
Abstract
Abstract
Objective
To evaluate the clinical and functional results of a technical procedure used in the surgical treatment of congenital constriction ring (CCR) in children.
Materials and methods
This was a retrospective study undertaken to evaluate the results of surgical techniques performed from January 1995 to December 2005 on 95 patients with 134 congenital constriction bands. Due to the drop-out of nine patients during follow-up, data on 86 patients (121 congenital constriction rings; average age at surgery 1 year 2 months) were analyzed. The extent of the constrictions was classified by according to the Patterson criteria. All patients were treated by two-stage sine plasty combined with removal of the fibrous groove and fasciotomy, with one-half of the ring removed during the first stage and the other half removed 1 week later during the second state. The surgical outcomes were assess according to the Moses criteria.
Results
Three types of CCR (Patterson criteria) were identified among the 86 patients (121 constriction rings): types I (5 patients, 4.1 %), II (107, 88.5 %), III (9, 7.4 %). Of the 121 constriction rings, good results were attained in 73.6 % and fair results in 26.4 %. Sensory deficits were seen in six patients immediately after the surgery but all six had improved to a normal condition at the final follow-up examination. There were no skin necrosis or wound healing problems.
Conclusion
The combined sine plasty/removal of fibrous groove and fasciotomy method reported here is a simple and safe surgical technique for treating CCR in children.
Introduction
Amniotic constriction band, first described in 1832 by Montgomery [1], is one term used to describe a wide range of associated congenital anomalies, including anular constrictions of multiple extremities, oligodactyly, acrosyndactyly, talipes equinovarus, cleft lip and cleft palate, and hemangiomas. Additional, less common clinical manifestations include complete absence of the limb, short umbilical cord, craniofacial disruptions, neural tube defects, cranial defects, scoliosis, and body-wall defects, such as gastroschisis and extrathoracic heart. Some of these manifestations occur at birth at only a very low frequency because they result in spontaneous abortion [2–5].
The variability of presentation between patients, the unusual nature of this constellation of anomalies, and the lack of a consensus on etiology are all reflected in the fact that 34 different names have been used to describe this entity in the literature [6].
A number of techniques have been developed for the correction of congenital constriction rings (CCRs). To date, four techniques have been used for the correction of CCRs in one- or two-staged approaches, namely, historical multiple Z-plasty [7], W-plasty [8], the “Mutaf procedure” [9], and the replacment of Z-plasty with direct closure [10]. While many advances in different fields of reconstructive surgery are reported every day, surprisingly there has been no report in recent decades of a new technique for the correction of CCRs of the extremities.
Since 1995, we been developing and improving upon a method of skin plasty for the correction of CCRs in which the skin incision is performed at the constriction rings in sine manner. We have designated this technique “sine plasty.” In this article, we present this new surgical procedure and our clinical experience of 15 years with this procedure, with the aim of evaluating the long-term results of this technique.
Materials and methods
A retrospective study was undertaken to evaluate the results of surgical techniques performed from January 1995 to December 2005 in 95 patients with 134 congenital constriction bands. Data on nine patients (13 constriction bands) were not analyzed due to insufficient follow-up. The remaining 86 patients (121 constriction bands) formed the patient group of this study. The patient group comprised 51 female infants and 35 male infants, whose average age at surgery was 1 years and 2 months (range 4 days to 3 years).
All patients and their parents were questioned for pertinent facts of family history, neonatal, prenatal history, and existing impairment due to constriction rings. During the physical examination, we specifically noted deformities of the nails, accompanying anomalies, and circulatory and neural deficits. When the other opposite limb was normal, it was used for comparative measurements.
