
Abstract
Abstract
Purpose
The aim of this study was to determine the prevalence of developmental dysplasia of the hip (DDH) in preterm infants with maternal risk factors.
Methods
A prospective review of the medical records and ultrasound (US) scans of all preterm infants at one tertiary-care children's hospital was completed to identify all premature infants without any infantile risk factors at a particular time frame. We consecutively evaluated 421 babies (842 hips) who satisfied the criteria for inclusion. Hip US images were classified according to Graf.
Results
Overall, one hip was diagnosed as DDH (Graf type 2c). Female infants had significantly lower alpha angles (70.2 ± 6.6 and 71.4 ± 4.4 for females and males, respectively) (P = 0.033). There was no correlation between oligohydramnios and alpha and beta angles and hip sides (P = 0.345 and P = 0.789 for left and right hips, respectively). US examination of the infants revealed no differences between the alpha and beta angles of the hips and birth weight and age at gestation. Although it was statistically not significant, US evaluation of left hips among singletons demonstrated one immature hip (P = 0.864) and that of right hips demonstrated one immature hip for both singletons and twins (P = 0.904).
Conclusions
Prematurity with or without maternal risk factors does not have an effect on DDH.
Introduction
Hip ultrasonography (US) is widely accepted as the imaging method of choice to screen hip abnormalities in babies between 4 to 6 months of age. Attempts to evaluate the reliability of ultrasonographic measurements showed high intraobserver reproducibility and interobserver reliability. Although US scan in infants with low birth weight and prematurity can make hip typing and subsequent treatments complicated, US is still useful in the neonatal period of infants with positive family history or clinical signs for developmental dysplasia of the hip (DDH).
Numerous authors have examined various risk factors for DDH. Gardiner et al. [1], Bielski et al. [2], Azzopardi et al. [3], and Tuncay et al. [4] have recognized prematurity as being less prevalent in DDH. Although each of their articles contributes to our knowledge, none provides a comprehensive review of prematurity as a solitary risk factor for DDH. We, therefore, performed a prospective analysis to address two questions: (1) does prematurity have an effect on DDH; (2) do gender, birth weight, twinness, and oligohydramnios play a role on DDH in the case of prematurity.
Materials and methods
This prospective study evaluated a consecutive sample of 449 premature infants who were born in or admitted to Zekai Tahir Burak research hospital, division of child development, from September 1, 2008, through June, 2011. Infants with chromosomal, genetic or structural defects, and signs of intrauterine infection or neonatal early-onset sepsis were not eligible for this study. The study protocol was approved by the local Ethics Committee and written informed consent was obtained from the parents or legal guardians of all participants.
Prematurity was accepted as being born before 37 weeks of gestation, counting from the first day of the last menstrual period. Prenatal and neonatal data were recorded, including the type of delivery, birth weight, week of gestation at birth, state of amniotic fluid during pregnancy, and risk factors. Family history, postural or structural deformities of the foot, and torticollis were accepted as risk factors for DDH. We excluded 28 infants with the above-mentioned risk factors and a total of 421 infants were ultrasonographically evaluated.
All participants were studied using the same protocol, consisting of bilateral hip US scans according to Graf's technique in the third or fourth weeks after delivery. Prior to US, all babies’ physical examinations were carried out to look for Ortolani, Barlow, and Galeazzi signs, and for restriction in abduction. US images were obtained with a Login 200 equipment using a 7.5-MHz linear transducer. Examination included two static coronal images of the hip. All images were evaluated by our senior author (S.K.), who is trained in the evaluation of neonatal hip US. US images were classified according to Graf's morphologic assessment. All measurements were repeated by three orthopedic residents (C.S., I.D., and S.U.) on two different occasions and the mean values were chosen in order to reduce the error. For intra- and interobserver reliability, all images were assigned a random number and were independently and blindly measured, and a single measurement, the interclass coefficient (ICC), was determined. Convergent validity (Pearson's r) was evaluated by correlating measurements. Reliability was excellent (ICC > 0.80) in all but four assessments.
Comparison between alpha and beta angles of right and left hips and gender were carried out using an independent-samples t-test. The Chi-square test was used to determine any significance between Graf types and gender. Also, an independent-samples t-test was used to reveal any difference between birth weight with hip angles and amniotic fluid state with hip angles. Regression analysis was used to examine the effects of amniotic fluid state, birth weight, and twinness on the alpha and beta angles. Comparison between triplets and twins for alpha angles was carried out using a two-sided Mann–Whitney U-test for medians and Fisher's exact test for proportions. Kruskal–Wallis one-way analysis of variance (ANOVA) was used to identify differences between parity and alpha angles. All statistical analyses were calculated with the SPSS 15.0 statistical software (SPSS for Windows, SPSS, Inc., Chicago, IL).
