
Abstract
Abstract
Purpose
The relationship between congenital talipes equinovarus (CTEV) and developmental dysplasia of the hip (DDH) remains uncertain. The role of routine hip screening in children with CTEV is debated. A recent study has found a high incidence of DDH in patients with CTEV. The aim of our study was to determine the true prevalence of radiographic hip dysplasia and identify the need for routine hip screening in patients treated for CTEV.
Methods
From a single centre database of 165 children consisting of 260 CTEV, a prospective radiological prevalence study of 101 children was performed over a period of 3 months. A single anterior-posterior pelvic radiograph was performed at a minimum age of 5 months. The DDH was determined by a single senior investigator based on the age-adjusted acetabular index (AI) as described by Tonnis.
Results
There were no dislocations or subluxations. According to the age-adjusted AI, 16 children had ‘light’ dysplasia and one child had ‘severe’ dysplasia. The child with severe dysplasia was known to have DDH and had already undergone treatment. The 16 children with light dysplasia did not require any form of treatment.
Conclusion
Out of one hundred and one children with CTEV, only one had DDH requiring treatment. This is consistent with the majority of the literature supporting the premise that there is no true association between CTEV and DDH. We, therefore, feel that routine hip screening for children with CTEV is not supported by current evidence and cannot be recommended.
Keywords
Introduction
Although the aetiology of both congenital talipes equinovarus (CTEV) and developmental dysplasia of the hip (DDH) remains unknown, it has been suggested that there may be an association between the two conditions [1, 2]. Despite this presumed association, there are no agreed protocols for routine screening and the efficacy of screening hips in patients with CTEV remains undetermined [3, 4]. Clinical examination alone has been shown to be inadequate in preventing late-presenting DDH [5].
The early identification of children with DDH is valuable as it allows for less invasive corrective procedures than if DDH is identified late [6]. Following reports about the inadequacies of clinical screening for DDH, the newborn and infant physical examination programme (NIPE) in the UK mandates the use of ultrasound screening for children with identified risk factors for DDH [7]. Currently, CTEV is not included as one of these risk factors. As with any screening programme, there are potential risks associated with over diagnosis and subsequent over treatment. The use of an abduction brace carries small but finite risks of avascular necrosis of the proximal femoral epiphysis, transient femoral nerve palsy, brachial plexus palsy and obturator foramen dislocation [8–14]. Furthermore, there are socioeconomic health concerns with radiologically screening and following up a large population of children [15].
Studies to date have shown a variation in the incidence of DDH in children with CTEV. Many of these studies have small numbers; and it has been difficult to draw any firm conclusions from them. Subsequently, there remains a debate about the true association between CTEV and DDH. The aim of this study was to determine the prevalence of radiographic hip dysplasia in patients treated for CTEV, and to, therefore, assess the value of routine hip screening in this group of children.
Materials and methods
This was a prospective radiological prevalence study of 101 children (202 hips), aged between 5 months and 8 years, treated for CTEV at a single centre over a 3-month period. Patient recruitment for this study was carried out at a dedicated talipes clinic, based on certain inclusion and exclusion criteria (Table 1). The diagnosis of CTEV had been made by the senior author based on the classical appearances of the foot and the severity was graded using the Pirani classification system [16]. Patients at our institute with CTEV are treated with the Ponseti method. Patients with a confirmed diagnosis of CTEV undergoing treatment in the talipes clinic at our institute, or on follow-up following treatment, were sequentially recruited into the study following parental informed consent.
Selection criteria
Approval for this study was gained from the National Research Ethics Committee as well as the hospital's Research and Development committee.
Patient demographics, the severity and treatment modality of CTEV, as well as any risk factors for DDH were recorded. These included breech position, positive family history, congenital postural deformities, and oligohydramnios.
A plain anteroposterior pelvic radiograph was performed with a protective lead shield to cover the gonads of all children, except those who had never previously had a pelvis X-ray. This was our institute's protocol, to ensure that no incidental pathology was missed due to the obscuring lead shield. The acetabular index (AI), defined as the angle between the Hilgenreiner line and the tangential line of the acetabular bony ridges, was used as a measure of DDH and this radiological assessment was performed by the senior investigator. The AI was first described by Kleinberg and Liebeman in 1936 and is considered to be a reliable measurement for the assessment of DDH with low inter-observer and intra-observer variability [17–19]. The age-adjusted AI can be used to determine hip dysplasia and subsequent need for further management [20]. Tonnis in 1976 published normative data for the AI based on age, gender and laterality [21]. We have used this data to define the presence of slight or severe dysplasia in our study patients (Fig. 1).