There is no widely accepted classification scheme for amniotic constriction band. In our assessment, we followed the Patterson classification for the common extremity manifestations [11]:
Type I includes extremities with simple constriction rings. There may be deficient subcutaneous tissue at the level of the ring, but the extremity distal to the ring is normal. Type II is a constriction ring with distal deformity, including atrophy and lymphedema. These findings are thought to represent lymphatic or neurovascular disruption caused by the ring. There may be sensory deficits, especially when rings occur at the proximal aspect of the extremity [12, 13]. Type III is acrosyndactyly, or fenestrated syndactyly, which is a distal cutaneous fusion of the skin with separation of the digits proximally. This differs from typical or developmental syndactyly, which results when normal interdigital cell death does not occur during hand development and which always involves the proximal web. Short digits are commonly noted in infants with acrosyndactyly, in contrast to the normal-length digits that are seen in most infants with developmental syndactyly. Type IV includes amputation at any level of the extremity or digit.
Timing for surgical repair
Surgery was indicated once the cases were identified.
Surgical technique
After general anesthesia is administered and the tourniquet applied, we use loupe magnification. First, the joints are placed in a neutral position and the two proximal, distal skin edges of the constriction band pulled close together. The position of the incision is then marked (Fig. 1a), and a perpendicular incision is made through the skin to fibrous band and fascia (Fig. 1b, c). The constricted area must be meticulously and carefully dissected to avoid damaging the underlying neurovasculature. A fasciotomy is performed after the excision of all fibrotic tissue, with separation of the subcutanous layer from fascia for 1.5 cm on both sides (Fig. 1d). Direct closure is completed without fascia suture (Fig. 1d), which allows the fatty tissue to naturally reposition itself under the skin. For wound closure, we use a 4-0 Monocryl suture (Ethicon, Johnson & Johnson, Somerville, NJ) in the deep layer and a 5-0 Monocryl suture in the subcutaneous layer.
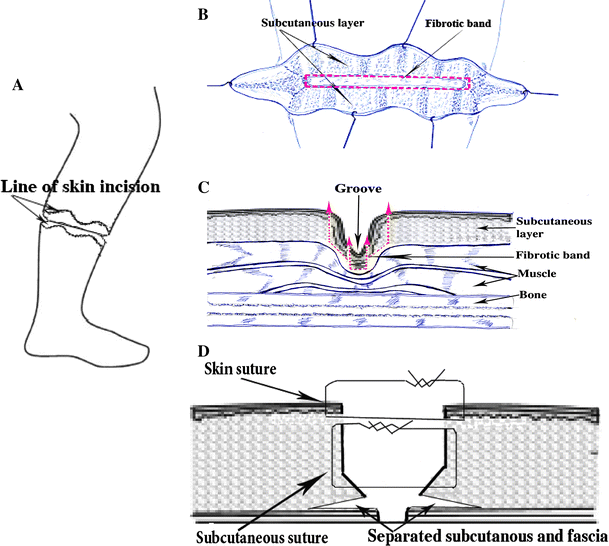
A two-stage correction approach was used in all cases, with one-half of the circumference excised during the first operation and the other half excised 7 days thereafter. This approach avoids any problems to the distal circulation in the limb, which might already be compromised. Lymphedema, when present, significantly improves within a few weeks following the first surgery.
Post-surgical care
Postoperatively, the limb is placed in a plaster splint and a neutral position. Approximately 3 weeks after the sine plasty surgery, the plaster splint is removed and the extremity can move freely.
Follow-up
Patients were re-examined postoperatively at 3 and 6 weeks, 3 and 6 months, 1 year, and every year thereafter. We recorded the results of surgery based on function, clinical evidence or recurrence, appearance, and improvement of preoperative symptoms according to Moses criteria [14]: A good result meant no functional loss, no cosmetic deformity, no recurrence, and a decrease in the extent of edema or cyanosis, if present. A fair result meant little or no functional loss, mild cosmetic deformity, and slight recurrence of the ring, but improvement in circulatory signs (if they were present). A poor result meant a noticeable functional deficit, a cosmetic deformity (scarring), a definite recurrence of the ring, and no change in symptoms.
