
Abstract
Abstract
Purpose
The eight-plate system for angular deformity correction is well known, reliable and effective at any age during growth. Due to high implant costs, we sought to evaluate the effectiveness and safety of a less expensive alternative.
Methods
Between 2006 and 2011, 41 children with angular deformities were managed using a two-hole one-third tubular plate in cases where an eight plate would normally be indicated. Inclusion criteria in this retrospective study were: genu valgum and genu varum. X-ray documentation was performed before and after surgery and patients were followed clinically every 3 months after surgery. The cost per implant was 361.40 Sfr (Swiss Francs) compared to the eight plate at 737 Sfr.
Results
Mean time for correction was 13 months. A mean LDFA/MPTA after correction of 89.9°/86.8° was recorded, as well as a mean correction angle of 6.8°/6.6°. The complication rate was 6.6 % (one superficial wound infection and one insufficient correction in an older child). These results compare favourably with published data on the eight plate.
Conclusion
The two hole one-third tubular plate seems to be a clinically and also cost effective alternative to the eight plate. Full deformity correction is gained for a fraction of the cost. Level of Evidence: Level III
Introduction
Angular deformities particularly in the frontal plane around the knee often require hemiepiphysiodesis in children or adolescents [6]. Temporary hemiepiphysiodesis is a common procedure [13, 19] carried out as a minimally invasive technique to correct angular deformities and is used to ‘guide growth’. Techniques with different implants (transphyseal screw, staples) for hemiepiphysiodesis have been reported in the literature [4, 5, 9, 10]. The direct ablation of one side of the physis has also been reported [3]. The 8-plate (Orthofix, McKinney, Tex), a tension band device, was introduced in 2005 [2, 11, 16, 17]. This system has been reported as a reliable and effective tool at any age [4], even if it seems to be less effective in some diseases [14].
The long-term effectiveness of both epiphysiodesis techniques (staples or eight plate) is similar. However correction was achieved in less time with the 8-plate than when using conventional staples. Longitudinal growth inhibition is also lower when using the 8-plate [7].
Due to high implant costs of the 8-plate we sought to evaluate the use of a less expensive alternative—a two-hole one-third tubular plate (Synthes, Oberdorf, Switzerland). We analysed the correction power of this plate and report on costs and complications of the treatment. A comparison with the common implants described in the literature was made.
Materials and methods
Between January 2006 and April 2011, 41 children (total number of limbs: 57, number of femora: 43, number of tibiae: 14, number of patients where tibia and femur were involved: 4) with progressive pathological and symptomatic (pain, gait problems) angular deformity (idiopathic genu varum, idiopathic genu valgum), were treated at our institution with hemiepiphysiodesis by using a one-third two-hole tubular plate (Synthes, Oberdorf, Switzerland). Photographic documentation and X-ray radiographs (long leg standing views) were performed before surgery and after the correction was achieved. After metalwork removal patients were followed up routinely until the treated physis had fused. Depending on deformity location mechanical Lateral Distal Femoral Angle (mLDFA) and/or mechanical Medial Proximal Tibial Angle (mMPTA) described by Paley and Herzenberg [12] were measured. The monthly rate of change of each angle was evaluated. Also mLDFA and/or mMPTA were correlated with time needed until correction was achieved and these data were compared to available results in the current literature using the standard eight plate and staples. We assessed the total time until correction and the rate of angle change before and after metal removal. Demographics for each patient including gender, age at surgery and age at metal removal. The complication rate and functional outcome were also recorded.
Patients were evaluated clinically every 3 months postoperatively. In 30 cases, the device was removed electively. In four cases a complete data set was not available, and therefore these patients were excluded from the study. Seven children are currently still undergoing treatment and have the implant in situ.
A statement of costs per implant (in Swiss Francs = Sfr) has been performed and the amount has been compared to the Orthofix eight-plate device.
Surgical technique
Biomechanically, the capacity of the tension bend effect is used, and surgically almost all principles of the eight-plate system were inherited, beside the fact that it is not possible to use a physeal guide wire to insert the plate due to the missing hole in the centre of the product.
After a 2-cm skin incision and localization of the centre of the physes by using an X-ray, the (not pre-bent) plate was inserted with a needle holder and non-threaded 1.6-mm guide wires above and below the physes were inserted directly in the centre of the intended plate holes.
After position verification, solely the cortex was threaded followed by insertion of the self tapping screws, which need to be positioned parallel or slightly divergent.
