
Abstract
Abstract
Purpose
Temporary hemiepiphysiodesis has gained increasing popularity after the introduction of the eight-Plate Guided Growth System. Since its introduction, the eight-Plate has largely supplanted the traditional Blount staple. The eight-Plate offers better purchase in the bone and a more precise insertion technique. However, the Blount staple is less expensive than the various guided growth plates. Further, some surgeons feel that the Blount staple may work faster, making it more appropriate for children who are approaching skeletal maturity. Unfortunately, the original instrumentation and technique for inserting the Blount staple is over 50 years old and has not been updated.
Methods
The purpose of this study was to develop new instrumentation to make Blount staple insertion as accurate and minimally invasive as eight-Plate insertion. We developed wire/drill guides to accommodate all three sizes of the Blount staple. Two wires are inserted through the wire guide under image intensifier control. After confirming the accurate position of the guidewires, a 3.2-mm cannulated step drill is used to drill over the wires to a depth of 5 mm. This creates two pilot holes for the two tines of the Blount staple. The final insertion is guided under an anteroposterior image intensifier view. We also developed a small staple holder that permits insertion through a small incision.
Results
We developed a working prototype of the new instrumentation and used it in three clinical cases.
Conclusions
With the new staple inserter and instrumentation, Blount staples can now be inserted through a smaller incision with similar accuracy as eight-Plate insertion.
Keywords
Introduction
We developed new instrumentation that potentially allows for easier and more accurate Blount staple insertion through a smaller incision. Eidelman and D'Agostino [1] proposed a modified staple design for easier insertion, but our instrumentation is designed to work with the standard Blount staple. This technical note describes the new wire/drill guide, cannulated step drill, and staple inserter.
Epiphysiodesis is a simple way (compared to limb lengthening) to treat limb length discrepancy in growing children. Blount and Clarke [2] described stapling for epiphysiodesis to achieve correction of limb length discrepancy and Zuege et al. [3] described stapling for temporary hemiepiphysiodesis to achieve correction of angular deformities. For the last half of the twentieth century, the Blount staple (Zimmer, Warsaw, IN, USA) has been widely used to perform temporary hemiepiphysiodesis [3] or permanent epiphysiodesis [2]. The insertion instrumentation provided by Zimmer includes a bulky inserter that is wider than the largest Blount staple. Generally, a long (approximately 4 cm) incision is required for this standard inserter. The staple is positioned to straddle the physis, and this position is verified on the anteroposterior view of the image intensifier. However, there is no easy way to ensure correct placement (midway from front to back) in the sagittal view until after the staple has already been inserted. Staple placement that is too anterior or posterior may result in recurvatum or procurvatum deformity, respectively. The one-staple method has been described and has been proven to be effective [4]. However, some surgeons prefer to use two or three staples [5]. There is no consensus in the literature about the optimal number of Blount staples to be inserted for hemiepiphysiodesis or epiphysiodesis. The new instrumentation was designed so that a smaller incision can be used and the staple can be placed more accurately.
Surgical technique
We designed a slender inserter that securely clamps all three staple sizes (3/8, 5/8, and 7/8 inch) but is the width of only the smallest staple (Fig. 1). This inserter includes a removable back slapper extractor, if needed, for later removal of the staple (Fig. 1). To achieve a more accurate insertion, we also designed a new combined wire and drill guide for each of the three sizes of the Blount staple (Fig. 2). The wire guide allows the surgeon to position the two 1.5-mm guidewires at the same width as the two tines of the Blount staple. Then, the surgeon can check the precise position of the guidewires in both the frontal and sagittal planes with the image intensifier (Fig. 3). If necessary, the guidewires can be changed easily, without damaging the bone or the physis. The other end of the combined wire and drill guide is a drill guide for the insertion of a 3.2-mm-diameter cannulated step drill that is designed to drill the outer cortex of the bone to a depth of no more than 5 mm. The drill hole width of 3.2 mm is smaller than the width of the shoulder of the Blount staple (5 mm). The Blount staple can be locked in the inserter and the tines easily placed into the pre-drilled holes that are 3.2 mm wide and 5 mm deep (Fig. 4a). Then, the tilt of the staple can be adjusted on the anteroposterior view so that it is parallel to the growth plate in the frontal plane. After hammering the staple into the bone, anteroposterior and lateral image intensifier views are obtained as final documentation of the staple position (Fig. 4b, c).