Results
The average follow-up was 7 years 9 months (range 2 years 9 months to 15 years 7 months). We found no family history of ring constrictions, but five male and seven female patients had a positive family history for other anomalies.
There was a high incidence of CCRs in first pregnancies (39 patients), and premature birth was noted for 11 patients. However, no significant relationship could be demonstrated between the anomalies and drug ingestion, maternal illness (such as viral infections during the first trimester), ohigohydramnios, or polyhydramnios. The mother was ≤24 years of age in 42 cases, and in 39 of these cases the patient was the first-born child.
Deformities of the nails consistently resulted when the bands were located below the wrist or ankle. Forty-nine patients, all with distal bands, had abnormalities of the nails; of these 49 patients, 37 had hypoplastic nails while in the remaining 11 patients this abnormality was absent (see Tables 1, 2).
Position of constriction band in extremity is often combined with constriction band in another position
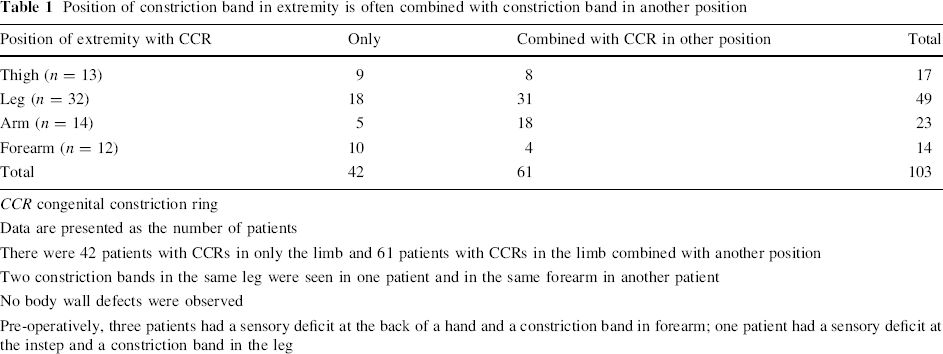
CCR congenital constriction ring
Data are presented as the number of patients
There were 42 patients with CCRs in only the limb and 61 patients with CCRs in the limb combined with another position
Two constriction bands in the same leg were seen in one patient and in the same forearm in another patient
No body wall defects were observed
Pre-operatively, three patients had a sensory deficit at the back of a hand and a constriction band in forearm; one patient had a sensory deficit at the instep and a constriction band in the leg
Congenital constriction rings only in the hand or foot
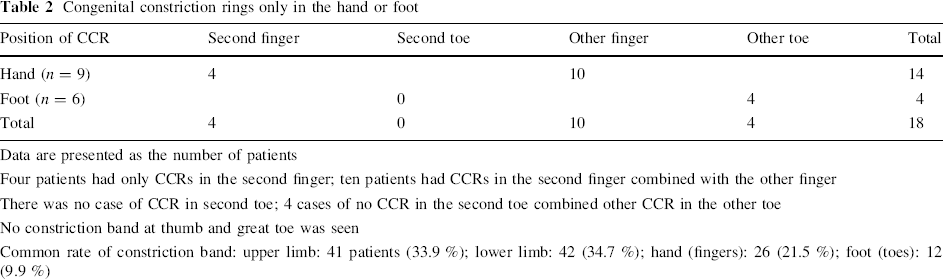
Data are presented as the number of patients
Four patients had only CCRs in the second finger; ten patients had CCRs in the second finger combined with the other finger
There was no case of CCR in second toe; 4 cases of no CCR in the second toe combined other CCR in the other toe
No constriction band at thumb and great toe was seen
Common rate of constriction band: upper limb: 41 patients (33.9 %); lower limb: 42 (34.7 %); hand (fingers): 26 (21.5 %); foot (toes): 12 (9.9 %)
Sensory deficits
Pre-operatively, there were four patients with sensory deficits: three with a sensory deficit at the back of a hand and a constriction band in the forearm, and one with a sensory deficit at the instep and a constriction band in the leg.