Immediate weight bearing was possible after the procedure. Clinical follow ups were performed on a 3-month routine until full correction was achieved.
Statistics
All data was collected on an Excel (Microsoft ™) spreadsheet and results were expressed as means and standard deviations of each data set. Correlations were compared using Pearson's correlation coefficient for parametric data and the correlation curves so created. A p value <0.05 was considered statistically significant. Analysis was performed using the Statistica V6 software package (Statsoft Inc., Tulsa, Oklahoma).
Results
Forty-one patients (16 female, 25 male) with symptomatic angular deformity were treated at our institution using this technique between 2006 and 2011. Seven patients are still undergoing correction. The four cases without complete data were excluded from the study, leaving a total of 30 patients with a complete data set. From this data set, the total number of limbs that underwent surgery was 57 with 47 femurs and 14 tibiae. Mean follow up was 3.2 years (Min 2.4 years, max 4.3 years). Mean age at time of surgery was 10.6 years (±4.87). Mean surgery time in unilateral cases was 27 min (±7 min) and in bilateral cases 42 min (±8 min). Mean duration of hospital stay was 2.2 days (1–5 days).
Metal removal was performed at the mean age of 11.9 (±2.05). Mean correction of mLDFA was 7.43° (±2.78) with a mean monthly rate of change of 0.73 (±0.32) degrees. Mean correction of mMPTA was 7° (±2.11), with a monthly angle change of 0.51 (±0.19) degree. The total time to achieve overall correction was 12.37 months (±5.46) and metal removal was performed at this time. The mean time for correction of the mLDFA was 11.63 months (±4.31) compared to the mMPTA which was 15.43 months (±7.19).
In two patients (6.6 %), postoperative complications were observed. One boy developed a superficial wound infection which was treated successfully with antibiotics, without the need for further surgical intervention. In one girl the full correction desired was not achieved. In no cases hardware loosening or failure occurred. Premature growth arrest was also not detected in any case.
Correlations were carried out between time and the change of both the femoral (mLDFA) and tibial (mMPTA) angles. A statistically significant correlation (p = 0.01) was noted between time and change of the femoral angle as demonstrated in the graph in Fig. 1. Again a statistically significant correlation (p = 0.03) was noted between age and the rate of change of the femoral angle as demonstrated in the graph in Fig. 2.
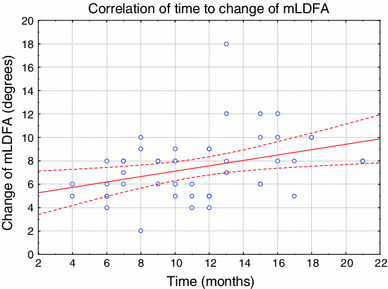
Graph showing correlation between time and change of mechanical lateral distal femoral angle (mLDFA). Statistically significant: r2 = 0.1274; r = 0.3569, p = 0.0138. 95 % regression bands shown
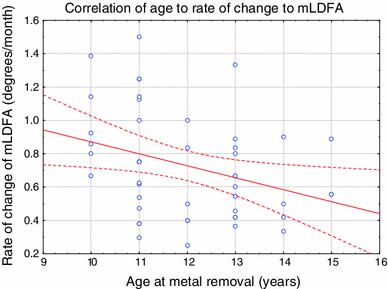
Graph showing correlation between age and rate of change of mechanical lateral distal femoral angle (mLDFA). Statistically significant: r2 = 0.1054; r = −0.3247, p = 0.0260. 95 % regression bands shown
Time and change of the tibial angle was not statistically significant for the tibial angle (p = 0.09). Similar findings were seen when the rate of change of mLDFA and mMPTA were compared to the age of the patient at metal removal Figs. 3 and 4.