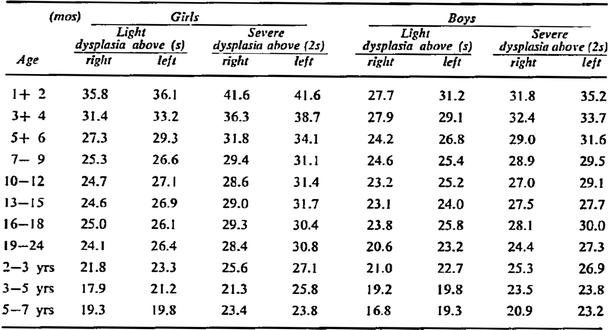
Acetabular index of light and severe dysplasias in different years of life (Tonnis [21])
Rotation of the pelvis X-ray was confirmed by calculating the ratio between the diameters of the obturator foramen. Acceptable rotation was considered with ratios between 0.56 and 1.8 [21]. Inclination of the X-rays was represented by calculating the symphysis-os ischium angle [21]. Any films outside these normal parameters were disregarded to ensure radiological measurements were reliable and reproducible.
This study did not include a control group as it was considered unethical to perform a radiation exposing procedure on a normal child without clinical indication. Thus, standard statistical tests were not employed; however, due to the rare nature of these two conditions, the sample size calculations were based on existing similar studies published in the literature.
Results
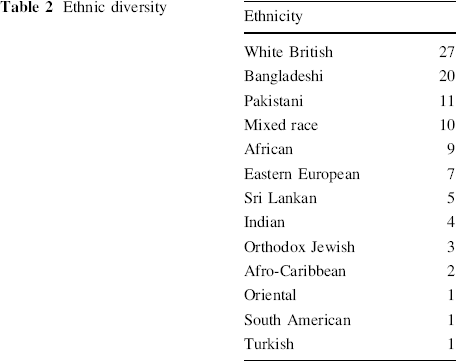
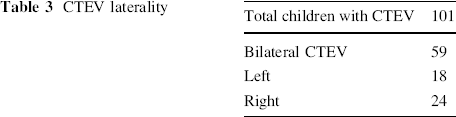
Of the 101 children included in our prospective study, 31 were female and 70 were male. The average age was 4 years old (range 5 months–8 years old). Our study included a significantly diverse ethnic population with over 13 different ethnic groups (Table 2). Two patients were found to have one of the established risk factors for DDH, namely one with a family history and one with a history of breech presentation in pregnancy. Fifty-nine children had bilateral CTEV and the initial mean Pirani score was 5.3 (range 3–6) (Table 3). We found no hip dislocations or subluxations and there were no newly diagnosed cases of severe hip dysplasia. According to the age, gender and laterality-adjusted AI described by Tonnis, 16 children had ‘light’ dysplasia and one child had ‘severe’ dysplasia in her right hip.
Ethnic diversity
CTEV laterality
Of all the 16 children with light dysplasia, none required any form of treatment. The age range for these children with light dysplasia, at the time of our study, was from 13 to 69 months old. The single child identified to have severe dysplasia in our study was known to have DDH. She was born at term and had undergone routine ultrasound hip screening because of breech presentation. Having initially failed Pavlik harness treatment, she subsequently went on to require a closed reduction and adductor tenotomy and entered our study after successfully undergoing treatment for acetabular dysplasia with subluxation, but with mild resolving residual acetabular dysplasia not requiring any current further intervention.
Discussion
There is current controversy in the literature as to the association between CTEV and DDH. Our prospective radiological study of 202 hips (101 children) supports the notion that there is no association between CTEV and DDH. Only one child had DDH and she had already been identified at birth due to her breech pregnancy. These results are consistent with the majority of other studies summarised in Table 4.