Associated anomalies
All patients demonstrated at least one other developmental anomaly. Forty-one patients (48.8 %) had hand abnormalities (syndactyly, acrosyndactylt, hypoplastic phalanges, camptodactyly, brachyclactyly, symbrachydactyly, electrosyndactyly); 31 (38.3 %) had foot abnormalities (club foot, hypoplasia of phalanx or brachydactyly, syndactyly, metatarsus adductus, pes planus); seven (8.6 %) had oral cavity deformities (cleft palpate, high palpate); two (1.1 %) had cardiovascular abnormalities (patel ductus arteriosus); seven (3.9 %) had other abnormalities (kyphoscoliosis, hemangioma, mental retardation, cerebral palsy). The most frequent combination was syndactyly of the hand and club-foot deformity (21 patients, 24.4 %).
Position of extremity with constriction band
The extent of the constrictions according to the Patterson classification [15] was (121 CCRs):
05 (4.1 %) 107 (88.5 %) 9 (7.4 %) 0
Postoperative results
The average follow-up was 7 years 9 months (range 2 years 9 months to 15 years 7 months). The surgical results according to the Moses criteria [14] were: 89 (73.6 %) 32 (26.4 %) 0
Complications
Postoperatively, sensory deficits were seen in six patients. Of these; three had sensory deficits at the back of a hand with a forearm constriction band, two had sensory deficits at the2 instep with a leg constriction band, and one had a sensory deficit at the toes with a leg constriction band.
Preoperatively, four patients had sensory deficits due to the distal constriction band (back forearm in 1 patient, lower one-third leg in 1 patient, second finger in 1 patient).
At the final follow-up examination, of these four patients within preoperative sensory deficits, three patients were improved. The fourth patient showed no sensory improvement. This patient had a constriction band in the leg and had been operated on at age 11 months. At the final follow-up examination (4 years 7 months after sine plasty surgery) the sensory deficit remained at the instep.
