challenge for all of those who work with the aged.
Concluding remarks
The demographic changes presented by an ageing Europe and an ageing world are a challenge for all of us. A policy for the aged, however, should not only be determined by the question, ‘What can we do for the aged?’; it must also consider, ‘What can the aged do for society?’ For this we need to revise the negative image of the aged that is found in some European countries, such as Germany. Most of the elderly are competent and wish to be engaged with other people and society. Societies, communities, churches, clubs and other organisations should promote this readiness for voluntary public engagement and be prepared to provide the framework and utilise the potential and services elderly people have to offer.
Some political and economic discussions in our country may give the impression that the extension of the average lifespan is the worst thing that could happen to the human race because of the rising costs for pensions and the health care system. Listening to some politicians, one might feel that it is very unlucky that so many people now survive to an advanced age, collecting a pension for which the younger generation has to pay. One should not forget, however, that it took much effort over many centuries to enable people to survive into old age. The history of medicine is one of continuous efforts to prolong human life. It would be strange to consider the great progress made in clinical medicine, biology and pharmacology as bad luck for women and men. For many years the World Health Organization has promoted programmes for healthy ageing. Science and politics are striving together to create new medical and economic conditions for achieving this goal–- and to educate people to persue a healthier lifestyle.
The increase in life expectancy shows that these efforts have been successful–-this is cause for celebration. It would be foolhardy to overlook the progress made so far in decreasing morbidity and mortality and instead focus only on the high costs associated with longevity.
Longevity should not be seen as a problem but as an opportunity and a challenge, a challenge for everyone: for the ageing individual, for his or her family and for society. We should not only ask about the problems and deficits of ageing and old age. We must also ask about–- and open our eyes to–-the new potentials of the aged, even the competencies and new potentials of very old people. We must see the aged as human capital.
Footnotes