Implants used
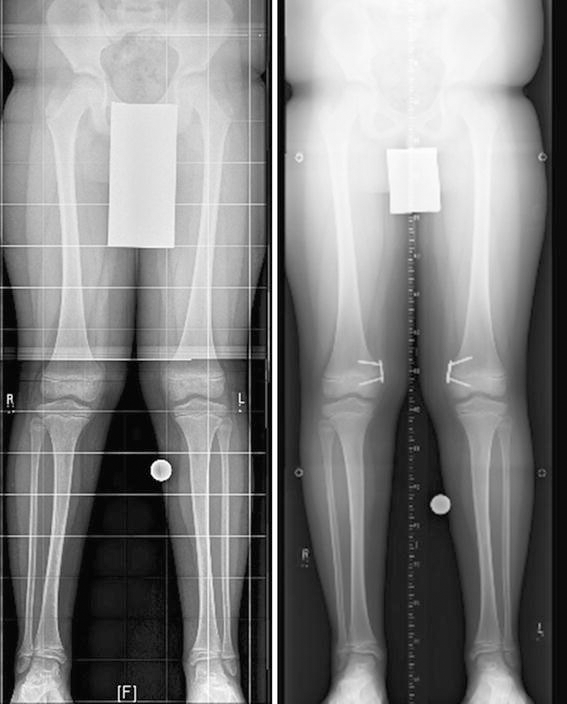
An example of the correction achieved using the one-third tubular plate
Also no significant correlation between age and the rate of change of the tibial angle (p = 0.35) could be found. No rebound effect was observed in our patient group.
The implant costs (in Swiss Francs = Sfr) of the original eight plate device (Orthofix) consisting of two cannulated screws (400 Sfr in total), one eight plate (235 Sfr) and a double pack of K wires (102 Sfr) are in total 737 Sfr. The two-hole one-third tubular plate device (Synthes) is 361.40 Sfr (two cannulated partly threaded screws are 156 Sfr, one two-hole one-third tubular plate is 147.80 Sfr and two standard K wires are 57.60 Sfr).
For renting the Orthofix device, 120 Sfr. is charged and buying the complete system would cost in total 2,658 Sfr. (Orthofix prize list 2011, Orthofix AG Zug).
Discussion
Temporary epiphysiodesis using a tension band device is gradually becoming the gold standard in the treatment of angular deformities, particularly in the coronal plane around the knee. It is a minimally invasive technique and seems to be effective at any age during growth. Complication rates including hardware failure and longitudinal growth inhibition are reduced compared to other techniques such as staples and transphyseal screws [15, 16, 18, 20].
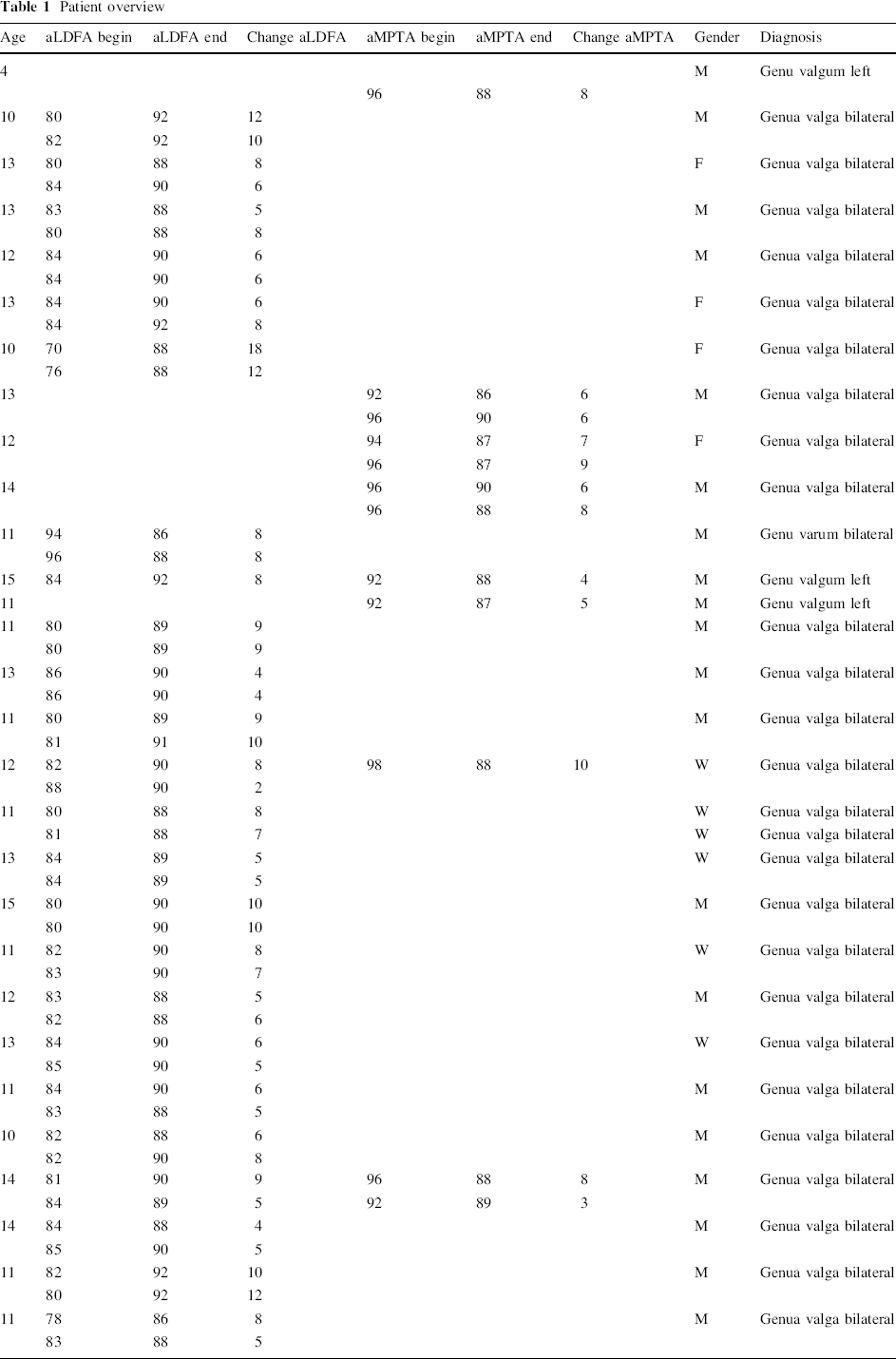
Our series of 30 patients (Table 1) is comparable to the current literature examining correction of deformity using the 8-plate and included a multiplicity of pathology causing the deformity (idiopathic, posttraumatic, multiple exostosis, Blount's disease). The mean correction time in our series was 12.3 months. Stevens et al. [16] published a group of 34 patients “with 65 deformities due to a variety of pathological conditions” in 2007 and correction was achieved in this group after a mean of 11 months. Ballal et al. [1] described 25 patients with symptomatic genu valgum and varum also managed with the 8-plate device who had a mean correction time of 16.1 months. Guzman et al. [8] were the first group who focussed solely on the treatment of idiopathic genu valgum with the tension band plate and reported on two cases which had a mean correction time of 13.5 months. All authors noted a faster and greater potential for correction in younger patients particularly those less than 10 years of age. With a mean age of 10.6 years at surgery and 11.9 years at plate removal the two hole one-third tubular plate used in our patients confirms our initial hypothesis that it as effective as the 8-plate. With this system the mean correction of mLDFA was 0.73° per month which is as fast as described in the above mentioned studies.