New staple inserter is only as wide as the smallest Blount staple but still securely clamps all three staple sizes. The inserter can be combined, if needed, with a back slapper extractor for later removal of the Blount staple
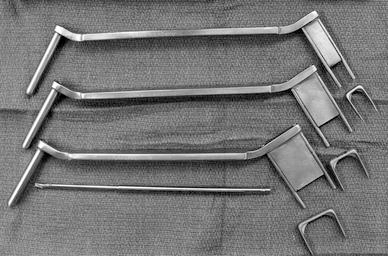
Combined wire and drill guide was designed to accommodate all three sizes (3/8, 5/8, and 7/8 inch) of the Blount staple. The 3.2-mm drill is designed as a step drill that reams the outer cortex of the bone to a depth of 5 mm
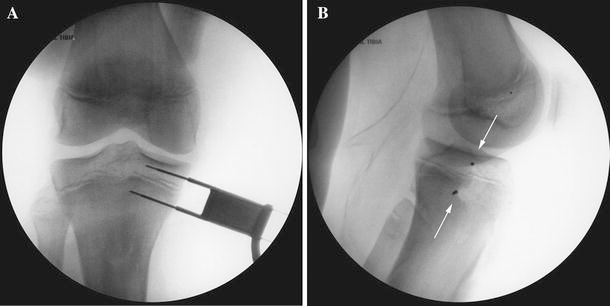
Intraoperative image intensifier view showing two guidewires inserted over the 5/8-inch wire guide on the anteroposterior (

Three patients (two 15-year-old boys and one 13-year-old girl) underwent treatment for genu valgum. The new instrumentation was used to insert a Blount staple in the distal femur or proximal tibia. The compact inserter made the staple placement easier and reduced the length of the skin incision to approximately 2.5 cm (Fig. 5).

Intraoperative photograph showing the difference in size between the original Zimmer staple inserter and our new inserter
Discussion
Recently, the eight-Plate Guided Growth System (Orthofix, Lewisville, TX, USA) [6–8] has largely replaced the Blount staple. The insertion instrumentation of this and other similar screw-plate devices allows a great degree of precision and represents one reason why many surgeons have switched from Blount staples to screw-plate devices [6–9]. However, eight-Plates are more expensive than Blount staples (approximately US $475 for an eight-Plate, screws, and guide pins compared with US $75 for a Blount staple). This is an especially important consideration in the developing world. With the new Blount staple insertion apparatus, insertion of the Blount staple becomes as accurate, simple, and minimally invasive as eight-Plate insertion. The screw-plate devices still have other important advantages over the Blount staple, particularly in young children in whom spontaneous Blount staple extrusion is a problem.
Some surgeons believe that staples work faster than screw-plate devices [10]. Others feel that the rate of correction with screw-plate devices is the same [5] or faster [6] than staples. While there may be some controversies, there still seems to be a role for the Blount staple in epiphysiodesis and hemiepiphysiodesis with the device's low cost and the potential for a more rapid correction. Given the continued market demand for the Blount staple, it would seem reasonable to have an improved insertion technique and instrument for more accurate placement through smaller incisions.
Footnotes
None of the authors received financial support for this study.
Acknowledgments
The authors want to thank A. Koromilas, SA, Athens, Greece, for manufacturing the prototype of our new instrumentation, and Amanda Chase, MA, and Alvien Lee for their invaluable assistance with the manuscript.