Six patients developed postoperative sensory deficits at the distal constriction band (back forearm in 2 patients, mild one-third leg in 1 patient, lower one-third leg in 2 patients, third toe in 1 patient). By the time of the final follow-up examination, all patients had fully recovered (see Table 3).
Improvement of the sensory deficits with correction of the distal constriction band
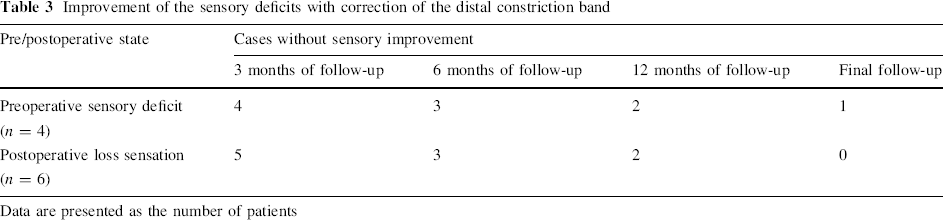
Data are presented as the number of patients
Other complications
No patient showed skin necrosis or margin of skin, and no patient developed an infection
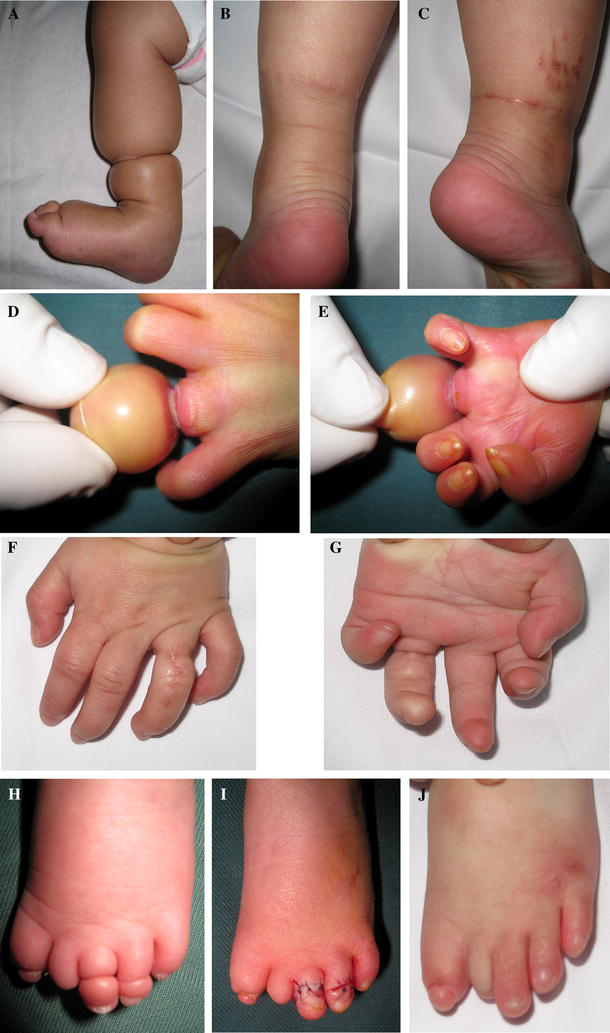
By completion of surgery, a normal extremity contour was obtained in all patients. There was no patient with circulatory compromise or edema postoperatively. The wounds healed uneventfully in all patients with minimal scar formation and complete elimination of the contour deformity, and without hourglass deformity (Figs. 2, 3, 4, 5).
Lower limb:
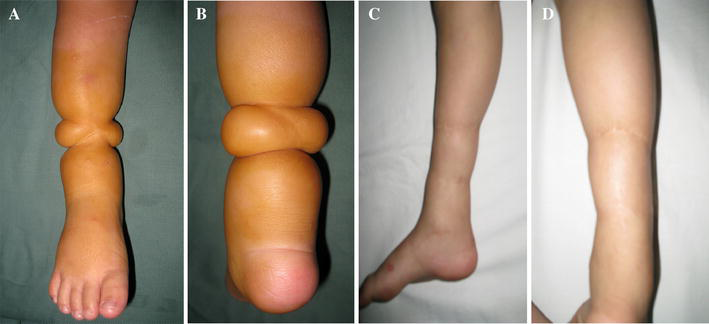
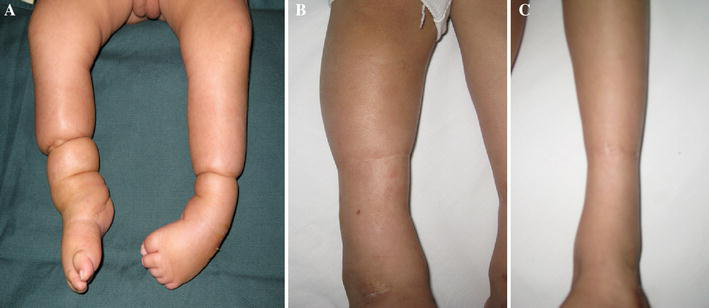
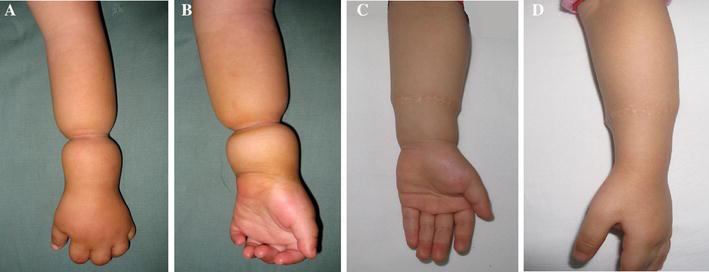
Illustrative cases
Case 1
Case 2
Case 3
Case 4
Discussion
Surgical technique
Timing for surgery
The timing for surgical management of constriction rings ranges from in utero surgery to urgent postnatal surgery to multiple-stage reconstructive surgeries beginning later in life. In utero surgery requires that the constrictions be properly diagnosed by ultrasound and be considered severe enough as to be threatening limb or fetal survival. After birth, however, surgical repair is the indicated intervention for correction of a constriction ring. Because both dysfunction and deformity are characteristics of CCR limbs, treatment is aimed at both functional and aesthetic improvements [16]. Swollen lymphedematous tissue is most easily decompressed during infancy because it has not been indurated by scar tissue [17, 18]. More complex and multi-staged procedures are by necessity delayed until the surgeon is more comfortable with the apparent size and function of the pertinent structures. Nevertheless, all major reconstructive work, according to Upton, should be completed by school age, with simultaneous hand and foot procedures best performed before the child begins to walk [19].
