
Abstract
Abstract
In 1983 Howard King presented his classification system for adolescent idiopathic scoliosis (AIS) based on the experience with Harrington rod instrumentation. Curves were divided into five types and guidelines and recommendations for which levels should be instrumented were given to preserve motion as much as possible. As segmental instrumentation systems began to gain favor over the Harrington rods this system failed and led to the development of a new classification system which was presented by Lawrence Lenke in 2001. In order to define a curve type by the Lenke classification, one must identify the curve type, the lumbar modifier and, for the first time in any classification system for scoliosis, the sagittal profile was also included. The Lenke classification showed higher inter and intra-reliability compared to the King classification. It also provided a better and more reliable tool to assist surgeons in choosing the best method of treatment for each curve pattern. Although the Lenke classification is more comprehensive and reliable than the King classification it is still far from perfect. It does not address the rotational component of the deformity. New technologies which provide three-dimensional (3D) reconstruction of the spine may serve as a basis for a truly 3D classification of scoliosis and for new therapeutic concepts.
In 1948 John Cobb was the first to describe a classification system of scoliosis. He was the first to give a description of major and minor curves, structural and non-structural curves and set guidelines for treating these deformities accordingly.
In 1983 Howard King presented his classification system for AIS [1]. This system was based on the experience of John Moe in the surgical treatment of AIS patients with Harrington rod instrumentation. Curves were divided into five types and guidelines and recommendations for which levels should be instrumented were given according to those different curve types in order to preserve motion as much as possible. King et al., gave, for the first time, some very important definitions which some are still widely used today: (1) Stable vertebra: the vertebra most closely bisected by the center sacral vertical line (CSVL). (2) Structural versus Compensatory curves: the curves were defined according to their flexibility on side bending films.
King and Moe defined five curve types (Fig. 1):
The King classification published 1983 [1] Type 1: an “S” shape deformity, in which both curves are structural and cross the CSVL, with the lumbar curve being larger than the thoracic one. Type 2: an “S” shape deformity, in which both curves are structural and cross the CSVL, with the thoracic curve being larger or equal to the lumbar one. Type 3: major thoracic curve in which only the thoracic curve is structural and crosses the CSVL. Type 4: long “C” shape thoracic curve in which the fifth lumbar vertebra is centered over the sacrum and the forth lumbar vertebra is tilted into the thoracic curve. Type 5: double thoracic curve.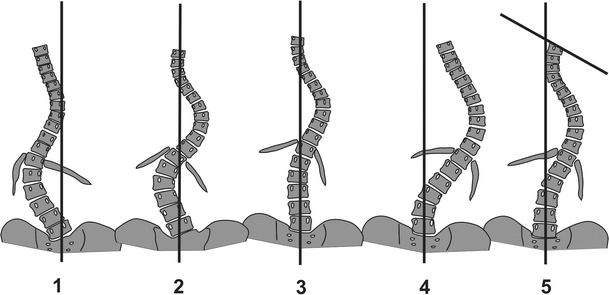
As segmental instrumentation systems began to gain favor over the Harrington rods this classification system failed to give accurate and reliable guidelines for choosing the proper levels for fusion [2–4]. In addition, several articles showed low inter and intra-observer reliability of this classification system [5, 6].
This lead to the development of a new classification system which was presented by Lawrence Lenke in 2001 [7]. In order to define a curve type by the Lenke classification, one must identify the curve type, the lumbar modifier and, for the first time in any classification system for scoliosis, the sagittal profile was also included. A few new definitions were made: (1) Major curve: the curve of greatest magnitude and is always structural. (2) Minor curve: a smaller curve which may be structural or nonstructural. (3) Nonstructural curve: a curve which bends to less than 25° on side bending radiographs.