Results
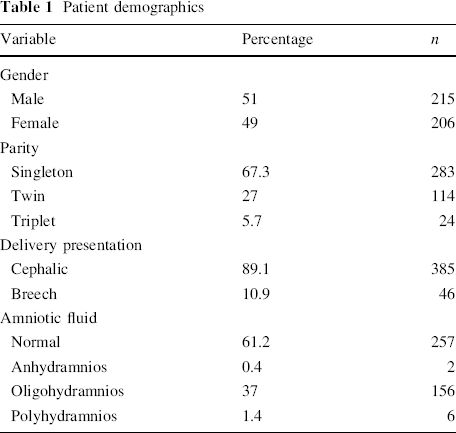
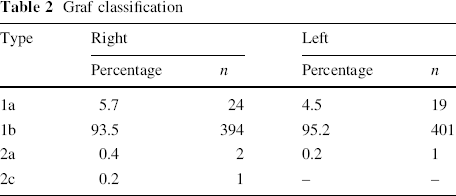
Among the 421 premature infant (842 hips), only one hip (0,246 %) was diagnosed as DDH (right hip, Graf type 2c). The demographic details are summarized in Table 1, and the results of the Graf typing are displayed in Table 2. On physical examination, there were no unstable hips among the patients. Only one patient had indistinct restriction in abduction and the same patient's US revealed Graf type 2a hip. The baby with type 2c hip was treated by a Pavlik bandage for 6 weeks and wore an abduction brace for another 4 weeks, and she had a stable hip at the end of the treatment. One baby with bilateral type 2a hip and one baby with unilateral type 2a hip were followed up and their fourth month (according to corrected age) US evaluations revealed type 1 hips in both babies. Although there were no differences between Graf types and gender (P > 0.05), female infants had significantly lower alpha angles (70.2 ± 6.6 and 71.4 ± 4.4 for females and males, respectively) (P = 0.033). The mean birth weight was 1,401.42 ± 366.725 g (range 560–2,890 g) and the mean age at gestation was 30.44 ± 2.443 weeks (range 22–37 weeks).
Patient demographics
Graf classification
There were no differences between both right and left hips with birth weight and age at gestation (Table 3). A detailed analysis of the type of US findings and parity with both right and left sides showed no statistical significance. US evaluation of left hips among singletons demonstrated one immature hip (P = 0.864) and that of right hips demonstrated one immature hip for both singletons and twins (P = 0.904).
Comparison of right and left hips with birth weight and age at gestation
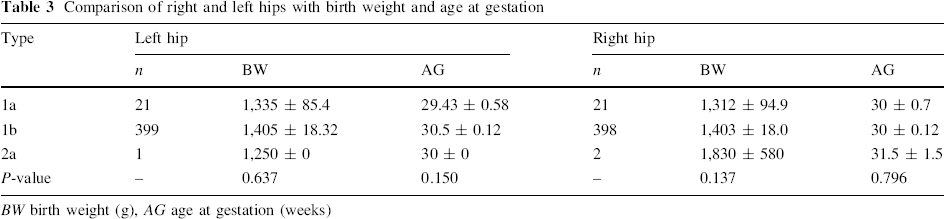
BW birth weight (g), AG age at gestation (weeks)
A well-known risk factor for DDH is breech delivery. Although there were two type 2a right hips (P = 0.733) and one type 2a left hip (P = 0.486) for cephalic presentation, there was no type 2a hip detected among breech presentations (n = 48). Another risk factor for DDH is oligohydramnios. There were 159 cases with oligohydramnios. There was no correlation between oligohydramnios and alpha and beta angles and hip sides (P = 0.345 and P = 0.789 for left and right hips, respectively). The finding of oligohydramnios among 158 (seven type 1a and 151 type 1b) normal hips and only one immature hip can be explained as lower risk for DDH. When the effects of amniotic fluid state, birth weight, and twinness on alpha and beta angles were examined by regression analysis, multiparity was found to have an inverse effect on left alpha angles; again, female gender had an inverse effect on the right alpha angle. Also, there was a statistically significant difference in the alpha angles between singletons and twins (P < 0.05). Among bilateral hip US evaluations, there was no statistical difference between the alpha and beta angles of right and left hips (P > 0.05). However, the beta angles of left hips of male infants were significantly higher than that of the beta angles of right hips (P = 0.033). Although left alpha angles were higher among singletons, twins had lower left alpha angles (P = 0.01).
Discussion
The results of this study suggest that prematurity has no effect on the prevalence of DDH. Our findings are consistent with recently published long-term studies that were conducted in infants during the neonatal period to evaluate multiple risk factors for DDH [3, 5–8].
DDH is associated with specific suboptimal development affecting both the acetabulum and proximal femur, suggesting the need for concentric reduction for an acceptable hip development. Early diagnosis is the mainstay of treatment and the gold standard for the diagnosis of DDH before 4 months of age is US screening. US was used in many reports to evaluate the effect of risk factors on DDH.