Summary of literature
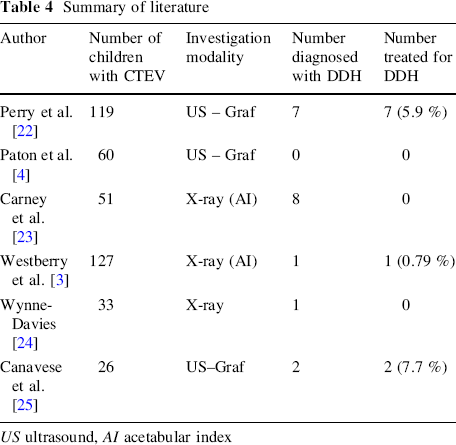
US ultrasound, AI acetabular index
This study identified sixteen children who fell within the Tonnis definition of light dysplasia based on the AI measurement adjusted for age, sex and laterality. None of these children required any form of intervention and further radiological follow up confirmed normalisation of the acetabular indices. A study by Carney et al., measured the AI in 51 children with CTEV and found eight children with an AI of more than 28°, which they defined as hip dysplasia [23]. According to the authors, no child underwent active treatment for acetabular dysplasia; so we can only presume that the radiological markers resolved on follow up. A number of studies have looked at children with borderline AI based on the age-related values of Tonnis. Mladenov et al. [26] studied 45 children with an increased age-related AI and concluded that clinically stable hips with light or severe AI values did not progress towards deterioration of hip morphology, even without treatment. D'Souza et al., studied 210 children with radiographic evidence of acetabular dysplasia who subsequently required no treatment and had normal radiographs at 12 months [27]. To date, the literature supports the favorable natural history of hips fitting the criteria for light or severe dysplasia without instability or displacement [28–31].
A recent study by Perry et al. [22] suggests that 5.9 % of patients with CTEV had DDH requiring treatment and they conclude that patients with CTEV should be considered for selective ultrasound hip screening. In their institute, they successfully treated six infants in a Pavlik harness; three with Graf IIb hips and three with Graf III hips. One patient with a Graf IV hip moved out of their region prior to any treatment. Graf in 1984 described the Graf IIb hip as having delayed ossification and recommended further follow up [32]. To date, there is no evidence that treating Graf IIb hips in a Pavlik harness alters the natural history of the development of normal hip morphology.
There is little evidence to support the treatment of mild to moderate hip dysplasia with abduction bracing [33]. Moreover, the use of a hip abduction brace is associated with a small yet finite risk of significant complications. Pavlik reported an incidence of avascular necrosis (AVN) in 2.8 % of 632 dislocated hips treated in his harness [34]. Although the actual incidence of AVN following use of an abduction brace is difficult to accurately evaluate, the reported incidence ranges from 1 to 15 % [35–38]. Tonnis has suggested that overly tightening the abduction strap may result in avascular necrosis [36, 39]. Ramsey et al. [14] highlighted the occurrence of a transient femoral nerve palsy in children treated for DDH with a Pavlik harness. Marnaghan et al. [40] showed that thirty (2.5 %) of the 1,218 patients they treated with a Pavlik harness suffered a transient femoral nerve palsy. Other complications that have been described include brachial plexus palsy and obturator foramen dislocation [13].
In our prospective study of 101 children, there was only one child with DDH that required treatment who had previously been identified due to breech pregnancy. Westberry et al. [3] retrospectively reviewed the hip radiographs of 127 patients with CTEV and found only one patient with DDH. She was born prematurely by Caesarean section and was a product of an extra-abdominal pregnancy. Other studies with similar results also suggest that there is no true association between these two conditions [2–4]. In addition, Brown et al.[15] have estimated total costs of selective screening per 100,000 live births, in the United Kingdom, at £3 million for selective ultrasound screening versus £1 million for clinical screening alone. Combined with the potential medical risks of over treating patients in a Pavlik harness, it seems inappropriate to include patients with CTEV in a targeted screening programme.
We acknowledge there are certain limitations to this study. The age at which plain radiographs were performed in our study to assess hip dysplasia varied significantly. A child with a normal AI aged 10 could potentially have had a mildly dysplastic hip at an earlier age. Whilst this may not have affected their treatment, it could have some bearing on our study results. Radiographic follow up of patients with light dysplasia was not conducted as part of the study protocol; however, these patients remain under clinical follow up at our institute. Ethical restrictions prevented direct comparison to a control group or the continued recruitment of patients to achieve statistical power in light of the study findings.
Conclusion
The results from this prospective cohort study demonstrate that the mere presence of CTEV in the absence of any well-established risk factors for DDH does not indicate a higher incidence of DDH. This is consistent with the majority of the literature in support of the idea that there is no association between CTEV and DDH. Clearly, a population wide prospective epidemiological study to assess the link between true CTEV and DDH would be the most appropriate next step. However, we feel that routine hip screening for children with CTEV is currently not warranted.
Footnotes
All authors declare no conflict of interest in the preparation of this manuscript. All authors declare no relevant financial relationships.