According to these definitions there are six different curve types (Fig. 2):
The Lenke classification published 2001 [7] Type 1: main thoracic (MT) is the only structural curve while the others (proximal thoracic and lumbar or thoracolumbar) are nonstructural. Type 2: double thoracic in which the MT is the major curve, the proximal thoracic (PT) is the minor curve but is structural and the thoracolumbar (TL) or lumbar (L) curves are minor and nonstructural. Type 3: double major curve pattern in which the MT is the major curve and the lumbar is the minor one but is structural whereas the PT is nonstructural. Type 4: triple major curve pattern when the MT is the major curve but all three curves are structural. Type 5: the TL or L curve is the major and only structural curve, with the PT and\or MT curves being minor and nonstructural. Type 6: the TL or L curve is the major curve measuring at least 5° more than the MT which is the minor but structural curve.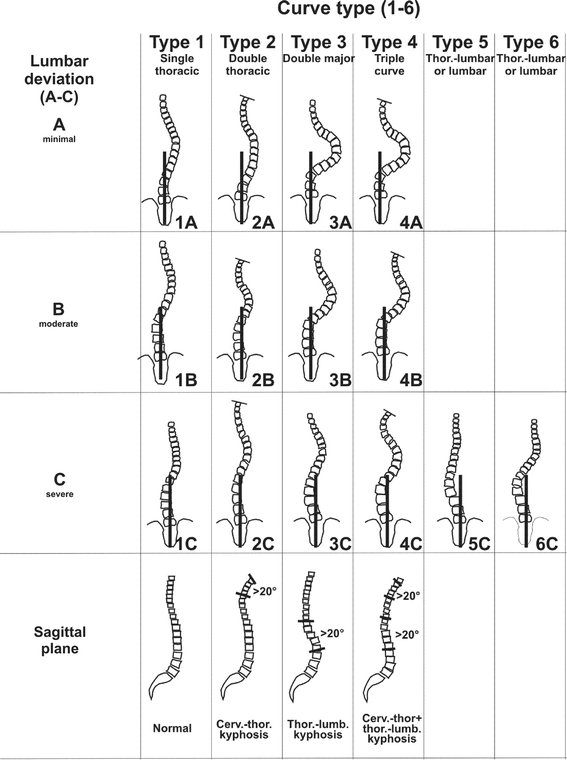
To these basic six curve types the lumbar spine modifier is added. This modifier is defined by the location of the CVSL on the apical vertebra of the lumbar curve. Lenke defined three lumbar modifiers: Modifier A: when the CSVL runs between the pedicles of the lumbar apical vertebra. Modifier B: when the CSVL runs between the medial border of the lumbar concave pedicle and the lateral margin of the apical vertebral body. Modifier C: when the CSVL falls completely medially to concave apical vertebra's body.
As mentioned, a thoracic sagittal profile modifier is also included in the Lenke classification. Thoracic kyphosis is measured between T5–T12 and defined as: + (plus): when thoracic kyphosis measures >40°. N (normal): when thoracic kyphosis measures between 10 and 40°. − (minus): when thoracic kyphosis measures <10°.
The Lenke classification showed higher inter and inta-reliability compared to the King classification [7]. It also provided a better and more reliable tool to assist surgeons in choosing the best method of treatment for each curve pattern. Lenke curves types 1 and 5 can be treated either anteriorly or posteriorly. Lenke types 2, 3, 4 and 6 should be treated completely posteriorly. In patients with lumbar modifiers A or B a selective thoracic fusion is advocated in order to avoid as much as possible the fusion of lumbar vertebrae.
Although the Lenke classification is more comprehensive and reliable than the King classification, it is still far from perfect. Surgeons still deviate 15 % of the time from the algorithm given for selecting fusion levels [8] and the classification failed to address the rotational component of the deformity. Recently, investigators offered stereoradiographic measurements of spinal deformity [9, 10]. The measurements utilized for the analysis were the Cobb angle, apical vertebra, axial rotation of the apical vertebra and the orientation of the apical vertebra with respect of the sagittal plane. This allows assessment of the deformity in the coronal, sagittal and axial planes. New technologies such as the EOS system, which provides 3D reconstruction of the spine may serve as a basis for a truly 3D classification of scoliosis as a basis for new concepts in therapeutic procedures [11].
Footnotes
Acknowledgments
The author thanks Prof. Fritz Hefti, Basel/Switzerland for having contributed both figures.