In accordance with Streeter's guidelines [20], all our patients were operated on immediately to save the limb functions from being damaged due to circulatory compromise. For the five type I cases, we initiated the intervention for cosmetic reasons.
The technique of sine plasty
Several principles are central in surgical correction. For example, the depth of the groove should be completely excised and replaced with normal skin flaps, and local tissue should be defatted and advanced into the defect to correct the ultimate contour deficiency [18]. Additional approaches to the reconstruction of the affected digits include toe-to-hand transfers and distraction osteogenesis.
In addition to creating a very noticeable aesthetic deformity, CCR may cause circulatory compromise, leading to lymphedema and amputations. Correction of CCR is therefore needed for aesthetic and functional reasons. Despite the many advances in reconstructive surgery during the previous century, a literature review revealed that only four techniques (multiple Z-plasty [7], W-plasty [8], Mutaf and Sunay [21], and Z-plasty with direct closure [10]) have been standardly used for decades to correct this anomaly. We consider that a basic requirement in the correction of CCR is providing a normal extremity contour with an acceptable scar. However, these four techniques are not effective in eliminating the contour deformity in severe cases, and they often result in bad scarring. The sandglass deformity, which is a result of subcutaneous tissue deficiency under the constriction ring, persists either a short or long time after these techniques have been used. To achieve a normal extremity contour in the correction of CCR, soft tissue deficiency under the constriction ring needs to be replaced with a like tissue. To this end, in our technique, we separate the subcutanous layer from fascia to produce a potential space that can later be refilled with a soft tissue bracelet; this approach helps to reduce the superficial sandglass deformity in an efficient manner. Moreover, the use of sine plasty techniques allows placement of the incision lines parallel to the relaxed skin tension lines, and these incisional scars are remarkably improved over the scars resulting from the previous Z-plasty procedures (Fig. 6a–c). On the one hand, incisions are longer along the sine line, which helps to compensate further the skin constriction; on the other hand, the scars look nicer than those resulting from Z-plasty or Mutaf plasty. Even in severe CCRs, we observed a normal extremity growth in all of our patients after surgery, implying that this new technique does provide a well-vascularized soft tissue padding that relieves the chronic pressure over the underlying neurovascular structures and might have a positive effect on extremity growth over the long term.
Comparative schematic views of three techniques
Comparative schematic views of the resultant scar formation after the classic Z-plasty technique, Mutaf technique, and sine plasty technique are shown in Fig. 6a–c.
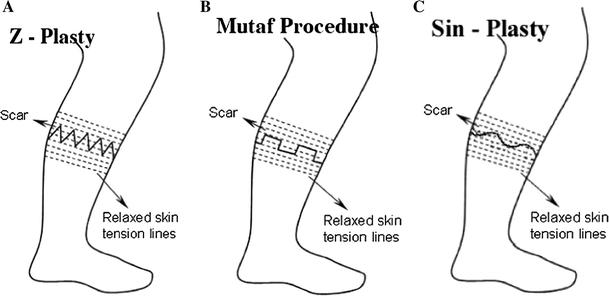
It should be noted that the major limbs of sine plasty are aligned to be parallel with the relaxed skin tension lines, whereas all limbs of the multiple Z-plasty scar are obliquely crossing these lines, while with the Mutaf technique, the major limbs remain crossing relaxed skin tension lines. In the sine plasty technique, all limbs of the scar are parallel relaxed skin tension lines.