Patient overview
Furthermore we noted a lower correction rate for the mMPTA measured at 0.51° per month in our series, again a finding similar to that in previous studies [8]. With regard to the mean time until correction was achieved, mean overall correction of mLDFA and mMPTA and monthly correction rate of mLDFA and mMPTA the findings in our study were again comparable to those previously published using the standard eight plate. Stevens [16] described complications in four patients age under the age of 11 years, where he detected rebound phenomenon and the requirement for further surgery. The same series also reported hardware loosening in one patient with Blount's disease. Otherwise no complications including premature physeal closure or overcorrection were noted in his study. Results with the two hole one-third tubular plate presented in this study show a similarly low complication rate of 6.6 %. All of our patients were treated using partially threaded, cannulated, self tapping screws (3.5 mm). No hardware loosening or failure was found. No overcorrection or the revision surgery has been required thus far. In one case (a girl) where treatment was started at the age of 12.5 years, the correction was insufficient and further treatment will be necessary in the future.
Regarding cost effectiveness the two hole one-third tubular plate at a cost of 361.4 Sfr per implant is superior to currently available systems—an aspect of modern medicine that is becoming even more important. The plate itself costs less than half of the price for the original Orthofix device. The instrumentation rental fee (120 Sfr) or purchase costs of the whole system (2,658 Sfr) can be eliminated as the instruments required for using the one-third tubular plate such as the drill and screw driver are very likely to be available in every pediatric orthopaedic department.
The only potentially perceived difference in the one-third tubular plate may be the absence of a central guide hole. In our experience, however, this did not appear to increase the technical difficulties or time taken for the surgery.
Guided growth using the two hole one-third tubular plate gives reliable results and it is as effective and safe as currently available systems, in patients with idiopathic genu valgum or varum.
We have shown efficacy in regard to overall correction time as well as correction rate per month and demonstrated a low and acceptable complication rate in our patient group. Additionally the system is highly economical and is likely to be already available in the large majority of centres allowing children to be treated with this powerful system for a fraction of the costs attributed to other devices.
Footnotes
None.