Among risk factors previously reported, the most important ones are female gender, family history, and breech presentation [9]. These risk factors with positive clinical signs have a significantly increased effect on the diagnosis of DDH. Although the impact of female gender is milder than that of breech delivery and family history, actually, DDH can be associated with some other risk factors, such as oligohydramnios, congenital foot abnormalities, primiparity, cesarean section, nationality, first-born child, low birth weight, low gestational age, first-trimester maternal hyperthyroidism [10], congenital muscular torticollis [11], and twin pregnancy [12]. The rate of subsequent development of hip dysplasia with the existence of one or more risk factors in infants may range from 0.1 to 10 % [13].
There is a tendency toward screening programs in newborns to detect DDH earlier. A review of the studies that were carried out in our country shows a pronounced decrease in the prevalence rate of late DDH. In their cross-sectional study, Kutlu et al. [14] found that the prevalence rate of late DDH in 1992 was 15.7 %. However, in 2011, Songür et al. [15] established a study to discover the prevalence rate of late DDH in Turkish children aged 6 months to 14 years from more than 20 provinces of our country and found a 5.9 % rate of late DDH. Especially increased public awareness, increased birth rate under the supervision of a healthcare provider, and after introducing hip US screening for documented risk factors by experienced physicians, the rates were decreased. In a recent study by Akman et al. [8], risk factors such as female gender, family history, swaddling, oligohydramnios, and primiparity for DDH were evaluated and hip US results were reported. In their study, the only inclusion criteria was proper sonographic evaluation and data were collected from the same region as in our study. They found the prevalence of DDH to be as high as 3.4 % in 403 babies (14 of 403 babies; five type 2b, seven type 2c, one type D, and one type IV). When type 2b immature hips are excluded from the prevalence rate, the corrected rate of DDH in 403 babies can be calculated as 2.2 %. Apart from our study in which only prematurity analyzed as a risk factor, they stated that oligohydramnios and swaddling in the presence of female gender was the most important risk factors in the unilateral analysis for DDH. However, we could not detect any correlation between oligohydramnios and alpha and beta angles and hip sides. Multicentric studies are definitely needed in order to clarify the effect of oligohydramnios on DDH in case of prematurity.
Several authors emphasized the importance of US screening for the diagnosis of DDH in conjunction with common risk factors. As Hansson et al. [16] themselves noted, the screening of children in maternity wards may reveal a substantial number of babies that have been missed for hip dysplasia in postpartum intensive care units. They concluded that prematurity can increase the risk of late DDH due to neglected diagnosis [16].
We found an inverse proportion between birth weight and alpha angles among especially premature infants with low birth weight. Timmler et al. [17] also emphasized the increased incidence of type 2a hips together with the increase of birth weight in premature infants who were examined later, during the third month of life. However, they found no statistically significant difference at the final examination. Our results are compatible with this report and we recommend secondary hip US examination in case of an alpha angle between 50–60°.
Bache et al. [5] questioned the prevalence of DDH in babies with common risk factors and attempted to ascertain which babies have to be selected for hip screening. They accepted gender, family history, breech delivery, cesarean section, and birth weight as risk factors, and concluded that those babies with a birth weight of more than 4 kg to have a two-fold increase for US abnormality. Apart from this study, nevertheless, Dogruel et al. [18] considered both low birth weight (<2,500 g) and prematurity (<37 weeks gestational age) as risk factors for DDH. Although they found Graf type 2b or more severe DDH in 7 of 262 infants with prematurity and 6 of 253 infants with low birth weight, they concluded that there was no significant association between DDH and prematurity and low birth weight.
A previous study by Tuncay et al. [4] aimed to determine the importance of prematurity and suggested the incoherence of prematurity in hip typing. They compared preterm and term infants and found no statistical differences between the two groups with respect to hips that required further treatment. The results of the present study support those of this report and indicated that individual evaluation of both left and right hips with regard to birth weight, age at gestation, parity, twins, breech delivery, oligohydramnios, cesarean section, and prematurity have no effect on the prevalence of DDH.
Our study has some limitations. Only referrals to a single tertiary-care institution were included. It would be ideal to perform a multicentric analysis to evaluate the effect of prematurity on DDH. The second limitation is that only static coronal images of the hips were evaluated. The dynamic methods of Harcke and Clarke were not used, thus, static assessment can theoretically miss an unstable hip; this represents the ‘worst-case scenario’. However, we believe that the design of this study presents two important differences with respect to a previous report [4]. First, we performed serial US scans on preterm infants without pediatrician referral due to established risk factors or positive clinical findings, which, consequently, allowed the prevalence of DDH to be established more reliably. Second, Graf typing was performed in particular with maternal factors such as breech delivery, cesarean section, twin pregnancy, and oligohydramnios, an approach not used in previous studies.
In conclusion, the results of this study suggest that prematurity cannot be accepted as a risk factor for DDH. Risk factors such as breech delivery, twin pregnancy, cesarean section, and oligohydramnios, in conjunction with prematurity, should be assessed in future studies evaluating abnormal findings in US scans. Nonetheless, the information provided here can be used cautiously to counsel parents and developmental services for preterm infants that having positive physical findings and additional risk factors. These findings should be confirmed and expanded in larger studies to refine the natural developmental history of hip dysplasia in preterm infants.
Footnotes
None.