Several reports of a one-stage release for circumferential constriction bands have appeared in the plastic surgery literature. Hall et al. [19] describe the circumferential release of a deep constriction ring in the wrist of a neonate. Di Meo and Mercer [22] report the results of one-stage correction of circumferential constriction bands in four patients, the ages of whom ranged from 17 days to 7 months. Muguti [23] describes the findings in two infants, 5 days and 5 weeks old, respectively. In our study, our youngest patient for CCR was 4 days old.
Should corrections for CCR be performed using a one-stage or multi-staged approach?
Constriction rings are released in two to three stages to prevent the appearance of vascular complications in the distal parts. This concept, first propagated by Stevensons [7], is advocated by many surgeons [12, 15, 24–29]. However, several reports of the one-stage release of a congenital constriction band have been reported in the literature [8, 19, 22, 23, 30, 31] with good outcomes.
Studies on the circulation to the skin flaps [32] have found that the blood supply to the skin is primarily from the musculocutaneous arteries that directly penetrate the subcutaneous and cutaneous tissue from underlying muscles. This observation provides very important support to single-stage contracture release as it confirms that there will be no wound healing problems and venous obstruction. To the contrary, removal of band actually facilitates blood circulation to muscles in a severely involved limb.
The sine plasty technique involves the two-stage release of the congenital constriction band, with a 1-week interval between stages. This approach has proved to be safe without any necrosis and healing problems. Deep vessels are not damaged by our surgical procedures.
The pathologic tissue is typically friable and attached to the skin and subcutaneous tissue and must be removed in its entirety (Fig. 1b, c). In some cases, the band may extend through the underlying fascia and muscle, even to the periosteum of the underlying bone [19]. Fasciotomy should be considered only if the compartmental pressure remains persistently elevated [33]. However, we performed fasciotomy for all CCR to create free muscle or tendon so that the underlying muscle or fascia could fill the defect.
Complication
The surgical repair of constriction bands is associated with complications similar to those associated with other hand surgeries, including infection, maceration, and graft loss due to inadequate immobilization, combined with flap necrosis and distal digital ischemia due to circulatory compromise. Further complications, including sensory loss, contractures, and/or immobility, are difficult to identify as they also may be due to the initial insult caused by the constriction band.
Although most constriction rings are superficial, the depth is maximal on the dorsal surfaces, especially on those of the hand and wrist [17, 34, 35] The depth of the groove may vary from a partial defect with a mild deficiency of subcutaneous tissue to a deep circumferential indentation interrupting veins, lymphatic channels, tendons, and even nerves [29] in the case of a complete constriction band occurring with or without distal swelling or lymphedema [17]. The greater the involvement of the palmar surface of the extremity, the greater the potential is for neurovascular compromise and tendon involvement. The lack of predilection for dorsal surface involvement in the arm or axillary regions can more often result in severe distal neurovascular and lymphatic compromise, including palsies and sensory deficits [17].
In our sine plasty approach, the incision in the skin perpendicular to the fibrous band and fascia and the constricted area must be meticulously and carefully dissected to avoid damaging the underlying neurovasculature. Postoperatively, there were six patients (6.9 %) with sensory deficits due to the distal constriction band. However all six patients had fully recovered by the time of the final follow-up examination.
Conclusion
The correction of CCR by sine plasty combined with removing fibrous groove and fasciotomy in two stages (1-week interval between stages) is simple, safe, and effective in the treatment of CCR in children without any major complications.